Preventive maintenance and timely repair of assistive technology
advertisement

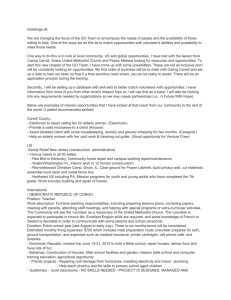
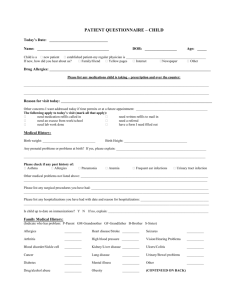
Preventive maintenance and timely repair of assistive technology (AT) is essential to people requiring AT to obtain and maintain employment, and to contribute as independent members of society. Various stakeholders – users, vendors, funding agencies and healthcare practitioners have repeatedly expressed concerns regarding the current process. However, a thorough literature review of disability and rehabilitation issues reveals that there has been no recent study on the maintenance and repair of assistive technology devices, even though several articles mention that it is a serious issue and merits further research. The purpose of our project is to study the current process of maintenance and repair of assistive technology devices, identify areas of concern, and find possible methods to improve the current system. Therefore, as part of our initial research effort, we organized the first symposium Perspectives on Maintenance and Repair of Assistive Technology – on November 9, 2004. There were two overall objectives for the symposium. The first was to learn the specific experiences, activities and responsibilities for each of the groups that is involved with maintenance and repair of AT. Panelists focused particularly on devices that enhance mobility. The second objective was for each of the constituencies to identify specific issues or problems (from the perspective of the specific constituency) that affected the maintenance and repair process. The groups that were identified as central to the issue of maintenance and repair of assistive technology mobility devices included: Users of assistive technology Durable medical equipment repair and maintenance providers Insurance and health maintenance organizations Government support agencies Healthcare practitioners We present below a summary of the issues highlighted at the symposium. Summary of Experiences, Activities, and Responsibilities USERS User experiences with maintenance and repair related at the Symposium can be summarized by the following list: Lengthy time for repairs (more than 1 month for simple repairs such as tire replacement) Confusion about repair process o What is the process? o Who is involved? o Who pays for what? Lack of back-up equipment when repair is lengthy Problems with equipment on delivery common, particularly because of model changes in AT which do not work with other AT in use. For example, a change in wheelchair model may mean that the tie down system used in the user’s van may not work without modification Travel problems common, particularly when traveling via commercial airplane Lack of familiarity of technicians with specific equipment Lack of preventive maintenance Lack of emergency service Limited choices for repair Finally, users felt that in addition to the DME providers, consumer experience and review could be an important source of information regarding choice of appropriate AT. Such review is currently lacking in any organized fashion. DURABLE MEDICAL EQUIPMENT PROVIDERS Durable Medical Equipment (DME) provider experience with maintenance and repair of AT can be summarized as follows: Reimbursement rates from Medicaid and private insurance companies do not cover expenses incurred by the DME in providing the repair service Number of repairs needed versus the ability of the DME to complete repairs means that repairs have to be prioritized based on the medical needs of the user Complexity and time delays associated with approval process from agencies providing reimbursement for repair services Need for back-up equipment, however, no support for it Lack of consistency among different manufacturers Difficulty with repair because of individualization and customization of wheelchairs HEALTHCARE PRACTITIONERS Healthcare Practitioners experience with maintenance and repair of AT include: Lack of understanding by consumers of need to consider multiple sources for support of AT Insufficient funds to cover needed activity Lack of standardization of insurance policies Fragmentation in current system Delays from requirement for a physician’s signature on justification letter Therapists often in advocacy role for user INSURANCE AND GOVERNMENT SUPPORT AGENCIES Insurance company and government support agency experience with maintenance and repair includes: Insurance companies face problems with misunderstandings of what AT is “medical necessary” versus AT that will facilitate activities of daily living Confusion because law does not mandate that insurance providers must provide AT Lack of understanding