Chemicals and reagents
advertisement

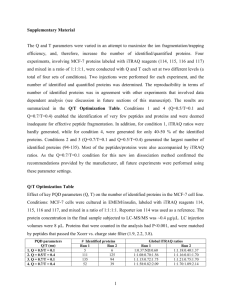
1 miR-27b-Regulated TCTP as a Novel Plasma Biomarker for Oral Cancer: From Quantitative 2 Proteomics to Post-Transcriptional Study 3 4 Wan-Yu Lo1,2,3, Huang-Joe Wang4,5, Chih-Wei Chiu6, Sung-Fang Chen6* 5 1 6 2. . 7 3. Department of life science, National Chung Hsing University, Taichung, Taiwan 8 4. Department of Internal Medicine, School of Medicine, China Medical University, Taichung, Taiwan 9 5. Division of Cardiology, Department of Medicine, China Medical University Hospital, Taichung, Taiwan 10 6. Department of Chemistry, National Taiwan Normal University, Taipei, Taiwan Graduate Institute of Integrated Medicine, China Medical University, Taichung, Taiwan Division of Surgery, Department of Medical Research, China Medical University Hospital, Taichung, Taiwan 11 12 13 *Correspondence: Dr. Sung-Fang Chen, Depa rt m ent of C hem i st r y, National Taiwan Normal 14 University, No. 88, Sec. 4, Ting-Chow Rd, Taipei, Taiwan, 11677 Taipei, Taiwan 15 Phone: 886-2-77346210 Fax: 886-2-9324249 16 Email: sfchen@ntnu.edu.tw 17 18 19 Keywords: Quantitative proteomic analysis, iTRAQ, oral cancer, translationally controlled tumor 20 protein, TCTP, miR-27b 21 1 22 Abstract 23 We combined an iTRAQ-based quantitative proteomic analysis and the miRNA determination to 24 profile potentially novel biomarker from oral cancer. There are 757 and 674 unique proteins were 25 identified from proteomic analysis, and 13 proteins displayed consistent underexpression (<0.67 fold) 26 in normal tissues in comparison with the corresponding tumor tissues. After the preliminary screening, 27 the EGFR, OAT, TPT1, ITGA6, G3BP1 and CB39L were the six genes validated in the 37 oral cancer 28 patients (T1, n=10; T2, n=10; T3, n=10 and T4, n=7). The TPT1, ITGA6 and CAB39L genes were 29 displayed the higher transcriptions level in the tumor tissues and the TPT1, ITGA6 and CAB39L 30 proteins were also shown overexpression in the tumor tissues from the same patients. The miR-19a, 31 19b, 27a, 27b, 186, 203 and 377 transcripts were predicted and the miRNA-27a and 27b level was 32 shown significantly reduction in the tumor tissues and the plasma of OSCC patients. In the in vitro 33 study, the overexpression of miR-27b significantly only decreased TCTP protein and gene levels in 34 both of HSC-3 and Cal-27 cell lines. Our results demonstrate that human miR-27b regulates the 35 expression of the TCTP tumor protein, and circulating miR-27b may be useful as a biomarker for oral 36 cancer research. 37 2 38 Introduction 39 An estimated 263,900 new cases and 128,000 deaths from oral cavity cancer (including lip 40 cancer) occur annually worldwide [1]. Smoking, betel-quid and areca-nut chewing, alcohol use, 41 smokeless tobacco products and Human Papillomavirus (HPV) infection are the major risk factors for 42 oral cancer. Various treatment options including surgery, radiotherapy and chemotherapy are available 43 for oral cancer. However, the five-year survival rate of oral cancer is one of the lowest among common 44 malignant neoplasms [2]. In Taiwan, an endemic betel quid chewing area, a significantly increasing 45 trend in oral cancer has been observed in males [3]. In 2006, oral cancer became the 6th most common 46 cancer in Taiwan and the 4th most common cause of cancer deaths in Taiwanese men. Therefore, the 47 development of a reliable, accurate, cost-effective and noninvasive test for oral cancer is highly 48 desirable [4,5]. The alteration of genes has been traditionally revealed by the use of cytogenetics, 49 immunohistochemistry, or molecular approaches based on one or a few genes that change the 50 expression of many genes, e.g., oncogenes and tumor suppressor genes, which have been associated 51 with oral carcinogenesis [6-8]. Genomics has been incorporated in oncology research, and now, in the 52 post-genomic era, there is a strong drive to additionally incorporate proteomic technologies[9,10]. 53 Proteomics can help us to better understand the changes in the levels of multiple proteins 54 involved in oncogenesis and cancer progression and identify new diagnostic and prognostic biomarkers 55 [11]. Quantitative proteomics is an important branch of proteomics that is applied to quantify and 56 identify all the proteins expressed by a whole genome or in a complex mixture. The method of using 57 isobaric tags for relative and absolute quantification (iTRAQ) was developed in 2004. This method 58 uses global peptide labeling to preserve post-translational modification information and involves the 59 simultaneous quantitative proteomic analysis of four samples under the same experimental conditions 60 [12, 13]. This unique approach labels samples with four independent isobaric tags of the same mass that, 3 61 after fragmentation in MS/MS, give rise to four unique reporter ions (with m/z values ranging from 114 62 to 117) that provide quantitative information upon integration of the peak areas to quantify the four 63 different samples [14, 15]. The advanced combination of proteomics and bioinformatics provides the 64 opportunity to study changes in the global proteome and other molecular-level indicators of expression 65 in cells at any time point or treatment. Unfortunately, only a few limited studies have been conducted 66 in oral cancer research to date, and none have reported a miRNA-related approach. 