Management of FAP and HNPCC
advertisement

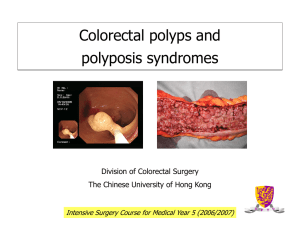
MANAGEMENT OF FAP AND HNPCC Dr. J. Northover These two dominantly inherited conditions are the cause of around 5% of cases of colorectal cancer in the US and the European Union. They produce considerable challenges in management, and provide important insights into the pathogenesis of colorectal cancer. Making the diagnosis FAP was characterised in the 1920s, and presents an unmistakable clinical picture. With 100% penetrance, the pattern of inheritance is easily recognised; in most cases rectoscopy reveals that the rectum contains large numbers of adenomas; cancer occurs frequently in their 30s and 40s in untreated individuals. Most have other minor features such as epidermoid cysts, dental cysts and retinal pigmentation. More significantly in terms of morbidity and mortality, around 12% harbour desmoid tumours and 90% have duodenal adenomas; in the latter group, cancer develops in a significant proportion. HNPCC, another dominantly inherited single gene abnormality, was not recognised reliably until Lynch described two apparently different conditions (families exhibiting either colon cancer alone [‘Lynch I’] or in pedigrees including gynaecological and other cancers [‘Lynch II]) in the 1960s. With only 80% penetrance, with few patients developing multiple adenomas, and with none of the ‘tell-tale’ features that facilitate the diagnosis in FAP, this condition is more difficult to recognise, and hence more difficult to manage. Opportunities in management arising from molecular diagnosis The faulty gene causing FAP was localised on chromosome 5 in 1987, and identified precisely (‘cloned’) in the early 90s. The FAP gene is very large, and the mutation can affect any part of it. Finding the precise site of mutation in a particular individual is a long and laborious task, but once located it can be looked for much more quickly in other family members. Previously we had to rely on sigmoidoscopy and the identification of adenomas as evidence of inheritance, performed regularly for many years before an individual can be said with confidence not to have inherited FAP. Today molecular diagnosis can be used instead in families in which the mutation has been identified; at any stage, including in utero if needed, inheritance can be predicted by this method. In HNPCC the situation is much more complicated; first of all there are at least four genes which may be mutated in this condition, though only one will be affected in any individual pedigree. Second, HNPCC cannot be excluded if the pedigree suggests dominant inheritance, but no mutation is identified in these four genes. Finally, as there is incomplete penetrance, even if inheritance is demonstrated by identification of a mutation, the individual may never develop the condition. Finding affected individuals In FAP adenomas usually begin to develop in the large bowel in the early teens. Those at risk of inheritance are straightforwardly the children of anyone affected by FAP - 50% are likely to develop the condition. The traditional approach to identification was yearly rectoscopy from around age 14, continuing either until adenomas are seen (leading to prophylactic surgery) or until age 35, when it is normally assumed that inheritance has not occurred if the rectum remains normal; in our experience at St Mark’s the rectum is always affected, making simple rigid rectoscopy the diagnostic tool. As indicated above, molecular diagnosis has largely supplanted this practice, allowing inheritance status to be determined in the teens, and those who have not inherited being discharged from follow-up. In HNPCC, even identification of those at risk for inheritance may be difficult. Those with two first degree relatives who have had bowel cancer, or the close relatives of anyone developing bowel cancer before age 45 are at significant risk, and should be offered colonoscopic surveillance; more limited endoscopy is not enough. As the age of appearance of phenotypic abnormalities is variable, three yearly colonoscopy should be instituted from age 25, and continued for life. If other cancer sites have occurred in the pedigree, surveillance of other organs, particularly the pelvis by endosonography, is necessary. Surgery in affected individuals Affected individuals without cancer In FAP, cancer rarely occurs before age 20, but almost always before age 40. In those identified through early examination, prophylactic surgery can be offered, diminishing the colorectal cancer risk by a factor of 8. The preferred procedure at St Mark’s is total colectomy and ileorectal anastomosis; after this procedure, which has the advantages of simplicity and good postoperative function, the patient needs to attend six monthly for life to check on the state of the rectum. Proctocolectomy and ileal pouch-anal anastomosis is used in some circunstances, particularly those with dense rectal polyps, and in those thought likely to default from regular follow-up examination; it can also be used in those in whom the rectum later becomes densely populated by adenomas, or if severe dysplasia or malignancy supervene. In an HNPCC-affected individual, regular surveillance colonoscopy and polypectomy is suitable prophylaxis in most cases, though multiple polyps, particularly if they are sessile or severely dysplastic, may warrant surgery; in such cases the procedures offered are the same as those used in FAP. Affected individuals with cancer If cancer has developed, whether the underlying diagnosis is FAP or HNPCC, and assuming that radical removal of the primary tumour is feasible, the segmental resection that would be sufficient in sporadic cancers is not enough. Total colectomy should be recommended, while in those with rectal cancer, the oncologically appropriate rectal procedure is added also. Management of lesions outside the large bowel In FAP patients, this includes the management of desmoid tumours and upper GI malignancies, while in HNPCC there are ovarian, uterine, stomach and urothelial tumours to consider. In the short time available for this lecture, these issues will not be covered in detail.