of process by consumers Differences in level for prior authorizations Summary of Issues Identified with Current Maintenance and Repair Process Shown in Table 1 below is a tabulation of the issues that were identified from each of the different constituents. As illustrated, each of the constituent groups identified issues with the complexity of the current system. For example, all groups indicated that the Prior Authorization (PA) approval process needed to be improved. The time necessary to complete repairs was also identified as an issue by all constituents. Procurement of parts is a problem for both the user and DMERP. Again, the time necessary for approval was identified as an issue by all groups. The DMERP and Organizations providing funding for maintenance and repair identified user abuse as an issue. All parties identified lack of emergency services as a problem. Users and the healthcare practitioners identified lack of back-up equipment as a significant issue. The DMERP indicated that they would provide back-up equipment if funds existed for support of back-up equipment. Lack of preventive maintenance was identified as a problem by users and the DMERPs. Lack of manufacturing standards and means of independent equipment evaluation was cited by all groups. And finally, users indicated that independent repair facilities, not direct equipment providers, was an issue. Constituent Issues Identified A. COMPLEXITY 1. Paperwork 2. PA and Approval 3. Funding structure 4. Number of steps 5. Inability to understand system B. TIME 1. Time to bring chair for assessment 2. PA and Approval 3. Procurement of Parts 4. Time to complete repair C. USER ABUSE OF EQUIPMENT D. EMERGENCY SERVICES E. LACK OF LOANER EQUIPMENT F. LACK OF PREVENTIVE MAINTENANCE G. LACK OF MANUFACTURING STANDARDS H. LACK OF CONSUMER REPORTS I. LACK OF INDEPENDENT REPAIR FACILITIES Users DMERP Organizations Providing Funding for Maintenance and Repair Healthcare Practitioners √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ Would provide if adequate funding available √ √ √ √ √ √ √ √ Table 1: Issues with the current system for maintenance and repair √ √ √ √ The symposium provided us with enough material to start our research. The primary issues identified were thoroughly researched and our findings are presented below. A. COMPLEXITY : Funding Process for Repair of Durable Medical Equipment As mentioned earlier, each stakeholder agreed that more than one of the elements of the funding process is a pressing concern. We were unable to find any study on the subject. And, have tried to outline the basic steps that need to be followed without getting into the details of each subset of funding agencies that may be involved. However, it is useful to keep in mind that each step outlined could have compounding time effect if more than one agency has to approve the application. The following flow-charts indicate how a user addresses his need for repair of AT device. Problem with AT Device Select Appropriate Durable Medical Equipment Repair Provider (DMERP) Identification of problem by vendor along with user Verify whether qualify for funding based on the eligibility criterion and the exclusions list of insurance providers Prepare a funding request Apply for Prior Authorization PA Denied Follow Appeal Process PA Denied Do not need Prior Authorization PA Approved Get Repairs for AT Device PA Approved 1 1 Procedure codes with the "RP" modifier do not require prior authorization (PA) if all of the following are true: The DME is more than one year old. Claims submitted with the "RP" modifier without PA during the first year will be denied. The charge for the repair parts is $50.00 or less. Wisconsin Medicaid purchased the DME being repaired. Check which agencies are willing to provide funds and how much of the total expenses they will cover Private Medicaid Medicare Medicaid Private Medicare Medicaid 2 2 Out-of-pocket payments are not possible if the user is covered by Medicaid which is the funding agency of last resort. Further, with more than one funding agency picking up the bill, there could be a cascading effect. Prepare a Funding Request Determine if Prior Authorization needed PA: Applicable to Medicaid for repair costs greater than $49.99 in uncoded HCPC parts or for repair requiring greater than 5 units of labor Can back-date the PA and go through with repairs No PA: Applicable to Medicaid for repair costs less than $49.99 in uncoded HCPC parts and requiring less than 5 units of labor Also to Medicare and Private insurance for all repairs I II I Process I: Requires PA Applicable to Medicaid for repair costs greater than $49.99 in uncoded HCPC parts or repair requiring greater