RESEARCH PROPOSAL - Document Server

TYPES AND PREVALENCE OF BIRTH DEFECTS
AMONG BABIES BORN TO MOTHERS ON ARV
DRUGS AND THEIR COUNTER-PARTS IN
MBARARA, UGANDA.
BY
DR. NTUUYO FRED
MBChB, MSc. Anat (MUST)
SUPERVISOR
--------------------------------------------
A research proposal written as a requirement for PhD research in human anatomy
March 2010
1
TABLE OF CONTENTS
TITLE …………………………………………………………………….... 1
TABLE OF CONTENTS …………………………………………………. 2
ACRONYMS USED ……….……………………………………………….4
ABSTRACT ………………………………………………………………. 5
CHAPTER 1 : INTRODUCTION ……………………………………….... 6
1.1: Background ………………………………………………….…..6
1.1.1: Genetic factors ………………………………………... 7
1.1.2: Twinning ……………………………….……………... 8
1.1.3: Environmental factors ……………….……………….... 8
1.2: Types of ARV drugs .................................................................. 10
1.2.1: NRTIs ……………………………………………… 11
1.2.2: NNRTIs ……………………………………………. 12
1.2.3: Protease Inhibitors……………………………….….. 12
1.2.4: Entry/Fusion Inhibitors………………………….….... 12
1.2.5: Integrase Inhibitors …………………………….…….. 13
1.3: History of HAART and PMTCT………………….……………13
1.4: Statement of the problem ……………………….……………. 15
1.5: Research Significance…………………………….…….……... 15
1.6: General Objective…………………………………………….. 16
1.7: Specific Objectives …………………………………………… 16
1.8: Hypothesis …………………………………………………..… 16
1.9. Conceptual Framework ………………………………… …… 17
CHAPTER 2: LITERATURE REVIEW ………………………………… 18
CHAPTER 3: RESEARCH METHODOLOGY…………………………. 23
3.1: Study Subjects/Area of study ………………..………………. 23
2
3.2: Research Design/Data collection…….……............................... 24
3.3: Data analysis and Presentation................................................... 26
REFERENCES ………………………………………….………………....27
Appendix i: RESEARCH QUESTIONNAIRE ……………………………32
Appendix ii: RESEARCH BUDGET ……………………….……………. 45
Appendix iii: RESEARCH TIME FRAME ……………………………… 46
3
ACRONYMS USED
HAART – Highly Active Anti-Retroviral Therapy
HIV – Human Immunodeficiency Virus
ART – Anti Retroviral Therapy
ARV – Anti-Retroviral
NRTIs – Nucleotide/Nucleoside Reverse Transcriptase Inhibitors.
DNA- Deoxyribonucleic Acid
NNRTIs – Non Nucleoside Reverse Transcriptase Inhibitors
PI – Protease Inhibitor(s)
PMTCT - Prevention of Mother To Child Transmission (of HIV)
AZT - 3’-Azido-3’-deoxythymidine or Zidovudine d4T - 2’, 3’-didehydro-3’-deoxythymidine or Stavudine
3TC - 2’-deoxy-3’thiacytidine or Lamivudine gp41 - Glycoprotein 41
CCR5 - Chemokine Receptor 5
CD4 – Cluster of Differentiation 4
WHO - World Health Organisation et al.
- and others
MRRH - Mbarara Regional Referral Hospital
ISS - Immune Suppression Syndrome
MJAP - Mulago Mbarara Joint AIDS Program
TASO - The AIDS Support Organisation i.e. - that is to say e.g. - for example
CDC - Centers for Disease Control and prevention
4
ABSTRACT
Birth defects are the structural, behavioral, functional and metabolic disorders that a baby may have at birth. Several birth defects are reported nowadays by the media, causes of which are obscure. In literature, 40-60% cases of birth defects occur due to completely unknown causes.
Environmental factors, genetic disorders and twinning are the known causes of birth defects. Drugs such as Thalidomide were confirmed in the early
1940s to be among the environmental teratogens. Today, use of
Antiretroviral therapy in pregnancy as HAART or as dual therapy for
PMTCT still poses debate on the safety of the ARV drugs to the embryo/foetus. In the developed world, safety profiles of ARV drugs to the embryo/foetus have been studied and reported. In addition, birth defects registries for the general population have been established. This has not been done in Uganda. This research will endeavor to bridge these gaps for our population. A survey will hence be conducted among mothers not on ARV therapy to establish the types and prevalence of birth defects among their offsprings. Simultaneously, a similar survey will be conducted among mothers on ARV drugs for HAART or dual therapy for PMTCT.
5
CHAPTER ONE
INTRODUCTION
1.1
Background
Birth defects are the structural, behavioral, functional and metabolic disorders that a baby may have at birth (Sadler, 2004). Major structural anomalies occur in 4-6% of live born babies and are the leading cause of infant mortality, accounting for about 25% of infant deaths, not discriminating on racial grounds (Moore et al ., 1998). Till the 1940s, it was believed that the human embryo developed in an impervious maternal uterus. It was as such protected from environmental hazards, drugs inclusive, by the amnion and chorion. Hereditary factors were hence thought to be the primary cause of congenital anomalies (Sadler, 2004). This was challenged when Gregg (1941) discovered that rubella, an environmental agent, affecting a mother during early pregnancy could cause cataracts, heart and ear defects in the foetus. The importance of environmental factors in causation of congenital anomalies thus became prudent.
The observations of Lenz (1961) and McBride (1961) focused attention on drugs as teratogens. They documented severe limb anomalies and other disruptions caused by thalidomide, a drug which was used in early pregnancy to control nausea. Sadler (2005) also documented a variety of limb defects caused by the drug. These included amelia, meromelia and phocomelia.
Although the cause of birth defects is still not known in 40-60% of cases, it has been established that several factors can cause or predispose the embryo
6
to acquisition of an anomaly/anomalies. The known factors are grouped into; genetic/chromosomal disorders accounting for 15% of birth defects; environmental factors accounting for 10% of the defects; and twinning associated with 0.5-1% of the defects (Sadler, 2005).