67 The miRNAs are regulatory, non-coding RNAs approximately 21–23 nucleotides long that are 68 expressed at specific stages of tissue development or cell differentiation and have large-scale effects on 69 the expression of a variety of genes at the post-transcriptional level. Through base pairing with target 70 mRNAs, miRNA induces RNA degradation or translational suppression of the targeted transcripts [16, 71 17]. Mature miRNAs result from the processing of pri-miRNAs in two sequential cleavage steps 72 mediated by two RNase III enzymes, Drosha and Dicer [18]. Each mature 21- to 23-nt miRNA product 73 contains a 2-nt 3′ overhang on each strand and acts as the functional intermediate of RNAi that direct 74 mRNA cleavage and translational attenuation. Although their biological functions remain largely 75 unknown, recent studies suggest that miRNAs contribute to the development of various cancers [19-23]. 76 An important aspect of cancer biomarker identification is the development of simple, noninvasive tests 77 that indicate cancer risk, allow for early detection, and enable the classification of tumors to ensure that 78 patients receive the most appropriate therapy while monitoring disease progression, regression, and 79 recurrence [24]. Serological biomarkers can be analyzed relatively easily and economically and 80 therefore have the potential to greatly enhance screening acceptance [25]. Determinations of serum 81 miRNA are more convenient and less costly than serum protein marker determinations. Thus, serum 82 miRNA biomarkers are more suitable for future clinical applications in parallel with cancer-related 83 examination and have the potential to be the reliable biomarkers that can be utilized to develop an 4 84 effective approach for the early diagnosis of oral cancer. 85 Our previous study exploited a high-throughput technique that yields results complementary to 86 the traditional gel-based proteomics approaches for oral cancer and colon cancer [26, 27]. In this study, 87 we globally surveyed differential protein expression to identify potential diagnostic marker proteins 88 from the paired tissues of patients with early stage oral cancer using a comprehensive iTRAQ analysis 89 and then utilized bioinformatics to predict the associated target miRNAs and validated the correlations 90 from the tissues and sera from patients at varying stages of disease. We determined that plasma 91 miR-27b levels can provide such a biomarker for early cancer detection in clinical applications and 92 provide new insight in cancer research. 93 5 94 Materials and methods 95 Patients and clinical samples for iTRAQ 96 We collected pairs of surgically archived specimens of primary oral squamous cell carcinoma 97 (OSCC) and their matched adjacent normal surrounding mucosa specimens from 20 patients at the 98 China Medical University Hospital (Taichung, Taiwan), the collection methods as described in our 99 previous study.26 The 20 patients were classified into two categories: T1 (n=10) and T2 (n=10) 100 according to UICC TNM staging. The cancer stage was defined by the extent of the lesion as 101 determined by physical examination, radiological studies and pathological examination. The histology 102 for each patient was confirmed by two independent histopathologists following fixation, embedding, 103 sectioning and H&E staining. Overall, the tumor specimens all contained 90% tumor cells. No tumor 104 cells were detected in the surrounding mucosal tissue. Tissues were kept at −80 °C continuously until 105 analysis. The collection protocols were approved by the Institutional Review Board of China Medical 106 University Hospital (DMR98-IRB-77) and informed consent was obtained from each subject. 107 Sample preparations for iTRAQ 108 The extraction of total protein from oral cancer tissues (Tumor, n=20) and the corresponding 109 normal tissues (Normal, n=20) were performed as previously described. Additionally, the protein 110 supernatants were enriched using a 3-kDa centrifugal filter as described by the manufacturer (Millipore, 111 Merck KGaA, Germany). This process was repeated twice using ddH2O for desalting and to remove 112 the protease inhibitor cocktail. The protein concentrations of the resulting supernatants were measured 113 using the Bio-Rad Protein Assay (Bio-Rad, Hercules, CA) according to the manufacturer’s instructions 114 and stored at -20 °C for subsequent processing. A total of 2000 µg of protein was collected from the 115 paired tumor and normal tissues in the 20 patients (100 µg protein from the normal and tumor tissue in 116 each patient; Normal group, n=20; Tumor group, n=20) for iTRAQ analysis. 6 117 Chemicals and reagents for iTRAQ 118 The acetonitrile solvent was chromatography grade from Merck KGaA. Bradford protein assay 119 kits were purchased from Bio-Rad. Modified porcine trypsin (sequencing grade) was obtained from 120 Promega (Madison, WI). The iTRAQ 4-plex reagent kits were purchased from Applied Biosystems 121 (Framingham, MA). Desalting spin columns were purchased from Pierce (Thermo Scientific, San Jose, 122 CA). Centrifugal filters were purchased from Millipore (Merck KGaA). Column packing materials for 123 analyte column were purchased from Macherey Nagel (Düren, Germany). Packing materials for the 124 trap column were purchased from Michrom Bioresources (Auburn, CA). All other chemicals and 125 reagents were analytical grade from Sigma-Aldrich (St. Louis, MO) unless otherwise stated. 126 Reduction, alkylation, digestion, and labeling with iTRAQ 127 For our iTRAQ experiment, the two groups of proteins isolated from the 20 patients were polled. 