than 5 units of labor (i) Certificate of Medical Necessity (CMN): Valid referral or prescription from your primary physician or primary care provider to establish medical necessity, Or a form provided by DME company that is to be signed by the physician Medicaid validity : 6 months (ii) Submission of eligibility documents, CMN and funding request by vendor with valid ID to Medicaid Submission by fax or web options available XX * Time limits may vary from one insurance provider to another XX Contd.. PA process Medicaid time limit for decision – 10 days from the time a consultant gets it This does not include mail time, lag in attending to the request etc. so 30-45 days is a reasonable estimate for response time PA approved (iii) Initial Denial: If the PA is denied May be asked to submit missing documentation or further clarification Reconsideration: May resubmit the PA for reconsideration based on additional documentation (not submitted in the initial PA request) Approved Not Approved B A B Process (iv): File a written request for an Administrative Law Judge hearing (ALJ) to ask for a review of the funding denial decision Time limit for request - 60 days after decision Time limit for decision - no time limit, a fair estimate is that the hearing will be held six to nine months after the request is filed, and the decision will be issued two to three months later. Monetary threshold in dispute - $100 or more Submit justification letter and certificate of medical necessity Additional documents or oral statements at the hearing can be submitted A favorable decision is a reasonable expectation Approved A Not approved C C Process (iv): Request review by the Departmental Appeal Board Time limit for request - 60 days after ALJ decision Time limit for decision - no time limit, Expect about six to nine months or longer Monetary threshold in dispute - $100 or more Advocate or attorney will submit a memorandum of law explaining why the ALJ decision is incorrect Unless some significant new fact or circumstance arises, no opportunity to submit new information at this level of appeal. Approved Not approved A D 3 D Process (v): Final Appeal :Request for judicial review Time limit for request – 60 days after DAB decision Time limit for decision - no time limit, Monetary threshold in dispute - $1000 or more Approved A 3 Not approved Notified of denial in writing The closest paper that we could find on the subject was Parsons (1991) which discusses that this “complex adjudication mechanism consumes a great deal of time…On average, an individual who pursued all internal appeal mechanisms faced an internal processing delay of approximately 10.4 months in 1982. It is important to point out that this lag does not include the applicant's own response lags at the various stages…Of those who were initially denied in 1978, 41.7 percent appealed the decision. Of appellants The other possibility is a process that does not need a PA. II Process II: PA not required: (Less than $50 for Medicaid) Following documents needed: HIPAA form Rx form CMN for certain coded parts under Medicare Submission of above-mentioned documents by vendor If there is an assigned code for the part required, then follow corresponding Medicare/ Medicaid guidelines A A Vendor carries out repair work Vendor submits reimbursement request Reimbursed by Medicaid / Medicare / Private Insurance company / co-payment as the case may be Notification process Medicaid: No notification provided Medicare: Notified after billing submission Private insurance companies: Mostly notification provided denied eligibility at the “reconsideration” stage, almost half (48.0 percent) appealed to the administrativelaw-judge level.” B. TIME: Repair Process and Employment Outcomes: Fishman (1991) points out that “Developments in information technologies and assistive devices have enabled people with disabilities to engage in work that they could not have done in the past, as well as created new types of jobs that some people with disabilities are capable of performing.” There is consensus among writers in the field as well as attendees of the seminar that delays in repair of AT devices inhibit users from being able to carry out their daily activities and work. Thus, we are conducting an empirical study of the effects of the current AT maintenance and repair system on employment outcomes of users. Our literature review guided us that “…the type of disability that appears to be driving the observed overall decline in real wages of disabled workers relative to nondisabled, post-ADA, is musculoskeletal. The real wages of workers with musculoskeletal disabilities declined 4 percent more than for workers without disabilities