1.1.1 Genetic factors (Anonymous, 2006).
Genes are packaged in chromosomes to direct the growth, development and maintenance of both physical and biochemical systems. Errors/mutations alter the structure of the genes/chromosomes to cause congenital anomalies of the newborn. Common examples of such anomalies are the Marfan syndrome, Tay Sachs disease and Cri-du-chat syndrome.
The normal human chromosomal constitution is 22 pairs of autosomes and one pair of sex chromosomes. Any deviation from this number forms a numerical chromosome anomaly. Non-disjunction of chromosomes during meiosis and or mitosis is the cause of the observed aneuploidy. Nondisjunction affects both autosomes and sex chromosomes. Down’s syndrome
(Mongolism) is an anomaly caused by non-disjunction of the 21 st pair of autosomes. The offspring thus has an extra chromosome at position 21, a condition termed Trisomy 21. In Klinefelter and triple X syndromes, nondisjunction of the sex chromosomes occurs so that the offspring carries an extra X-chromosome hence XXY and XXX respectively. On the contrary, there may be absence of one of the sex chromosomes as in Turner’s syndrome i.e. XO (Sadler, 1995).
7
1.1.2. Twinning (Sadler, 1995)
Identical twins are formed by splitting of the zygote into two independent cell masses which develop to form two embryos. If it occurs in later stages of development, splitting may be incomplete in the axial area of the germ disc. This results in formation of conjoined twins.
Twin transfusion occurs in 5-15% of monochorionic monozygotic twins so that one twin receives most of the blood flow. The compromised twin is smaller, with death of both twins in 60-100% of cases.
1.1.3. Environmental factors (Sadler, 1995)
Environmental substances/factors which can cause birth defects are called teratogens. Wilson (1959) formulated the principles of teratology which determine the capacity of an agent to produce a birth defect. These are:
1 Susceptibility to teratogenesis depends on the genotype of the conceptus and the manner in which the genetic composition interacts with the adverse environmental factors
2 Susceptibility to teratogens varies with the developmental stage of the conceptus at the time of exposure. The most sensitive period for inducing birth defects is the 3 rd to 8 th weeks of gestation. This is known as the period of embryogenesis or organogenesis.
3 Manifestations of abnormal development depend on the dose and duration of exposure to the teratogen.
4 Teratogens act in specific mechanisms on the developing cells and tissues to initiate sequences of abnormal development.
5 Manifestations of abnormal development are functional
8
disorders, growth retardation, malformation and death.
Environmental teratogens are grouped into infectious agents, radiations, hormones, maternal disease, chemical agents and drugs. Infectious agents include viruses like Rubella, spirochaetes like Treponema pallidum and protozoa such as Toxoplasma gondii .
Ionising radiations e.g. X-rays subjected to pregnant mothers in heavy doses, can cause microcephaly, skull defects and spina bifida in the baby. Among the pregnant women who survived the atomic bomb explosions of
Hiroshima and Nagasaki, 28% aborted, 25% of the babies born died in their first year of life while 25% of those who lived had anomalies of their central nervous system e.g. mental retardation.
Diethyl stilbesterol is a synthetic oestrogen which was used in the 1940s and
1950s to prevent abortion. Its use was discontinued in 1971 after associating it with cancer of the vagina and cervix, among girls borne to mothers who had used the drug during pregnancy.
Several maternal diseases can have grave effects on the embryo/foetus.
Infants of mothers with Phenylalanine hydroxylase deficiency, are at risk of mental retardation, cardiac defects and microcephaly due to the high serum phenylalanine concentration. Diabetes Mellitus, Iodine deficiency and anaemia are other examples of maternal diseases of teratogenic importance.
Lead and mercury are examples of naturally occurring teratogens in the environment. Lead was associated with neurological disorders, growth
9
retardation and increased rates of abortions. Mercury caused multiple neurological disorders similar to cerebral palsy. Pesticides, insecticides and herbicides are teratogenic chemicals regularly used in homes.
Among drugs, are the pharmaceutical products and traditional medicinal herbs. The effects of thalidomide have been cited above. Angiotensin
Converting Enzyme inhibitors, e.g. Lisinopril, are known to cause growth retardation, foetal renal dysfunction and death. Valproic acid, an anticonvulsant, produces neural tube defects. Anti-neoplastic drugs and some antibiotics are known teratogens. Efavirenz, an ARV drug, is contraindicated in pregnancy for fear of its teratogenic potential.
Observations are still ongoing on the safety of other ARV drugs.
1.2. Types of ARV Drugs
There are currently five major classes of ARV drugs i.e. NRTIs, NNRTIs,
PIs, Entry/Fusion Inhibitors and Integrase Inhibitors (Finkel et al., 2009).
10
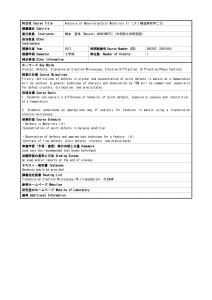
Figure 1: The life cycle of HIV.
The red text are the sites of action of the various ARV drugs (Furtado et al., 1999).
1.2.1.
NRTIs
Nucleoside and Nucleotide Reverse Transcriptase Inhibitors are analogues of native ribosides. They all lack the 3’ hydroxyl group. In the cells, they are phosphorylated to the corresponding triphosphate analogue which is preferentially incorporated into the viral DNA by the viral Reverse
11
Transcriptase enzyme. Due to absence of the 3’ hydroxyl group, a 3’-5’phosphodiester bond between the incoming nucleoside triphosphate and the growing DNA chain cannot be formed. Viral DNA chain elongation is thus terminated (Finkel et al.
, 2009). Examples of NRTIs are AZT, d4T, 3TC,
Didanosine, Tenofovir, Emitricitabine and Abacavir (Rang et al., 2007).
1.2.2.
NNRTIs
NNRTIs are non competitive inhibitors of the HIV 1 Reverse Transcriptase enzyme which do not require activation by cellular enzymes. They act by binding at a site adjacent to the active site of HIV 1 Reverse Transcriptase to induce conformational changes which result in enzyme inhibition. Four
NNRTIs are available for treatment of HIV 1 infection i.e. Nevirapine,
Efavirenz, Delavirdine and Entravine (Finkel et al., 2009).