128 Protein samples were then reduced, alkylated, digested, and labeled with iTRAQ reagents according to 129 the recommended protocol (Applied Biosystems, Framingham, MA). The protein pellets were 130 resuspended in 0.5 M triethylammonium bicarbonate (TEAB), pH 8.5, and 2% sodium dodecyl sulfate 131 (SDS), reduced with 5 mM Tris (2-carboxyethyl) phosphine (TCEP) for 1 h at 60 °C, and alkylated 132 with 10 mM s-methyl methanethiosulfonate (MMTS) at room temperature for 10 min. A total of 60 µg 133 of protein was digested overnight in tryptic solution (30/1, w/w) at 37 °C. Digested samples were 134 labeled with the iTRAQ reagents, and ethanol and the corresponding iTRAQ reagent was added to each 135 sample vial. The samples were labeled as follows: 114, Tumor-1; 115, Normal-1; 116, Tumor-2; and 136 117, Normal-2. Duplicate sets of iTRAQ samples were labeled to monitor the consistency of the results. 137 After 1 h of iTRAQ labeling; the samples were then mixed and dried by centrifugal evaporation. 138 Strong cation exchange chromatography (SCX) and solution IEF 139 The dried, labeled peptide mixture was reconstituted with buffer A (10 mM KH2PO4 in 25% 7 140 ACN, pH 3). Peptide separation was performed using a Polysulfoethyl A Column (200 mm L× 2.1 mm 141 i.d., 5 µm, 300 Å, PolyLC, Columbia, MD) on an Agilent 1100 binary HPLC (Agilent Technologies, 142 Wilmington, DE) using a 90 min gradient. One-hundred twenty micrograms of iTRAQ-labeled 143 peptides were eluted at a flow rate of 200 µL/min with a gradient of 2% buffer B (10 mM KH 2PO4 in 144 25% ACN/ 350 mM KCl, pH 3) for 15 min, 2-40% buffer B for 38 min and 40-98% buffer B for 7 min 145 and then maintained in 98% buffer B for 5 min before equilibrating with 2% buffer B for 20 min. A 146 total of 24 fractions were collected, pooled and purified using C-18 Spin columns (Thermo Scientific, 147 San Jose, CA) for further nano-LC-MS/MS analysis. 148 One-hundred twenty micrograms of dried, iTRAQ-labeled peptide was dissolved in 0.72 mL 149 ddH2O and 2.88 mL IPG stock buffer (pH 3-10). The IPG strips (pH 3-10, 24 cm) were assembled on 150 the OGE trays and rehydrated for 30 min with a solution of 240 µL H2O and 0.96 mL IPG stock buffer. 151 The samples were loaded into 24 off-gel wells. Peptide separation was performed over 48 h using the 152 3100 OFFGEL fractionator (Agilent Technologies, Wilmington, DE) with a limiting current of 50 µA 153 and a limit of 50 kV·h before holding the voltage at 500 V. The samples from the collected fractions 154 were purified using C-18 Spin columns (Thermo Scientific, San Jose, CA) for further nano-LC-MS/MS 155 analysis. 156 LC-ESI-MS/MS analysis 157 Each separated peptide fraction was reconstituted in buffer A (0.1% formic acid in 1% ACN), 158 and 0.5 µg of the peptides from each fraction were loaded onto a lab-made 2 cm trap column (100 μm 159 i.d., 5μm, 200 Å) at a flow rate of 10 µL/min in 2% buffer A. Separation was performed on a lab-made 160 10 cm analytical column (75 µm i.d., 3 µm, 100Å). Peptides were eluted at a flow rate of 250 nL/min 161 across the analytical column with a linear gradient of 2-40% buffer B (0.1% formic acid in 99% ACN) 162 for 95 min and 40-80% buffer B for 5 min and then maintained in 80% buffer B for 5 min before 8 163 equilibrating with 2% buffer B for 25 min. The LTQ-XL settings were as follows: spray voltage, 2.0 kV; 164 capillary temperature, 200 °C; and full MS scan range, 350-2000 Da. Thermo Scientific LTQ-XL was 165 operated in a data-dependent mode, i.e., using one MS1 scan for precursor ions followed by three 166 data-dependent zoom scans for precursor ions above a threshold ion count of 200,000 followed by three 167 data-dependent PQD-MS2 scans and CID-MS2 scans for precursor ions in zoom scan above a threshold 168 ion count of 100, with collisional energies of 29% for PQD and 35% for CID. 169 Database search and iTRAQ quantification 170 Protein identification and quantification in the iTRAQ samples were performed using Protein 171 Discoverer software (ThermoFisher, version 1.1) using MASCOT search algorithm. The search was 172 performed against the SwissProt v.2011_02 database (525207 sequences) with the following search 173 parameters: taxonomy, Homo sapiens; enzyme, trypsin; max. miss cleavages, 1; fixed modifications, 174 methylthiolation, N-terminal iTRAQ 4plex, lysine iTRAQ 4plex; variable modifications, methionine 175 oxidation, tyrosine iTRAQ 4plex; MS peptide tolerance, 1.5 Da; and MS/MS tolerance, 0.6 Da. 176 Proteins identified with at least two distinct peptides matched with a probability of 0.95 or above are 177 considered as correct identifications. 178 Patients and clinical samples for quantitative analysis of gene, tissue miRNA, plasma miRNA and 179 protein expression 180 The 17 patients were classified into two categories: T3 (n=10) and T4 (n=7) according to UICC 181 TNM stages, and samples were collected to evaluate the levels of gene, miRNA and protein expression 182 in the 20 patients following the same IRB project. Total RNA, miRNA and protein extractions were 183 isolated from pairs of surgically archived specimens and their matching adjacent normal surrounding 184 mucosa specimens in the total 37 patients. Following our previous study, the tumor and corresponding 185 normal tissues were dissected by laser pressure catapulting [27]. 9 186 Plasma was collected from the above 37 patients and 20 healthy volunteers from the same 187 department during 2007–2008. Cell-free nucleic acids were isolated from the blood samples using a 188 3-spin protocol (1500 r.p.m. for 30 min, 3000 r.p.m. for 5 min, and 4500 r.p.m. for 5 min) to 189 prevent contamination by cellular nucleic acids. All samples were then stored at −80 °C until further 190 processing. 