post-ADA…” (Hotchkiss, 2003). Also, Stern (1996) explains that “programs that affect the supply index of disabled people are much more efficient than those that equally affect the demand index for disabled people”. Therefore, decreasing missed days of work due to inefficiencies in maintenance and repair would contribute to increasing the labor supply of disabled persons. Lower absenteeism also increases the value of disabled persons to employers. Another paper by Oi (1996) suggests that greater customization of AT devices is likely to boost labor supply in two ways: increasing daily time available for both work and leisure as well as reducing disability specific work inconvenience. The following chart captures the inter-relationship between repair of AT devices and employment outcomes. Repair & Labor Long and highly variable absence Direct employer costs: turnover, replacement workers, other absenteeism costs Direct employee cost: Lost wages Fewer job opportunities and self selection Indirect employee cost: Lower wages offered Long and highly variable repair times Public insurance AT repair Lower employment and income of disabled persons Estimates We examine two measures of potential gains to be made through improving employment outcomes of the disabled population: 1. Lost wages due to absence 2. Lower income and employment We use the U.S. Census Bureau, 2000 Census of Population and Housing, 1% Public Use Microdata Sample. And, classify individuals in the following categories: • General Population : Persons without any physical disability • Population with Disability: All individuals who answered YES to the following two questions: Does this person have any of the following long-lasting conditions: A condition that substantially limits one or more basic physical activities such as walking, climbing stairs, reaching, lifting, or carrying? Because of a physical, mental, or emotional condition lasting 6 months or more, does this person have any difficulty in doing any of the following activities: (Answer if this person is 16 YEARS OLD OR OVER.) Working at a job or business? We summarize our methodology and findings here. We sorted the census data by age, income and population. 1. Used ‘typical’ hourly wage by age for each population sub-group: Found that if 10% of the individuals in the disability group miss work due to AT repair, the direct cost in terms of lost wages was $14 million per day in 1999. 2. Used ‘typical income gains’ resulting from reduced ‘employment gap’: Found that the annual US gains would be $10 million for every 1% reduction in the employment gap. However, these are merely preliminary estimates and we have no data on the number of days that a person with work and physical disability misses on average. Therefore, our next step is to conduct a national survey to answer these questions. The Mobility Device Repair Survey: Individuals with Disabilities is an ambitious project of our research team that aims to gather data that can be used for further analysis of the specific problems that users face when obtaining repairs for AT devices. The survey questions can be broadly separated into the following categories: 1. questions related to the time component of repair 2. questions related to funding of the repair 3. questions related to impact of AT problems on user’s activities especially work 4. questions related to user’s feedback on the current AT repair system 5. demographic information of the user We are posting the survey on various bulletin boards on the internet and also contacting various independent living centers across the country. We expect to have the survey responses collected within the next three months. After that we plan to analyze the results so that we can get a deeper understanding of the issues involved and consequently make informed progress towards finding solutions o the current shortcomings. References: • • • • Fishman, Michael E., Framing the Issues: Economic Research on Employment Policy for People with Disabilities, Employment and Disability Institute Collection, Cornell University, October 1999. Hotchkiss, Julie L., The Labor Market Experience of Workers with Disabilities: The ADA and Beyond, W.E. Upjohn Institute for Employment Research, Kalamazoo, Michigan, 2003. Oi, Walter Y., Employment and Benefits for People with Diverse Disabilities.” in Disability, Work and Cash Benefits, ed. by Jerry L. Mashaw, Virginia Reno, Richard V. Burkhauser, and Monroe Berkowitz, Kalamazoo: W.E. Upjohn Institute for Employment Research, 1996. Parsons, Donald O., The Health and Earnings of Rejected Disability Insurance Applicants: Comment, The American Economic Review, vol. 81, no. 5, Dec. 1991, 1419-1426.