1.2.3.
Protease Inhibitors
These are the inhibitors of the HIV Aspartyl Protease, the enzyme responsible for cleavage of the viral polyprotein into the essential enzymes
(Reverse Transcriptase, Protease and Integrase) and several structural proteins (Finkel et al., 2009). PIs bind to the active site of the enzyme to prevent maturation of the viral particles which leads to production of non infectious virions. Examples of PIs are Lopinavir, Nelfinavir, Retonavir,
Indinavir and Saquinavir (Walker Roger and Clive Edwards, 2003).
1.2.4.
Entry/Fusion Inhibitors
To enter the host cell, the membrane of the HIV virus must fuse with that of the former. Such fusion is accompanied by changes in the conformation of the viral transmembrane glycoprotein gp41. Enfuvirtide, a 36-aminoacid
12
peptide, binds to gp41 to prevent the conformational change. This leads to failure of viral entry into the host cell. (Finkel et al., 2009).
Maraviroc, a Chemokine Receptor antagonist, is an orally available Entry
Inhibitor which blocks the CCR5 co-receptor. The CCR5 co-receptor works in conjunction with the gp41 to facilitate HIV entry into the host cell.
(Finkel et al., 2009).
1.2.5.
Integrase Inhibitors
Integrase Inhibitors bind to the viral enzyme Integrase to prevent incorporation of the reverse transcribed HIV DNA into the host cell DNA.
Raltegravir is the first Integrase Inhibitor.
1.3. History of ART and PMTCT
3’-Azido-3’-deoxythymidine (AZT/Zidovudine) was approved in 1987 as the first ARV drug (Finkel et al., 2009). AZT showed significant reduction in mortality among patients with advanced HIV 1 infection with a parallel rise in CD4 lymphocyte count. The NRTIs Zalcitabine and Didanosine that followed AZT were initially used almost exclusively as mono-therapy for patients who were either intolerant or had AZT treatment failure.
In 1991-93, NNRTIs were introduced but were challenged by the extremely rapid appearance of viral drug resistance. Various clinical trials revealed that therapy with two NRTIs (dual therapy) was superior to mono-therapy in halting viral replication and restoration of the CD4 lymphocyte count.
Lamivudine, the negative enantiomer of 2’-deoxy-3’thiacytidine, and 2’, 3’didehydro-3’-deoxythymidine (d4T) were formulated.
13
In 1995, HIV 1 Protease Inhibitors were developed. The availability of HIV
1 RNA assays led to a better understanding of viral dynamics hence the advent of better ARV drugs, including PIs, led to a quantum leap in the treatment of HIV 1 infection. Use of three drugs (Triple therapy) i.e. two
NRTIs and a PI proved superior to the dual therapy. Triple therapy was subsequently adopted as the standard of care.
It was later demonstrated that, if NNRTIs were used with a potent combination of drugs (NRTIs) to cause suppression of viral replication to minimal levels, development of resistance to the former could be prevented.
Subsequently, proof emerged that a combination of two NRTIs and a
NNRTI was a potent alternative to two NRTIs and a PI. To this day, use of two NRTIs and a NNRTI or a PI is the standard therapy.
The WHO (2007) issued recommendations for the use of ARV drugs in pregnancy for PMTCT. Over time, the recommendations have been revised to include the following:
HAART for all HIV positive pregnant mothers eligible for treatment according to CD4 cell counts or clinical staging.
ARV prophylactic regimens for HIV positive pregnant mothers who do not require HAART by the above criteria.
Implementation of the recommendations set fourth an inevitable exposure of embryos/fetuses to the toxic effects of ARV drugs. Current information may not recommend use of some ARV drugs in pregnancy (e.g. Efavirenz) for fear of its teratogenic potential (Jeantils et al., 2006). Concurrently, some
14
controversy still lingers about the safety of some of the recommended ARV drugs hence the need to further clinical investigations of their safety in pregnancy.
1.4. Statement of the problem
Birth defects are a worldwide challenge. Several countries/sub-regions have established their reference biodata and national registry of the prevalence and types of birth defects. This has not been done in Uganda, yet there is apparently a steady increase of birth defects observed and reported in the media.
ART prophylaxis as a specific intervention for PMTCT coupled with advances in HAART have led to increased usage of ARV drugs in pregnancy. Despite the high success rates of PMTCT (below 1-2% in developed countries, Thorne and Newell, 2003), there is little information on the teratogenicity of the complex ARV regimens yet more women (child bearing age group) are being enrolled on HAART.
1.5.
Research Significance
This research will enrich the field of Embryology (Anatomy) with knowledge on the types of birth defects prevalent in the catchment area of MRRH and the teratogenicity of ARV drugs used in pregnancy.
Findings will provide a basis for establishment of reference biodata for the types and prevalence of birth defects among natives of the catchment area of MRRH.
15
Considering the increasing number of women accessing HAART and the pressure for PMTCT, it is essential to analyse the safety of the diverse ART drug combinations for the indigenous population among whom such studies have not been done.
1.6. General Objective
To list the types and analyse the prevalence of birth defects among babies born to mothers on ARV drugs and among babies born to mothers not on
ARV drugs in MRRH.
1.7. Specific Objectives
To: a) Compare the types of birth defects among babies born to mothers on ARV drugs and those born to mothers not on ARV drugs b) compare the prevalence of birth defects among babies born to mothers on ARV drugs and those born to mothers not on ARV drugs c) determine prevalence and types of birth defects among the babies in relation to the ARV drug regimen used by the mother during pregnancy. d) compare the prevalence of birth defects by sex among babies born in MRRH
1.8.
Hypothesis
Birth defects occur commonly but use of ARV drugs in pregnancy is a risk factor.
16
1.9.