191 Quantitative analysis of candidate gene expression 192 Total RNA was extracted from cells using the RNeasy Mini kit (QIAGEN), and the RNA was 193 reverse-transcribed with the SuperScript III First Strand Synthesis System (Invitrogen) according to the 194 manufacturer's instructions. Real-time quantitative PCR was run on a LightCycler 480 with 195 LightCycler 480 SYBR Green I Master kit (Roche). The primers used for real-time quantitative PCR 196 are listed in Supplemental data 1. A reaction mixture containing the following components at the 197 indicated final concentrations was prepared according to the manufacturer's instructions: 0.2 μL of 198 forward primer (20 μmol), 0.2 μL of reverse primer (20 μmol), 0.1 μL of UPL probe and 5 μL master 199 mix. Fifty nanograms of reverse-transcribed total RNA in a volume of 4.4 μL was added as the PCR 200 template. The GAPDH gene was selected for data normalization. A negative control without a cDNA 201 template was included to assess overall amplification specificity. The PCR cycle conditions were as 202 follows: an initial denaturation for 10 min at 95 °C was followed by 40 cycles of amplification at 95 °C 203 for denaturation, 60 °C for annealing and 72 °C for extension. After amplification, the temperature was 204 slowly elevated above the melting temperature of the PCR product to measure the fluorescence and 205 thereby determine the melting curve. The real-time PCR data were calculated by the 2−ΔΔCt method for 206 RNA quantification. 207 Immunoblotting 10 208 For the immunoblot assays, 40 µg of each protein extract from the in vivo (Tumor and normal 209 tissues) and in vitro (transfected and control groups) studies were individually separated by 12% 210 SDS-PAGE and treated as described in our pervious study. After blocking, the membranes were probed 211 with one of the following monoclonal antibodies: anti-CAB39L (Santa Cruz Biotechnology Inc., Santa 212 Cruz, CA), anti-TCTP or anti-ITGA6 (Cell Signaling Technology). 213 Quantization of miRNA expression 214 Total miRNA was isolated from tissues and plasma using the miRNeasy Mini Kit (Qiagen) 215 according to the manufacturer's instructions. All aliquots of crude products were treated using the same 216 procedure except for the use of 5U DNase. RNA was purified using the RNeasy MinElute Cleanup Kit 217 (Qiagen) according to the manufacturer's instructions. The microRNA levels were determined by 218 real-time quantitative PCR using the TaqMan MicroRNA Assays kit (Applied Biosystems, Foster City, 219 CA) according to the manufacturer's instructions for the analysis of the human miR-19a (ID 000395), 220 miR-19b (ID 000396), miR-27a (ID 000408), miR-27b (ID 000409), miR-186 (ID 000486), 221 miR-203(ID 000507) and miR-377 (ID 000566). The relative expression levels of the mature miRNAs 222 were calculated using the comparative CT (2−ΔΔCT) method with miRNA-U6 as an endogenous control 223 for data normalization. All experiments were performed in triplicate wells on an Applied Biosystems 224 7900 real-time PCR system. The significance of the differences between the plasma miR-27b levels of 225 the control subjects and patients was determined using Student’s t-test. 226 Transfection of miR-27b 227 The human oral cancer cell lines HSC-3 and Cal-27 were gifts from Dr. Jing-Gung Chung 228 (China Medical University) and grown in DME/F-12 medium (Gibco) supplemented with 10% FBS 229 and 1% glutamine under humidified 5% CO2 at 37℃. HSC-3 and Cal-27 Cells were plated in six-well 230 plates at a density of 1×105 cells/well. The next day, the cells were transfected with 100 nM of 11 231 synthetic miR-27b (Ambion) using Oligofectamine (Invitrogen) following the manufacturer's 232 instructions, a cohort transfected with miRNA-let7 as a negative control. The treatment was performed 233 in triplicate, and cells treated with the transfection reagent only were used as a mock control. 234 Statistical analysis 235 All experiments were repeated at least in triplicate. All results are expressed as the means ± SD. 236 Student’s t-test was used to evaluate differences between two groups. The data were analyzed using the 237 SPSS 12.0 software package. P-values <0.05 were considered to be significant. 238 12 239 Results 240 iTRAQ analysis of the paired tumor and normal tissues from oral cancer patients 241 A schematic flowchart of the iTRAQ method is provided in Figure 1. Protein identifications 242 were initially accepted when based on at least two peptide identifications with (Mascot scores of ≥ 34) 243 and a false discovery rate of < 3%. The following parameters were used: precursor mass tolerance, 1.5 244 Da; fragment mass tolerance, 0.6 Da; static modification, methylthio (C), iTRAQ 4-plex (K) and 245 iTRAQ 4-plex (N); and dynamic modification, iTRAQ 4-plex (Y) and oxidation (M). This resulted in 246 the identification of 1959 and 2402 unique peptides, respectively, from the first and second iTRAQ 247 experiments. The relative quantitation was measured as two pairwise ratios: the Normal group against 248 the Tumor group (iTRAQ 115/114 or iTRAQ 117/116). From the two iTRAQ experiments 14,199 and 249 8,618 MS/MS spectra were identified, leading to identification of 2,402 and 1,959 unique peptides with 250 ≥ 34 ion score and identification of 674 and 757 proteins for the respective groups (Supplemental data 251 2). A total of 512 and 473 proteins were quantified with at least 2 MS/MS spectra assigned. The 252 following criteria were applied to obtain differentially expressed proteins that displayed consistent 253 under-expression in the Normal group: (1) the proteins are identified by two biological replicates; (2) 254 the proteins have at least 2 quantified MS/MS spectra; (3) the iTRAQ 115/114 or iTRAQ 117/116 255 ratios must be both lower than 0.67; (3) the variation of coefficient of the iTRAQ ratio must be less 256 than 20%. The overall quality of the quantitation, and subsequent normalization, is revealed by a 257 careful consideration of the ratios for the duplicate analyses at the peptide level. Among the identified 258 proteins, 13 proteins displayed consistent under-expression in the Normal group (Table 1). To gain a 259 better understanding of the 13 proteins in this study, we performed a functional annotation analysis of 260 these proteins. The grouping and naming of the identified proteins in the functional annotation analysis 261 were performed according to the Gene Ontology convention [27]. 