Clinical Summary
advertisement

Thrombosed portal vein aneurysm
Author(s)
Belo-Oliveira P, Rodrigues H, Belo-Soares P, Teixeira L, Caseiro-Alves F
Patient
female, 74 year(s)
Clinical Summary
A 74-year-old woman, previously healthy, presented with right upper quadrant pain. She
had no history of trauma, surgery, biopsy, or known hepatic disease. On physical
examination
she
had
mild
tenderness
in
the
right
upper
quadrant,
without
hepatosplenomegaly or palpable abdominal masses. Laboratory analyses including liverassociated enzymes were within normal limits.
Clinical History and Imaging Procedures
A 74-year-old woman, previously healthy, presented with right upper quadrant pain. She
had no history of trauma, surgery, biopsy, or known hepatic disease. On physical
examination
she
had
mild
tenderness
in
the
right
upper
quadrant,
without
hepatosplenomegaly or palpable abdominal masses. Laboratory analyses including liverassociated enzymes were within normal limits. A work-up was initiated with an abdominal
ultrasound that identified a mass, measuring 5.3x4.3cm, near the hilum of the liver, with
posterior acoustic enhancement compatible with cystic areas within the lesion. Colour
Doppler ultrasound examination revealed absence of flow within this mass. Normal
continuous nonpulsatile monophasic wave-form, with hepatopetal flow, was detected at the
left and right portal vein. No portal vein trunk was identified. An ecoendoscopy suggested
that the cystic lesion was probably in the head of the pancreas. The abdominal helical
computed tomography examination confirmed the presence of the mass at the hepatic
hilum, and the contrast enhanced images showed a beaded appearance at the porta hepatis,
compatible with a cavernomatous transformation of the portal vein. In the records of the
patient there was a previous CT examination, done six months earlier that showed an
aneurismal dilatation of the main portal vein showing homogeneous enhancement equal to
the left and right portal vein, thus confirming the diagnosis of a thrombosed portal vein
aneurysm with cavernomatous transformation. Attending to the patient’s age and the lack
of major complications the patient was submitted to conservative management with close
follow-up.
Discussion
Portal vein aneurysm (PVA) is defined as a focal dilatation of the portal venous system that
assumes a fusiform or saccular configuration. The first report of an extrahepatic portal vein
aneurysm was done in 1956 by Barziali e Kleckner. For a long time PVA was considered to
be a rare lesion. However, this opinion has largely been altered by the increasing number of
new cases published in recent years. The main explanation for this renewed appears to be
the increasing availability and use of non-invasive imaging modalities. In particular the
more widespread use of ultrasonography and Doppler ultrasound might have increased the
diagnosis rate of this entity. The origin of PVA remains unclear and has widely been
discussed. Some authors have suggested that portal hypertension causes PVA secondary to
the increased intraluminal pressure on the relatively thin portal vein wall. Histological
examination reveals a decrease in the number and size of muscle and elastic fibers within
the vessel wall, and fragmentation of the internal elastic lamella with replacement by
fibrous connective tissue. Other conditions which have been proposed as possible etiologies
include trauma and pancreatitis. In recent years the role of congenital factors has been
gaining popularity. The clinical significance of PVA is related to their size: small
aneurysms commonly are asymptomatic; large aneurysms have been found to cause
duodenal compression, common bile duct obstruction, chronic portal hypertension, and
complete occlusion of the portal vein by recurrent thrombosis, symptoms of acute portal
hypertension, rupture, and recurrent or cramping abdominal pain. The prevalence of serious
complications appears to be low. The PVA is frequently identified with ultrasound or
Doppler ultrasound and confirmed with computed tomography. On sonography, PVA
appear as an anechoic, fusiform, or saccular structure. Colour Doppler ultrasound has been
considered a very accurate tool for the diagnosis of PVA, which shows colour flow within
the lesion unless it contains thrombus. Computed tomography shows a well-circumscribed,
markedly enhancing mass communicating with the portal vein. At magnetic resonance PVA
is hypointense on T1-weighted images and hyperintense or with heterogeneous signal
intensity on T2-weighted images. Portography or contrast angiography is considered a
complementary procedure necessary only when surgical intervention is planned. There is
some controversy about treatment, because some complications have been reported. In
asymptomatic patients without evidence of portal hypertension or cirrhosis, an aneurysm is
expected not to grow and conservative management with close follow-up is recommended.
Surgical treatment of PVA depends on the size, symptoms, complications, and clinical
condition of the patient. Surgical interventions include aneurysmorrhaphy, or portocaval
shunt. In summary, PVA is being diagnosed more frequently. Patients are likely to present
with right upper quadrant pain. However, PVA can be discovered during evaluation of
other abdominal processes. Non-invasive diagnostic modalities such as ultrasound colour
Doppler ultrasound, computed tomography, and magnetic resonance can enable the
diagnosis of this entity due to its vascular nature. Treatment should be based primarily on
the clinical presentation of the patient.
Final Diagnosis
Thrombosed portal vein aneurysm
MeSH
1. Liver Diseases [C06.552]
References
1. [1]
Portal vein aneurysm: report of two cases. Mhanna T, Bernard P, Pilleul F,
Partensky C Hepatogastroenterology. 2004 Jul-Aug;51(58):1162-4
2. [2]
Acute thrombosis of a portal vein aneurysm and development. Kim J, Kim MJ,
Song SY, Kim JH, Lim JS, Oh YT, Kim KW Clin Radiol. 2004 Jul;59(7):631-3
3. [3]
Acute thrombosis of a giant portal venous aneurysm: value of colour Doppler
sonography. Santana P, Jeffrey RB Jr, Bastidas A J Ultrasound Med. 2002
Jun;21(6):701-4
4. [4]
Congenital and acquired anomalies of the portal venous system. Gallego C, Velasco
M, Marcuello P, Tejedor D, De Campo L, Friera A Radiographics. 2002 JanFeb;22(1):141-59
5. [5]
Extrahepatic portal vein aneurysm: a case report and review of the literature. Lau H,
Chew DK, Belkin M Cardiovasc Surg. 2002 Feb;10(1):58-61
Citation
Belo-Oliveira P, Rodrigues H, Belo-Soares P, Teixeira L, Caseiro-Alves F (2006, Feb 3).