Conceptual framework
Predisposing Factors Immediate Factors
Maternal age Smoking
Paternal age
Nutritional state of mother
Mother’s occupation
Alcohol consumption
Twinning
X-ray & other radiations
House hold income
Parity
Marital status
Tribe
Residence (Urban/rural)
Education level
Religion
-
-
-
ARV use
Maternal malnutrition
Other medicines
Chronic disease of the mother
17
CHAPTER TWO
LITERATURE REVIEW
2-3% of births are associated with major birth defects (Dastgiri et al ., 2002; and Abdi-Rad et al ., 2008). There is, however, a variable frequency in different populations, ranging from 1.07% in Japan (Imaizumi et al ., 1991) to 4.3% in Taiwan (Chen et al., 1992). It is also important to note that regional variations occur in the prevalence of specific birth defects as sighted in the literature below.
Abdi-Rad et al . (2008) determined the prevalence of overt birth defects at birth in Urmia, Northwestern Iran. Their four and a half year analysis of birth defects at Motahhari Hospital, documented 264 overt congenital anomalies among 14,121 births (1.87%). Anomalies of the central nervous system and musculoskeletal system were most frequent, accounting for
52.65% and 23.86% (respectively) of all anomalies. The digestive and urogenital systems, ear and neck were also affected with 7.20%, 6.82% and
4.17%, while chromosomal and other anomalies contributed 4.92% and
0.38% of defects respectively.
A similar study was conducted by Dastgiri et al . (2002) to determine the epidemiology of congenital anomalies in Glasgow, United Kingdom.
Among the 223,777 births, 7,250 had some form of congenital anomaly i.e.
324 per 10,000 births. Congenital heart disease ranked highest followed by limb, and digestive system anomalies with a tally of 50, 49 and 47 cases per
10,000 births respectively. Anomalies of the nervous, genitourinary, and musculoskeletal systems were quite common with 37, 30 and 25 cases per
18
10,000 births. Also highly significant were neural tube defects and chromosomal anomalies with 24 cases per 10,000 births each.
Rankin et al.
(2005) described trends in total and live birth prevalence of birth defects, and the regional differences in prevalence of the defects among five British regions. 839,521 births in five geographic regions of Britain comprised the sample. 10,844 birth defects were recorded, a prevalence of
129 per 10,000 births. Cleft lip and or palate, anencephaly and spina bifida were the most prevalent defects followed by gastroschisis and omphalocele.
In Uganda, Kiryowa et al . (2008) examined 754 new born babies in Mulago
Hospital, Kampala, for the prevalence, nature and characteristics of external congenital anomalies. 0.2 % of the babies were considered hermaphrodites.
35 external birth defects were diagnosed in 33 babies(4.4%). Limb defects accounted for 45.7% while cleft lip and palate made 14.2% of all defects.
Also common were central nervous system defects (8.5%), omphalocele and spina bifida, 5.8% each. Other anomalies, together, constituted 20.0%.
The use of HAART (any potent combination of three or more drugs) to combat HIV infection and the prophylactic use of ARV drugs (PMTCT) have reduced the rate of Mother to Child Transmission of HIV from 33% to
1-2% (Wongvipat, 2001; Thorne and Newell, 2003). The trend in prevalence and types of birth defects among such ARV drug users is yet to be ascertained. Several clinical studies have henceforth been conducted to assess the safety/risk of birth defects associated with some of these drugs.
19
Thorne and Newell (2003) decried the exposure of babies, born to HIV infected mothers, to ARV drugs for which there is limited information on toxicity. They cited a report (from France) of eight children with mitochondrial dysfunction, two of whom died, following exposure to AZT; and a report of a shorter duration of pregnancy in association with use of PIs in pregnancy. In 2005, Thorne and Newell wrote about the risk of cancers, mitochondrial disease, haematological abnormalities and prematurity of babies exposed to HAART.
In Bethesda, USA, rates and types of birth defects in relation to the timing of exposure to ARV drugs, among babies born to HIV infected women, were analysed by Watts et al ., (2007). They assessed 2527 live births among 2353 mothers. Ninety babies had birth defects. Genital anomalies, specifically hypospadius, were significantly high among babies born to mothers who used ARV drugs during the first trimester. Zidovudine use in the first trimester was associated with hypospadius.
Ibieta et al.
(2009) analysed the proportion and characteristics of congenital anomalies among 623 children, 479 of whom were exposed to ARV drugs in utero. Birth defects were seen in 52 children, the most frequent being genitourinary and cardiological. Children born to mothers who started ART in the first trimester had comparable rates of birth defects as those whose mothers started ART in the second trimester (7.4% and 8.8% respectively).
None of the ARV drugs was associated with an increase in birth defects.
In Buenos Aires (Argentina), Duran et al.
(2004) evaluated ART related toxicities among pregnant women. They assessed the prevalence of birth
20
defects among 271 pregnant mothers on ARV drugs for PMTCT. One hundred thirty eight (138) of them had been given AZT mono-therapy; 54 were on duo-therapy of 2NRTIs and the rest on triple therapy i.e. 41 were on
2NRTIs with a NNRTI while the 38 on 2NRTIs and a Protease Inhibitor.
Eight (2.3%) cases of congenital anomalies occurred, a prevalence similar to that expected in the general population.
The risk of birth defects associated with Nelfinavir exposure during pregnancy was investigated by Conner et al.
(2003). They analysed data of
757 live births exposed to Nelfinavir in utero. Eight birth defects (3.1%) were recorded among 256 mothers exposed to the drug in their first trimester. Whereas the rate was not significantly different from that of the
CDC, they recommended Nelfinavir use where the benefits outweigh the potential risk to the foetus.
Alimenti et al.
(2006) compared the neuro-development of 39 children exposed to HAART in utero with 24 children not exposed to HAART. The former group had lower development and adaptive behavior scores compared to the latter. However, after correcting for maternal substance use,
Alimenti et al.
(2006) ruled that the observed differences were not significant.
In the UK and Ireland, Townsend et al . (2006) analysed the relationship between ART in pregnancy and occurrence of birth defects. Defects were reported in 101 of 3172 infants. They did not find a statistically significant association between the prevalence of birth defects and exposure to ARV drugs. They also noted a similar prevalence of defects regardless of the time
21
of initial exposure to HAART, nor was there a significant association with the type of ART i.e. mono-therapy or dual therapy; HAART with a PI or
NNRTI.