13 262 Quantification of the expression of the six candidate genes 263 Excluding ribosomal protein and the variability of both the 115/114 and 117/116 samples in 264 over 10% of the candidates, among the 13 proteins, we selected the epidermal growth factor receptor 265 (EGFR, coding for receptor tyrosine-protein kinase ErbB-1, EGFR), ornithine aminotransferase (OAT, 266 coding for Ornithine aminotransferase, OAT), tumor protein, translationally controlled 1 (TPT1, 267 coding for translationally controlled tumor protein, TCTP), integrin alpha-6 (ITGA6, coding for 268 Integrin alpha-6 precursor, ITGA6), Ras GTPase-activating protein-binding protein 1 (G3BP1, coding 269 for Ras GTPase-activating protein-binding protein 1, G3BP1) and calcium-binding protein 39-like 270 (CB39L, coding for Calcium-binding protein 39-like, CB39L). The transcript levels of these six genes 271 were validated in the paired tumor and normal tissues from 37 OSCC patients (T1=10, T2=10, T3, 272 n=10 and T4, n=7) by real-time quantitative PCR. The dynamic results suggested that all of the 273 candidate genes were overexpressed in the tumor tissues across all stages. Comparing the tumor and 274 corresponding normal tissues from the 37 oral cancer patients, the EGFR, OAT, TPT1, ITGA6, G3BP1 275 and CB39L genes were overexpressed by an average of 2.74-fold (95% CI, 1.53-3.25), 1.07-fold (95% 276 CI, 0.57-1.65), 3.42-fold (95% CI, 1.80-4.52), 5.65-fold (95% CI, 1.58-5.22), 1.33-fold (95% CI, 277 0.13-3.74) and 3.72-fold (95% CI, 1.08-4.22) in the tumor tissues, respectively (Figure 2A). These 278 results indicate that the overexpression phenomena differentiating the tumor and normal tissues in the 279 oral cancer patients were not only manifested at the tissue protein levels but also at the mRNA level. In 280 addition, three genes, TPT1, CAB39L and ITGA6, displayed stable and higher expression levels related 281 to gene transcription in the tumor tissues (with a 3-fold greater mean overexpression level). 282 Moreover, we organized the individual overexpression levels of TPT1, CAB39L and ITGA6 in 283 the T1-4 groups. The overexpression of TPT1gene was observed not only in the early stage but also 284 increased in the late stages from 4.51-fold (T1) and 4.3-fold (T2) to 4.62-fold (T3) and 5.74-fold (T4), 14 285 although the overexpression was not significantly different between T1 + 2 and T3 + 4 (p= 0.078). 286 Additionally, CAB39L and ITGA6 consistently displayed greater overexpression levels in the T1 and T2 287 groups (with 6.9- and 6.6-fold increases on average for ITGA6 and 4.7- and 5.1-fold increases for 288 CAB39L) in the tumor tissues (Figure 2B). However, lower transcription levels of these genes were 289 observed in the tumor tissues of the T3 and T4 patients (with 3.8- and 3.1-fold increases for ITGA6 on 290 average and 2.3- and 1.6-fold for CAB39L). These two genes displayed significant differences between 291 their mean transcription levels in the T1+T2 and T3+T4 groups (P=0.02024 for ITGA6, and P=0.00038 292 for CAB39L). These results indicated that tissue overexpression of CAB39L and ITGA6 were dominant 293 in the early stage and not correlated with oral cancer progression, which are important for early 294 diagnosis. 295 Validation of the protein expressions in the tissues 296 The protein expression levels of TPT1, ITGA6 and CAB39L were validated in the paired tumor 297 and normal tissues from 37 OSCC patients (T1=10, T2=10, T3, n=10 and T4, n=7). The results 298 suggested that all of the three proteins were overexpressed in the tumor tissues across all stages (Figure 299 3A). Comparing the tumor and corresponding normal tissues from the 37 oral cancer patients, the TPT1, 300 ITGA6 and CAB39L proteins were overexpressed by an average of 2.83-fold, 3.27-fold and 1.62-fold 301 in the tumor tissues, respectively (Figure 3B). 302 Predictions of the candidate miRNAs 303 The candidate microRNA predictions were based on the 3′UTRs of the TPT1, CAB39L and 304 ITGA6 genes using two bioinformatics tools, the mirSVR predicted target site scoring method [28] and 305 the online tools at MicroRNA.org (http://www.mirbase.org). All the individual candidate miRNAs were 306 reported (Table 2); we selected the seven overlapping miRNAs (miR-19a, miR-27a, miR-27b, miR-19b 307 and miR-186 miR-203, miR-377) underlined in bold font as candidate targets for the subsequent 15 308 miRNA determinations. 309 Quantitative analysis of candidate miRNA expression 310 In the tissue study comparing the paired normal and tumor tissues, the target miRNAs 311 miR-19a, miR-19b, miR-186, miR-203 and miR-377 were detected by real-time Q-PCR and showed 312 overexpression levels averaging 7.93-, 1.18-, 1.64-, 14.57- and 33.21-fold, respectively, in the tumor 313 tissues from the 20 patients. However, only the has-miR-27a and has-miR-27b were underexpressed in 314 the tumor tissues, by 0.57- and 0.32-fold on average, respectively (Figure 4A). Following the 315 introduction, the overexpressions of miRNA will reduce the target protein expressions after 316 transcriptions, thus we selected the has-miR-27a and has-miR-27b for advance detection. 