Thrombosed portal vein aneurysm, {Online}.
URL: http://www.eurorad.org/case.php?id=3822
DOI: 10.1594/EURORAD/CASE.3822
To top
Published 03.02.2006
DOI 10.1594/EURORAD/CASE.3822
Section Liver, Biliary System, Pancreas, Spleen
Case-Type Clinical Case
Views 26
Language(s)
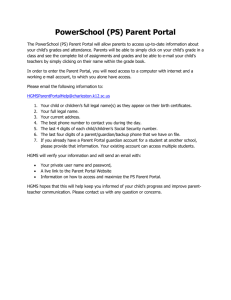
Figure 1
abdominal ultrasonography
ultrasonography showing a hypoechoic mass near the hilum of the liver, with posterior
acoustic enhancement compatible with cystic areas within the lesion
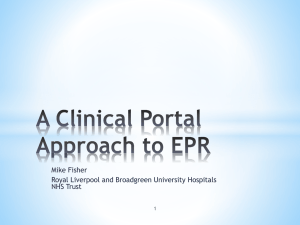
Figure 2
Abdominal ultrasound
ultrasonography showing a hypoechoic mass, measuring 5.3x4.3cm, near the hilum of the
liver, with posterior acoustic enhancement compatible with cystic areas within
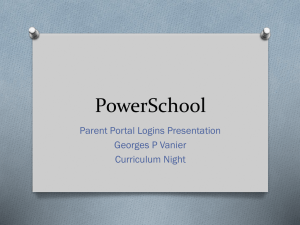
Figure 3
Color Doppler
Colour Doppler ultrasound examination showing absent flow within this mass
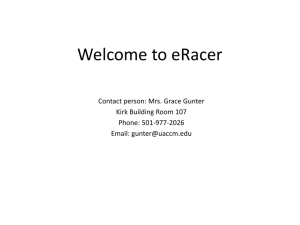
Figure 4
Spectral Doppler
Spectral Doppler ultrasound showing no pulses within the mass
Figure 5
Spectral Doppler
Spectral Doppler ultrasound showing normal continuous nonpulsatile monophasic waveform at the left and right portal vein
Figure 6
Endoscopic ultrasonography
Ecoendoscopy showing the cystic nature of the mass
Figure 7
Abdominal CT
Unenhanced abdominal CT showing a mass in the right upper quadrant near the hepatic
hilum (arrow)
Figure 8
Contrast enhanced abdominal CT
Contrast enhanced abdominal CT, portal phase, showing the thrombosed portal vein
aneurysm (arrow), with a cavernomatous transformation of the portal vein (small arrows).
The thrombus is nicely demonstrated in the splenic vein, near the confluence...
Figure 9
Contrast enhanced abdominal CT
Contrast enhanced abdominal CT, portal phase, done six months earlier showing an
aneurismal dilatation of the main portal vein (arrow) showing homogeneous enhancement
equal to the left and right portal vein branches
Figure 10
Contrast enhanced abdominal CT
Contrast enhanced abdominal CT, portal phase, done six months earlier showing an
aneurismal dilatation of the main portal vein (arrow) showing homogeneous enhancement
equal to the left and right portal vein branches
Figure 1
abdominal ultrasonography
ultrasonography showing a hypoechoic mass near the hilum of the liver, with posterior
acoustic enhancement compatible with cystic areas within the lesion
Figure 2
Abdominal ultrasound
ultrasonography showing a hypoechoic mass, measuring 5.3x4.3cm, near the hilum of the
liver, with posterior acoustic enhancement compatible with cystic areas within
Figure 3
Color Doppler
Colour Doppler ultrasound examination showing absent flow within this mass
Figure 4
Spectral Doppler
Spectral Doppler ultrasound showing no pulses within the mass
Figure 5
Spectral Doppler
Spectral Doppler ultrasound showing normal continuous nonpulsatile monophasic waveform at the left and right portal vein
Figure 6
Endoscopic ultrasonography
Ecoendoscopy showing the cystic nature of the mass
Figure 7
Abdominal CT
Unenhanced abdominal CT showing a mass in the right upper quadrant near the hepatic
hilum (arrow)
Figure 8
Contrast enhanced abdominal CT
Contrast enhanced abdominal CT, portal phase, showing the thrombosed portal vein
aneurysm (arrow), with a cavernomatous transformation of the portal vein (small arrows).
The thrombus is nicely demonstrated in the splenic vein, near the confluence (arrowhead)
Figure 9
Contrast enhanced abdominal CT
Contrast enhanced abdominal CT, portal phase, done six months earlier showing an
aneurismal dilatation of the main portal vein (arrow) showing homogeneous enhancement
equal to the left and right portal vein branches
Figure 10
Contrast enhanced abdominal CT
Contrast enhanced abdominal CT, portal phase, done six months earlier showing an
aneurismal dilatation of the main portal vein (arrow) showing homogeneous enhancement
equal to the left and right portal vein branches
To top
Home Search History FAQ Contact Disclaimer Imprint