Saitoh et al.
(2005), in the University of California, USA, reported a case of myelomeningocele in an infant whose mother used Efavirenz during the first
16 weeks of pregnancy. They related the anomaly to similar observations in primates suggesting that Efavirenz is a potential teratogen.
22
CHAPTER THREE
RESEARCH METHODOLOGY
3.1
Study subjects/ Area of study
Five hundred mothers naïve of ARV drugs and 500 mothers on ARV drugs during their current pregnancy will be included in the study. Because numbers of the latter may be difficult to realise, organizations providing
ART will be visited to identify such mothers for follow up till delivery. Such organizations include the ISS clinic, MJAP Mbarara and TASO Mbarara.
The catchment area of MRRH will provide the study subjects. These will be the babies of mothers who turn up to deliver on the maternity ward of
MRRH, and their mothers. The mothers will be the major respondents of the research interview. Mothers who access ART from the above organizations but deliver outside MRRH will be followed up for the interview and to examine their babies for birth defects.
Mothers who fail to carry their pregnancies to term will also be included in the study. They will be subjected to the same questionnaire (Appendix i), and where possible, the expelled foetuses/embryos (dead and alive) will be thoroughly examined for birth defects. The format in Appendix i will be followed in the examination and recording of the findings.
For purposes of obtaining an informed consent of the respondents, every mother, on individual basis, shall be furnished with detailed information concerning the research i.e. the research objectives, benefits and the
23
importance of examining them and their new born babies. It shall be clarified that:
The choice to participate in the research is completely voluntary
Every mother, even after giving consent to participate, shall retain the right to opt out of the research any time they feel like without repercussion against them
A physical examination shall be done to both the mother and her new born baby on the consent of the former
Such examination is liable to cause some inconvenience or discomfort to both the mother and baby or either of them
No surgical intervention, phlebotomy or invasive procedure whatsoever shall be performed unto either subject
No monetary or other forms of tangible benefits shall be realized in appreciation for participation in the research as a respondent
Every respondent shall be entitled to full information pertaining to the progress and findings of the research
All information obtained shall strictly be kept confidential and shall only be used for purposes of the said research
A respondent who consents to participate shall confirm such consent by appending her signature or thumb print on the availed Consent
Form (Appendix iii)
Mothers shall also be informed of the available collaboration with professionals who can handle the anomalies, if any. Where the defect can not be corrected in MRRH, relevant information shall still be given to the
24
concerned parents. Subsequently, mothers who will give written consent to the research will be recruited into the study.
Permission will also be sought from the administration of MRRH, MJAP,
ISS clinic and TASO Mbarara to allow me interview their clients/mothers and the newborn babies.
3.2 Research design/Data Collection
The research will be both a prospective and a cross sectional survey i.e. mothers on dual therapy for PMTCT and mothers on HAART during their pregnancy will, on their consent, be followed till birth and interviewed shortly after birth. Mothers who deliver in MRRH, regardless of their HIV status and ARV drug usage, will similarly be recruited. All respondents and their babies will be examined for any externally visible birth defects. The same physical examination will be done to foetuses/embryos expelled before term as well as the still births. The questionnaire in Appendix i will be followed to interview all consented mothers regardless of their pregnancy outcome. Their nutritional status will be assessed, among other maternal factors related to acquisition of birth defects among their babies. The head circumference and Crown-Heel Length of the babies will be measured too.
The following tools will be used to facilitate the interview and data collection:
Mothers’ medical records/files
Medical records/files of mothers on ARV drugs, both PMTCT and HAART, will be retrieved (where possible) for a review of their previous medical history. This will help find their ART regimen, duration of therapy and any
25
changes of regimen and dates/reasons for such changes. Ante-natal cards will also be useful as sources of information regarding the health of the mother during her pregnancy.
Research Questionnaire (Appendix i)
This will be written in English, but translated to the local languages (Nkole and Ganda) during the interview. It will be pilot tested and modified accordingly. The questionnaire will be administered according to the language spoken by each respondent. The main researcher and five research assistants will administer the questionnaires to the mothers. The research assistants will be trained to administer the questionnaires and record the responses and findings. The minimum academic qualifications of research assistants will be a Diploma in Nursing and or midwifery for easy appreciation, description and recording of deformities found.
Some sections of the questionnaire will be administered to the mothers to get information regarding their background characteristics and the outcome of their pregnancies, their HIV status and ART experience. There will be a section to assess the maternal clinical status and any birth defects they may have, as these may have a bearing on the state of the babies. Another section will be used to record particulars of the newborn (e.g. sex and birth weight), and to describe any defects found on physical examination of the newborn.
The last part of the questionnaire will explore the paternal background characteristics and health, as well as a history of birth defects among his immediate blood relations.
26
Clinical Examination
All newborn babies, prematures and stillbirths will be carefully examined for external birth defects. Their head circumferences and crown heel lengths will be measured and recorded in the questionnaires. Any defect(s) identified will be described and recorded. The appropriate diagnoses will be written below each description. For record and reference purposes, digital photographs of the defects will be taken. (Mothers will be counseled and advised accordingly on defects that warrant urgent medical/surgical attention. A referral system will be arranged to cater for babies whose defects need professional care elsewhere).
3.3
Data Analysis and Presentation
Subjects will be assigned numbers as information is collected. The data collected will be sorted, coded and analysed using Epi-Info. Findings will be presented on bar graphs, pie charts and frequency tables. Final research findings will be disseminated to the relevant stake holders.
27
REFERENCES
Abdi-Rad Isa, Khoshkalam, Hamid-Reza and Farrokh-Islamlou (2008). The prevalence at birth of overt congenital anomalies in Urmia, Northwestern
Iran. Arch. Iranian Med. 11(2): 148-151 .
Alimenti A., Forbes J. C., Oberlander T. F., Money D. M., Grunau R. E.,
Papsdorf M. P., Maan E., Cole L. J. and Burdge D. R. (2006). A prospective controlled study of neuro-development in HIV-uninfected children exposed to combination antiretroviral drugs in pregnancy. Pediatrics 118(4): e1139-
45 .