317 The plasma levels of miR-27a and miR-27b were determined and compared in 10 normal 318 individuals and 20 oral cancer patients. Unlike the control, miR-16, which was found in all patients and 319 normal individuals, plasma miR-27a was detected in only 11 % (4 of 37) of the OSCC patients and in 320 only 25% (5 of 20) of the healthy volunteers under the same conditions. The data indicate that the 321 major expression of miRNA-27a in tissues does not translated to higher plasma levels. However, the 322 plasma miR-27b levels were detectable in 70 % (26 of 37) of the tumor patients and all the healthy 323 volunteers; the levels tended to be significantly higher in the normal group than in the oral cancer 324 group (P=0.00019; 95% confidence interval, 9.5-29.7; with a mean level 13.2-fold higher) (Figure 4B). 325 This result indicated that decreased plasma miR-27b levels are a significant indicator for oral cancer 326 and that the miR-27b suppression may involve the expression off the tumor-associated proteins TCTP, 327 CAB39L and ITGA6 in oral cancer. We also investigated possible correlations between plasma 328 miR-27b levels and sex, age and tumor size in the 37 patients; no significant associations were 329 observed. 330 Translational regulation of candidate proteins by miR-27b 16 331 To determine the effects of miRNA-27b on the expression of the TCTP, CAB39L and ITGA6 332 proteins, 100 nM of synthetic miR-27b was transfected into HSC-3 and Cal-27 cells. The 333 overexpression of miR-27b significantly decreased the expression of TCTP mRNA and protein in both 334 the HSC-3 and Cal-27 cell lines but did not significantly affect gene and protein expression in the 335 CAB39L and ITGA6, as determined by both Q-PCR and immunoblot assays (Figure 5A and B). These 336 results indicate that miRNA-27b expression is involved in the regulation of TCTP in oral cancer cells. 17 337 Discussion 338 In tumorigenesis and cancer progression, dynamic protein expression is always a critical target 339 for initial investigation. Recently, functional proteomics combined with mass spectrometry (MS) has 340 offered great promise for unveiling the complex molecular events of tumorigenesis and transforming 341 the management of cancer by identifying new markers for screening, diagnosis, prognosis, and 342 monitoring responses to therapy [29-31]. Following previous reports, the rapid advances in quantitative 343 proteomic analysis based on isotope-dilution MS with mass-tagging reagents, such as iTRAQ, in 344 addition to multidimensional liquid chromatography−tandem mass spectrometry (LC−MS/MS) have 345 revolutionized the field of biomarker discovery and identification [32, 33]. Gel-free approaches 346 LC-MS/MS have been widely used for clinical tissue and cell line analysis. iTRAQ reagents contain 347 isobaric tags designed to bind specifically to the amine groups of peptides, enabling their quantitation 348 by the measurement of relative intensities of the reporter ions generated upon MS/MS fragmentation. 349 To avoid possible analytical and methodological biases, a technology different from the one used for 350 biomarker discovery is typically employed. Real-time Q-PCR and immunoblots are robust, powerful 351 techniques that are frequently selected for biomarker verification. These techniques permit not only the 352 identification and verification of biomarkers but also their quantification in various tissues and body 353 fluids [27]. Studies evaluating the prognostic utility of potential biomarkers identified using gel 354 free-proteomic techniques are not rare and are also needed to substantiate advances in clinical utility 355 and elucidate the potential mechanisms of new biomarkers. 356 The mature 20- to 23-nt miRNAs act as functional intermediates of RNAi that direct mRNA 357 cleavage and translational attenuation, and recent studies suggest that miRNAs contribute to the 358 development of hand and neck cancers [19, 34]. Generally, the miRNA can be easily and quickly 359 determined using real-time Q-PCR and is more suitable as a potential biomarker than protein 18 360 biomarkers for clinical applications. Generally, mRNA profiling with microarrays has been widely 361 used for miRNA target identification, but microarrays only detect the effects of miRNAs at the 362 transcriptional level and will miss targets repressed solely at the protein level. However, methods based 363 on the use of miRNA profiling techniques to predict proteins levels are difficult to implement in a 364 high-throughput fashion. Thus, we designed a new platform to demonstrate the potential for the 365 prognostic applications of candidate biomarkers identified using tissue proteomics by iTRAQ analysis 366 and attempted to identify biomarkers related to target miRNAs to replace proteins as useful biomarkers 367 for oral cancer. 368 In the iTRAQ analysis, we identified and quantified a total of 13 down-regulated and 6 369 up-regulated proteins with consistently different expression from the Normal tissue group. The 6 370 up-regulated proteins have been identified for future work in another study. In this study, we focus on 371 the 13 down-regulated proteins and the characterization of their mRNA- and miRNA-associated 372 expression levels in tissues and plasma. Moreover, we integrated in vivo and in vitro studies to 373 demonstrate that the expression of miR-27b significantly affects the downregulation of the TCTP 374 protein, one of the three candidate biomarkers. The developed platform represents the first combined 375 application of a differentially expressed tumor proteomic study to the identification of miRNA 376 biomarkers. Until now, there have been no reports of the identification of potential miRNA biomarkers 377 based on protein data from iTRAQ analysis in cancer research utilizing two types of quantitation. This 378 novel plateform can facilitate simultaneous screening for potentially correlated genes, miRNA and 379 downstream proteins. 