Rheumatology 6 – Clinical Features of Osteoarthritis
advertisement

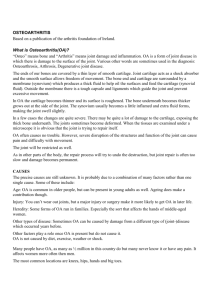
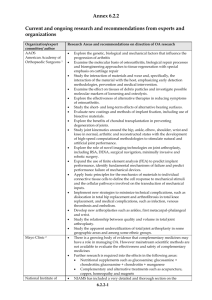
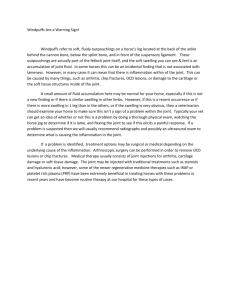
Rheumatology 6 - Clinical Features of Osteoarthritis Anil Chopra 1. 2. 3. 4. 5. Describe the causal factors of osteoarthritis Outline the general symptoms of arthritis Have a basic understanding of how to examine joints. List at least 3 radiological features helpful in the diagnosis of osteoarthritis Outline the diagnosis and treatment of osteoarthritis Osteoarthritis is a disease of cartilage not of bone. It is caused by: – Breakdown of proteoglycans and collagen – Change in water content – thinning and fibrillation of cartilage (where the cartilage has more fibrous as opposed to smooth structure) This results in bony changes (sclerosis and osteophytes) and is not related to osteoporosis. They occur as the body tries to compensate for loss of cartilage Risk factors for the development of osteoarthritis include: • Increasing age • Genetics • Joint damage – Obesity (weight bearing joints) – Congenital dysplasia (hips) – Sports injuries (knees) – Surgery (meniscectomy) – Previous rheumatoid arthritis as joint will be damaged. Osteoarthritis is not the same as ageing, it is a metabolic process Osteoarthritis Ageing - Increased cartilage Hydration - Decreased cartilage hydration - Decreased proteoglycan - Constant proteoglycans - Decreased collagen - Constant collagen - Increased chondrocytes proliferation - Constant chondrocytes proliferation - Increased metabolic activity - Constant metabolic activity - Increased sub-chondral bone thickness - Normal sub-chondral bone thickness Pathogenesis of Osteoarthritis The breakdown of proteoglycans caused by age and trauma has a number of effects. Early Changes: – Swelling of cartilage – Loosening of collagen framework – Chondrocytes increase proteoglycan synthesis but also release degradative enzymes – Increased water content Later Changes: – Proteoglycan broken down faster than produced – Cartilage thins and softens with fissuring and cracking – Repair attempted but inadequate – Bone exposed – Remodelling and hypertrophy of subchondral bone Healthy cartilage The diagram above is a representation of what healthy cartilage looks like (in terms of its structure). The proteoglycan contains many side chains and is very sulphated. This makes the proteoglycans extremely hydroscopic (i.e. they take up lots of water). This gives the cartilage huge tensile strength – the structure is very strong mainly due to the water content of it, and this is due to the hydroscopic nature of the proteoglycans involved. The diagram below shows the effect of trauma on the cartilage matrix. As you can see, trauma to the matrix induces the release of growth factors from the matrix which in turn cause release of metalloproteinases (from chondrocytes) which cause rapid joint destruction via collagen and proteoglycan breakdown in the cartilage of the joint. Unhealthy Cartilage in OA In OA, the proteoglycans (which are a key part of the normal structure) break down and become fragmented, and therefore, the water content of the cartilage diminishes. As a result, the collagen (supporting network) also degenerates. This causes the cartilage to thin, and as a result, the bones are able to get closer together – in some extreme cases, they may touch and rub together – this will cause pain in the joints, and as the osteophytes generate more bone to compensate for the cartilage lost, the condition worsens. This diagram shows the secondary effects of cartilage matrix breakdown. The cartilage has already started to degenerate, and at the centre of all of the action are chondrocytes. The chondrocytes release metalloproteinases which activate the synoviocytes to release pro-inflammatory cytokines and synovial fluid. The cytokines mediate the inflammation of arthritis and the release of synovial fluid and also inflammatory response will cause local swelling (oedema). Epidemiology • Aged 50, 50% population have OA on X-ray. • Aged 65, 90% have OA but only 5-10% symptomatic. Other rheumatic diseases (inflammation of the synovial membrane) are more disabling. – Rheumatoid arthritis ~ 1% (peak onset 45-55) – Reactive arthritis ~ 1% (peak onset 25-35) Diagnosis of Osteoarthritis It is characterised by joint pain, especially distal inter-phalangeal joints, carpometacarpal joint, hips or knees. It can cause knees to be: Valgus: outward angulation of the distal bone i.e. tibia is turned outward in relation to the femur, resulting in a knock-kneed appearance. Varus: inward angulation of a distal bone i.e. the tibia is turned inward in relation to the femur. Symptoms Pain experienced worsens upon using the joint affected. Swelling that may be present is usually hard (as it is caused by proliferation of bone and cartilage around the joint margins). Effusion (fluid leak into the joint) due to secondary synovitis is common. It mostly affects large joints. There is stiffness… – Morning stiffness – in OA it lasts for less than an hour (remember in RA it lasts for more than an hour). – Evening stiffness which mostly occurs after use of the joints (for example exercise, or continuous use during the day (such as at work) and relaxation in the evening (at home) may lead to joint stiffness). There is also joint deformity due to cartilage loss. The risk of development can be increased by past history of injury or surgery, playing traumatic sports, hip dysplasias and family history. Examinations Upon general examination, look for patients weight and fat proportion. The joints should then be examined by looking, feeling and moving. Hands • LOOK. – Redness – Pattern of joint involvement – Heberden’s and Bouchard’s nodes – Squaring of hand (CMC) – Joint deformities (varus or valgus) • FEEL. – bony swelling • MOVE – Crepitus: (cracking or grinding sound as bones rub) Particularly CMC joint Knee • LOOK – Quads wasting – Valgus or varus deformity – Gait • FEEL – Joint effusion – Bony swelling • MOVE – Crepitus – Reduced range of movement – Lateral instability Neck • LOOK – Kyphosis or scoliosis • FEEL – local tenderness • MOVE – Reduced range of movement • Neurological examination of the arms is important as many of the nerves that control arm movements run through the root of the neck and so the risk of compressing these nerves in spinal OA. Hip • • • LOOK – usually nothing visible – Gait Feel – Tenderness over the joint (mid-point inguinal ligament) Move – Reduced range of movement (particularly rotation in flexion) The differential diagnosis for osteoarthritis: • Presence of: – Heberden’s nodes – Squaring of the hand and CMC crepitus – Quad wasting, bony swelling and crepitus of the knee. Sometimes valgus or varus deformity. – Pain on movement of the hip • Absence of (compared to RA or reactive arthritis) – Warm joints – Soft tissue swelling – Large effusions Investigations • Blood – – • X-ray – – – – ESR and CRP normal ANA (antinuclear antibodies) and Rheumatoid factor are negative Joint space narrowed Periarticular sclerosis Osteophytes (Subchondral cysts may be seen) Treatment • Reassurance – they do not have rheumatoid arthritis • Lose weight to aid weight bearing joits • Physiotherapy – To increase muscle tone – Quads exercises in quad wasting • Analgesics, NSAIDs (COX-2 inhibitors) • Intra-articular steroids to reduce inflammation and swelling • Support devices and footwear • Surgery