Anonymous (2006). Birth defects. Accessed on February 14 th 2008 from http://www.marchofdimes.com/pnhec/4439 1206.asp
Chen C. J., Wang C. J., Yu M. W. and Lee T. K. (1992). Perinatal mortality and prevalence of major congenital malformations of twins in Taipei city.
Acta Genet Med Gemellol (Roma) 41(2-3): 197-203 .
Conner S. D., Covington D. L., Doi P. A., Swinson J. and Daniels E. M.
(2003). Risk of birth defects associated with Nelfinavir exposure during pregnancy.
10 th Conference on Retroviruses and Opportunistic Infections;
Boston, USA. Abstract no. 782.
Dastgiri S., Stone D. H., Le-Ha C. and Gilmour W. H. (2002).
Prevalence and secular trend of congenital anomalies in Glasgow, UK.
Arch. Dis. Child.
86:257-263 doi:10.1136/adc.86.4.257
28
Duran A., Masciottra F., Toibaro J., Lourtau L., Ivalo S. and Losso M.
(2004). Toxicity related to ART in a cohort of HIV pregnant women of
Buenos Aires. 11 th Conference on Retroviruses and Opportunistic
Infections; San Francisco, California. Abstract no. 940.
Finkel Richard, Luigi X., Cubeddu and Clark Michelle A. (2009).
Lippincot’s Illustrated Reviews: Pharmacology. 4 th Ed. Lippincot Williams and Wilkins.
Furtado M. R., Callaway D. S. and Phair J. P. (1999). Persistence of HIV-
1 transcription in peripheral-blood mononuclear cells in patients receiving potent antiretroviral therapy. N. Engl. J. Med.
340: 1614-1622.
Gregg N. M. (1941). Congenital cataract following German measles in the mother. Trans. Opthal. Soc. Aust . 3:35 in Moore Keith L. & Persaud T. V.
N. (1998). The Developing Human: Clinically oriented Embryology. 6 th edition; W. B. Saunders; Philadelphia, Pennyslvania.
Ibieta Fernandez M., Amador Ramos J. T., Cano Bellon J. M., Gonzalez-
Tome M. I., Guillen Martin S., Navarro Gomez M., de Jose M. I., Beceiro J.,
Iglesias E., Prieto L., Santos M. J., Martinez Guardia N., Roa M. A. and
Regidor J. (2009). Birth defects in a cohort of uninfected children born to
HIV-infected women. An. Pediatr. (Barc). 70(3): 253-64.
29
Imaizumi Yoko., Yamamura Hirozo., Nishikawa Masako., Matsuoka
Matsuo and Moriyama Ikuko (1991). The prevalence at birth of congenital malformations at a maternity hospital in Osaka city, 1948-1990. Journal of
Human Genetics 36(3): 275-287
Jeantils V., Khuong M. A., Delassus J. L., Honore P., Taverne B., Uzan M. and Tassi S. (2006). Efavirenz (Sustiva) in pregnancy: a study about 12 HIV patients. Gynecol. Obstet. Fertil. 34(7-8): 593-6.
Kiryowa Haruna, Ibingira Charles and Ochieng Joseph (2008). Prevalence, nature and types of congenital anomalies at Mulago hospital. 4 th Annual
Makerere University College of Health Sciences Scientific Conference, 17-
19 September 2008 . Hotel Africana Ltd., Kampala, Uganda.
Lenz W. (1988). A short history of thalidomide embryology. Teratology 38:
203 in Moore Keith L. & Persaud T. V. N. (1998). The Developing Human:
Clinically oriented Embryology. 6 th edition; W. B. Saunders; Philadelphia,
Pennyslvania.
McBride W. G. (1961). Thalidomide and congenital abnormalities. Lancet 2:
1358.
Moore Keith L. & Persaud T. V. N. (1998). The Developing Human:
Clinically oriented Embryology. 6 th edition; W. B. Saunders; Philadelphia,
Pennyslvania.
30
Rang H. P., Dale M. M., Ritter J. M. and Flower R. J. (2007). Rang and
Dale’s Pharmacology. 6 th Ed. Churchill Livingstone.
Rankin J., Pattenden S., Abramsky L., Boyd P., Jordan H., Stone D.,
Vrijheid M., Wellesley D. and Dolk H. (2005). Prevalence of congenital anomalies in five British regions, 1991–99.
Arch Dis Child Fetal Neonatal
90:F374-F379 doi:10.1136/adc.2003.047902
Sadler T. W. (1995). Langman’s Medical Embryology, 7 th edition; Williams and Wilkins; Baltimore, U.S.A.
Sadler T. W. (2004). Langman’s Medical Embryology. 9 th edition; Lipincott
Williams and Wilkins; Baltimore, U.S.A.
Sadler T. W. (2005). Langman’s Essential Medical Embryology. Lipincott
Williams and Wilkins; Baltimore, U.S.A.
Saitoh A., Hull A. D., Franklin P. and Spector S. A. (2005).
Myelomeningocele in an infant with intrauterine exposure to Efavirenz. J.
Perinatol. 25(8): 555-6 .
Thorne C. and Newell M. L. (2003). Antenatal and neonatal antiretroviral therapy in HIV infected women and their infants: a review of safety issues.
Med Wieku Rozwoj 7(4Pt 1): 425-36 .
Thorne C. and Newell M. L. (2005). The safety of antiretroviral drugs in pregnancy. Expert Opin. Drug Saf. 4(2): 323-35.
31
Townsend C. L., Tookey P. A., Cortina-Borja M. and Peckham C. S. (2006).
Antiretroviral therapy and congenital abnormalities in infants born to HIV infected women in the United Kingdom and Ireland, 1990 to 2003. J.
Acquir. Immune Defic. Syndr. 42(1): 91-4.
Walker Roger and Clive Edwards (2003). Clinical Pharmacy and
Therapeutics. 3 rd Ed. Churchill Livingstone.
Watts D. H., Li D., Handelsman E., Tilson H., Paul M., Foca M., Vajaranant
M., Diaz C., Tuomala R. and Thompson M. (2007). Assessment of birth defects according to maternal therapy among infants in the women and infants transmission study. J.