380 Among of the 13 underexpressed proteins, we selected 6 proteins for subsequent study. The 381 expression of their coding genes, EGFR, OAT, TPT1, ITGA6, G3BP1 and CAB39L, were confirmed by 382 real-time quantitative PCR analysis. The TPT1, ITGA6 and CB39L genes were found to be the most 19 383 consistently over-expressed in the tumor tissues, and we suggest that detecting the these three genes 384 could contribute considerably to the early diagnosis of oral cancer (T1 or T2). Excluding TPT1, the 385 QPCR results for the ITGA6 and CB39L genes demonstrated that their over-expression appears more 386 significantly in the early stages of oral cancer (T1+T2) than in the late stages (T3+T4) (Figure 2). In 387 previous studies, the TPT1, ITGA6 and CB39L genes were reported to be implicated in tumor growth, 388 malignancy and poor survival rates in breast cancer and monocytic leukemia [35-37], but the studies 389 have not reported the protein levels and correlated miRNAs associated with cancer. The three 390 tumor-related proteins and genes were also demonstrated for the first time here to be useful as the 391 biomarkers for oral cancer based on a clinical global quantitative proteomic analysis. The correlation of 392 Q-PCR data with protein expression provides evidence that the iTRAQ labeling method for large-scale 393 protein quantification is powerful and reliable for advanced miRNA biomarker profiling. 394 It is known the miRNAs can control the expression levels of particular genes by binding to the 395 3′UTRs of mRNAs. Thus, the dysregulation of miRNAs is expected to be found in diseases such as 396 cancer that are attributed to deregulated gene expression, suggesting that miRNA alteration may initiate 397 carcinogenesis [38]. However, there is limited information on the aberrant expression of miRNAs in 398 oral cancer [39]. Among the 7 miRNAs that were predicted for the TPT1, CAB39L and ITGA6 genes in 399 a bioinformatic analysis, miR-27a and miR-27b demonstrated consistent under-expression in the laser 400 pressure catapulting dissected tumor tissues in comparison with the corresponding normal tissues; 401 unfortunately, the miR-27a was found in too few plasma samples in the oral cancer patients to be 402 statistically significant in this group. Specially, the tissue related determinations were carried out after 403 the laser pressure catapulting dissection that has been reported is the best tool to define the malignant 404 and benign sample in the translational medicine. Thus, we focused on miR-27b in this study. The 405 aberrant expression of miRNAs has been implicated in the carcinogenesis of various cancers. In 20 406 previous studies, an up-regulation of miR-27b was observed in OSCC and breast cancers as the tumors 407 suppress various factors in genomic experiments, but the effects of miR-27b on the regulation of 408 intercellular proteins in oral tumorigenesis remains unclear [40, 41]. 409 As established in previous studies, TCTP is a highly conserved protein expressed abundantly 410 across a wide range of eukaryotes and is known to promote diverse cellular functions by interacting 411 with various proteins, with expression levels varying depending on the tissue type, growth, stress 412 factors and cytotoxic signals [42]. Knocking down TCTP protein expression in tumor cells inhibits 413 their growth, motility and invasive functions, and its expression levels have been demonstrated to be 414 downregulated by the activation of the tumor suppressor protein p53 [43, 44]. It also has been 415 suggested that several breast tumor cell lines, including MCF-7 and T47D, have high endogenous 416 levels of TCTP protein, and siRNA transfection promotes the downregulation of TCTP, resulting in 417 tumor reversion. However, the molecular mechanisms of tumor reversion remain to be defined. 418 Recently, TCTP was demonstrated to induce the chronic activation of Src, and EGFR and downstream 419 signaling molecules associated with cell transformation were significantly down-regulated by TCTP 420 siRNA [45]. It thus appears that the down-regulation of TCTP quenches the activation of 421 tumor-associated signals, causing tumor reversion [46, 47]. So far, it has not been investigated 422 whether the TCPT protein or the TPT1 gene can be regulated by miRNAs. 423 Thus, we performed transient transfection to overexpress the human miR-27b in oral cancer cell 424 lines to identify its regulatory role. This is the first report demonstrating that miR-27b is a negatively 425 regulator of the expression the of TPT1 gene and TCPT protein. We further demonstrated that miR-27b 426 overexpression not only reduced the level of TPT1 gene expressions and also downregulates cellular 427 TCPT expression in the oral cancer cells (Figure 4), but also that gene and protein levels of CAB39L 428 and ITGA6 are not significantly regulated by miR-27b overexpression, although the miR-27b sequence 21 429 was predicted from these three genes’ 3-UTR. These interesting and varied regulatory mechanisms 430 require further study to clarify their roles in cancer cells. 