Acquir. Immune Defic. Syndr. 44(3): 299-305 .
WHO (2007). Prevention of Mother-To-Child-Transmission (PMTCT). A briefing note. Department of HIV, WHO. Retrieved on 8 th February 2010 from http://www.google.com/search?hl=en&client=firefoxa&channel=s&rls=org.mozilla%3Aen-
US%3Aofficial&hs=t3m&q=History+of+PMTCT&aq=f&aqi=&oq =
Wilson J. G. and Fraser F. C. (1977). Handbook of Teratology Vol. 1-3.
Plenum press; New York, U.S.A.
Wongvipat Nancy (2001). HAART works! Retrieved on 19 th February 2010 from http://www.thebody.com/content/treat/art4826.html
32
Appendix i: RESEARCH QUESTIONAIRRE
A: MATERNAL BACKGROUND CHARACTERISTICS
1.
Respondent’s no. ……………………………………….……………
2.
Age………...........................................................................................
3.
Marital status Married Never married
Divorced Widow
4.
Religion Anglican Catholic Moslem
SDA Other
5.
Tribe Nkole Kiga Ganda Other
6.
Residence Urban Rural
7.
Education level None P.1 – P.4 P.5 – P.7
S.1 – S. 4 S.5 – S.6 Tertiary institution
8. Number of years of spent in school ………………………………….
9.
Occupation Gainfully employed Non-gainfully employed
10.
What is your average monthly income? Ug Shs…..…………………
33
B. OBSTETRIC HISTORY
1. Parity .………………………………………………………………
2. What was the outcome of your latest pregnancy?
Abortion Miscarriage
Still birth Live baby
Twins/multiple delivery
3. Sex of baby Male Female Ambiguous
4. What was the birth weight? …………………….……………….. Kg
5. If twins/multiple delivery, what were the sexes?
…………………………………………………………………………..
6. What were their birth weights? …………………………………..Kg
7. Have you ever heard about the term “Birth defects?” * Yes No
8. Have you ever had a child/children with a birth defect(s)?
Yes No
9. If yes, please describe the type of defect(s)
………………………………………………………………………………
………………………………………………………………………………
………………………………………………………………………………
10. Have you ever given birth to twins? Yes No
11. If yes, how many sets of twins have you had? ……..…………………
12. Did you have an X-ray investigation (or any intervention which involved
use of radiations) during your recent pregnancy? Yes No
13. If yes, when was that?
1 st three months of pregnancy
4 th to 6 th months of pregnancy
7 th to 9 th months of pregnancy
*
Examples are cleft lip, amelia, albinism, conjoined twins, anal atresia, heart defects (holes), tongue tie.
34
C: MATERNAL HEALTH AND DRUG USE DURING THE RECENT
PREGNANCY
1. Did you use any oral herbal medicines during the pregnancy?
Yes No
2. If yes, please state the names of the herbs you used
………………………………………………………………………………..
3. When did you use the medicines?
1 st three months of pregnancy
4 th to 6 th months of pregnancy
7 th to 9 th months of pregnancy
Throughout the pregnancy period
4.What was the frequency of use of the medicines?
Daily for a week
Daily for 2-4 weeks
Daily for over a month
Other (specify) …………………………………………….
5. Did you ever smoke during the pregnancy? Yes No
6. If yes, when did you do so?
1 st three months of pregnancy
4 th to 6 th months of pregnancy
7 th to 9 th months of pregnancy
Throughout the pregnancy period
7. What was the frequency of tobacco/cigarette use?
Daily for a week
Daily for 2-4 weeks
Daily for over a month
Other (specify) …………………………………………….
35
8. How many sticks of cigarettes/pipes of tobacco (average) did you consume a day?………………………………………………………….
9. Did you consume any alcoholic drinks during the pregnancy?
Yes No
10. If yes, when did you consume the drinks?
1 st three months of pregnancy
4 th to 6 th months of pregnancy
7 th to 9 th months of pregnancy
Throughout the pregnancy period
11. How often did you drink the alcoholic beverages?
Daily for a week
Daily for 2-4 weeks
Daily for over a month
Other (specify) ……………………………..………………….
12. How much alcohol (on average) did you consume a day?
……………………………………………………………………………….
13. What chronic diseases did you suffer during the pregnancy?
...........................................................................................................................
...........................................................................................................................
14. When were you affected by the diseases?
1 st three months of pregnancy
4 th to 6 th months of pregnancy
7 th to 9 th months of pregnancy
Throughout the pregnancy period
36
15. Please name the drugs which were used to manage the diseases in 13 above.
………………………………………………………………………………
………………………………………………………………………………
16. What were the doses and durations of the drugs listed above?
………………………………………………………………………………
………………………………………………………………………………
………………………………………………………………………………
………………………………………………………………………………
………………………………………………………………………………
17. Tick the conditions you had during your latest pregnancy
A painless sore (chancre) in private parts
A widespread non itchy body rash
Sores in the mouth, nose, throat or private parts
18. Where you treated? Yes No
19. When were you treated?
1 st three months of pregnancy
4 th to 6 th months of pregnancy
7 th to 9 th months of pregnancy
20. State the name, dose and duration of the drug or drugs you used
………………………………………………………………………………
………………………………………………………………………………
………………………………………………………………………………
Now I am going to ask you questions related to HIV and ARV drugs
37
D: MATERNAL HIV STATUS AND ARV DRUG EXPERIENCE
1. Have you ever had an HIV test? Yes No
2. If yes, what was the result? Negative Positive
Don’t know (Never received test results)
3. If positive, are you on ARV drug treatment? Yes No
Only mothers on ARV drugs should respond to the following questions.
4. When did you begin using ARV drugs?
Before conception
1 st three months of pregnancy
4 th to 6 th months of pregnancy
7 th to 9 th months of pregnancy
5. What was your initial ARV drug combination? …………… Don’t know
6. How long did you use the regimen in 5 above?
………..……..years ……………...months …………..weeks
7. What is your current ARV drug combination?…………………………..
8. When was the combination changed?
..……..years …..….….months ………..weeks ago Not applicable
9. Why was your combination changed?
Drug toxicity
Treatment failure
Pregnancy
TB/HIV co-management
Other (specify)……………………………………………….
10. What problems have you encountered due to use of the ARV drugs?
...........................................................................................................................
..........................................................................................................................
38
11. How have you responded to/managed the problems?
……………………………………………………….………………………
……………………………………………………………………………..…
………………………………………………………..………………………
12. Have you ever missed doses of your ARV drugs? Yes No
13. If yes, why?
…………………………………………………………….…………………
……………………………………………………………………………….
14. How many times did you miss in the last three months? ..………………
15. If no, how do you ensure that you do not miss any of the doses?
……………..………………………………………………………………..
………………………………………………………………………………
39
E: MATERNAL CLINICAL EVALUATION
(For all mothers, regardless of their HIV and ARV drug status)
1. Pallor Yes No
2. Jaundice Yes No
3. Height ………………………..… Cm
4. Weight ………………………….. Kg
5. BMI i.e. Weight (Kg) ÷ [Height (M) X Height (M)] …………… Kg/M 2
6. Has the mother got any external birth defect? Yes No
7. If yes, describe it….…………………………………………………..…
………………………………………………………………………………
………………………………………………………………………………
…………………………………………………………………… ………..
(Diagnosis…………………………………………………………………………)
40
F: CLINICAL EVALUATION OF THE:
Full term newborn Premature
Fresh Still Birth Macerated Still Birth
Arbotus
(For multiple births, use a separate form for each baby)
1. Sex Male Female Ambiguous
2. Birth weight …………………………………………………… Kg
3. Head circumference ……..…………………………………….. Cm
4. Crown Heel Length (CHL) …………………………………….Cm
(Only findings considered abnormal should be recorded under subsections 5-14)
5. Head, Face and Ears
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
( Diagnosis………………………………………………………………….……)
6. Oral Cavity, Tongue and Palate
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
( Diagnosis………………………………………………………………….……)
41
7. Neck
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
(
Diagnosis………………………………………………………………….……)
8. Thorax
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
( Diagnosis………………………………………………………………….……)
9. Abdomen
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
(
Diagnosis………………………………………………………………….……)
10. The Back
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
( Diagnosis………………………………………………………………….……)
42
11. Limbs and hands/feet
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
( Diagnosis………………………………………………………………….……)
12. External Genitalia and Perineum
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
(
Diagnosis………………………………………………………………….……)
13. Skin and hair
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
(
Diagnosis………………………………………………………………….……)
14. Any other findings considered abnormal
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
……………………………………………………………………………
( Diagnosis………………………………………………………………….……)
43
G: PARTENAL BACKGROUND CHARACTERISTICS & HEALTH
1. Status of husband/spouse Alive Dead Unknown
2. If living, how old is your husband/spouse? ………………...…… years
3. Occupation Gainfully employed Non-gainfully employed
4. What is his average monthly income? Ug Shs. ………………………..
5. Religion Anglican Catholic Moslem SDA Other
6. Tribe Nkole Kiga Ganda Other
7. Education level None P.1 – P.4 P.5 – P.7
S.1 – S. 4 S.5 – S.6 Tertiary institution Don’t know
8. Do you live together? Yes No Partly
9. Did he smoke during your latest pregnancy? Yes Not a smoker
10. If yes, how many cigars/pipes of tobacco did he consume a day?
…………………………………………………………………………….
11. Does he suffer any chronic disease/diseases? Yes No
12. If yes, please state the disease/diseases
………………………………………………………………………………
………………………………………………………………………………
13. Has he got any visible birth defect? Yes No
14. If he has, please describe it.
……………………………………………………………………………
……………………………………………………………………………
(Diagnosis …………………………………………………….…………………)
15. Has he got any immediate blood relative with birth a visible defect?
Yes No Don’t know
16. If yes, describe the defect
………………………………………………………………………………
(Diagnosis………………………………………………………..…………………..)
44
Appendix ii: RESEARCH BUDGET IN SWEDISH KRONA
I tem/activity SEK
1.
Equipment i.e.
A Laptop ……………………...…………………..……….… 12,500
A Desk top computer with accessories ..………………….….. 5,300
-
A Colour printer with Photocopier .…………………………. 4,200
10 Flash diskettes of 2GB each .……………………………... 1,250
A Digital camera ..………...……………………………….… 3,600
-
A Weighing Scale ……………………………………………. 200
-
A Height Scale ………………………………………………. 200
5 Tape measures ……………………………………………… 10
Sub Total …………….……………………………………… 27,260
2.
Consumables i.e.
- Internet (Modem, Installation and monthly subscription) ….. 9,000
Stationery and Secretarial services (Photocopying paper, Notebooks,
Box files, Folder files, Pens, Binding) ……………………….. 1,000
Printer cartridges ……………………………………………... 3,000
Sub Total …………………...………………………………. 13,000
3.
Travel (Within and abroad) ……….…………………………. 15,000
4.
Expenses in Sweden ……………….……………………….. 20,000
5.
Allowances for 5 Research Assistants ………………………. 60,000
6.
Subsistence ……………………..…………………………….. 22,000
7.
University fees for three academic years ...……………….. 45,860.22
8.
Research dissemination …………………………..……………. 2,860
GRAND TOTAL 205,980.22
45
Appendix iii: PROPOSED TIME FRAME
ACTIVITY PERIOD
1.
Seeking permission from the Executive Director MRRH,
and Directors of MJAP, ISS Clinic and TASO Mbarara to
conduct research in their settings ………………..…….... March 2010
2. Recruiting Research Assistants …………………………. March 2010
3. Pilot testing and adjusting the questionnaire ……. March – April 2010
4. Data collection ……………………………. May 2010 – October 2011
5. Data compilation and analysis ……… November 2011 – January 2012
6. Discussion and write up ………………… February 2012 – April 2012
7. Submission to External Examiner ………………………… April 2012
8. Review/attention to External Examiner’s comments ... September 2012
9. Thesis submission to the Academic Registrar………. …. October 2012
46