431 Our results indicate that miR-27b may function as a tumor-suppressor gene, whereas another 432 study suggested it may function as an oncogene in MDA-MB-231 cells [47]. They revealed that the 433 introduction of miR-27b into cells expressing the target gene, ST14, did not suppress cell growth, 434 suggesting that both miR-27b-dependent and independent functions of ST14 protein exist in breast 435 cancer. Furthermore, the miR-19a, miR-19b, miR-20a and miR-27b sequences were identified as the 436 major growth-sustaining micro-RNAs in the tumor cells in an assay of individual cell growth arrest 437 [48]. The complementary screening study unveiled only functional differences between homologous 438 mi-RNAs; miR-27b appears to be involved in an important novel mechanism in tumorigenesis. These 439 differences may occur due to differences in cancer types, patient organization, tumor status or 440 histologic tumor grade, etc. 441 Conclusion 442 Our study introduced the efficient use of an iTRAQ proteomics study to identify three protein 443 biomarkers for early stage oral cancer. We additionally discovered that tissue and plasma miR-27b 444 levels are better biomarkers than protein biomarkers due to their convenient determination by Q-PCR, 445 and that miR-27b overexpression in oral cancer cells significantly down-regulates the tumor associated 446 TCTP protein. The integrated study of quantitative proteomics and molecular biology will provide new 447 insights in both Proteomics and Translational medicine. 448 449 450 451 Acknowledgements This study was supported by grants from the National Science Council (NSC 96-2320-B-039-024, 22 452 NSC 97-2320-B-039-016-MY3, and NSC 98-2113-M-003-007-MY2), the China Medical University 453 Hospital (DMR-98-100) and China Medical University (CMU100-S-04). 454 23 455 References 456 1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J 457 458 459 460 461 462 Clin 2011;61(2):69-90. 2. Seiwert TY, Cohen EE. State-of-the-art management of locally advanced head and neck cancer. Br J Cancer 2005;92(8):1341-8. 3. Ho PS, Ko YC, Yang YH, Shieh TY, Tsai CC. The incidence of oropharyngeal cancer in Taiwan: an endemic betel quid chewing area. J Oral Pathol Med 2002;31(4):213-9. 4. Chen YJ, Chang JT, Liao CT, Wang HM, Yen TC, Chiu CC, et al. Head and neck cancer in the 463 betel quid chewing area: recent advances in molecular carcinogenesis. 464 2008;99(8):1507-14. Cancer Sci 465 5. Turhani D, Krapfenbauer K, Thurnher D, Langen H, Fountoulakis M. Identification of 466 differentially expressed, tumor-associated proteins in oral squamous cell carcinoma by proteomic 467 analysis. Electrophoresis 2006;27(7): 1417–23. 468 469 6. Gstaiger M, Jordan R, Lim M, Catzavelos C, Mestan J, Slingerland J, et al. Skp2 is oncogenic and overexpressed in human cancers. Proc Natl Acad Sci U S A 2001;98(9):5043–8. 470 7. Huang X, Gollin SM, Raja S, Godfrey TE. High-resolution mapping of the 11q13 amplicon and 471 identification of a gene, TAOS1, that is amplified and overexpressed in oral cancer cells. Proc Natl 472 Acad Sci U S A 2002;99(17):11369–74. 473 8. Sugimura T, Kumimoto H, Tohnai I, Fukui T, Matsuo K, Tsurusako S, et al. Gene–environment 474 interaction involved in oral carcinogenesis: molecuar epidemiological study for metabolic and 475 DNA repair gene polymorphisms. J Oral Pathol Med 2006;35(1):11–8. 476 9. Kallioniemi O. Medicine: profile of a tumour. Nature 2004;428(6981):379–82. 24 477 478 10. Geho DH, Petricoin EF, Liotta LA. Blasting into the microworld of tissue proteomics: a new window on cancer. Clin Cancer Res 2004;10(3):825–7. 479 11. Garbis SD, Tyritzis SI, Roumeliotis T, Zerefos P, Giannopoulou EG, Vlahou A, et al. Search for 480 potential markers for prostate cancer diagnosis, prognosis and treatment in clinical tissue specimens 481 using amine-specific isobaric tagging (iTRAQ) with two-dimensional liquid chromatography and 482 tandem mass spectrometry. J Proteome Res 2008;7(8):3146-58. 483 12. Wu WW, Wang G, Baek SJ, Shen RF. Comparative study of three proteomic quantitative methods, 484 DIGE, cICAT, and iTRAQ, using 2D gel- or LC-MALDI TOF/TOF. J Proteome Res 485 2006;5(3):651-8. 486 13. Ross PL, Huang YN, Marchese JN, Williamson B, Parker K, Hattan S, et al. Multiplexed protein 487 quantitation in Saccharomyces cerevisiae using amine-reactive isobaric tagging reagents. Mol Cell 488 Proteomics 2004;3(12):1154-69. 489 14. Ralhan R, Desouza LV, Matta A, Chandra TS, Ghanny S, Dattagupta S, et al. 490 iTRAQ-multidimensional 491 identification of potential biomarkers of oral epithelial dysplasia and novel networks between 492 inflammation and premalignancy. J Proteome Res 2009;8(1):300-9. 493 494 495 liquid chromatography and tandem mass spectrometry-based 15. Lewis BP, Burge CB, Bartel DP. Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell 2005;120(1):15–20. 16. Hsieh HC, Chen YT, Li JM, Chou TY, Chang MF, Huang SC, Protein Profilings in Mouse Liver 496 Regeneration after Partial 497 2009;8(2):1004-13. Hepatectomy using iTRAQ Technology. J Proteome Res 498 17. Farh KK, Grimson A, Jan C, Lewis BP, Johnston WK, Lim LP, et al. The widespread impact of 499 mammalian MicroRNAs on mRNA repression and evolution. Science 2005;310(5755):1817–21. 25 500 501 502 503 504 505 506 507 508 509 18. Cullen BR. Transcription and processing of human microRNA precursors. Mol Cell 2004;16(6):861–5. 19. Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat Rev Cancer 2006;6(11):857–66. 20. Gomes CC, Gomez RS. MicroRNA and oral cancer: future perspectives. Oral Oncol 2008;44(10):910-4. 21. Lima RT, Busacca S, Almeida GM, Gaudino G, Fennell DA, Vasconcelos MH. MicroRNA regulation of core apoptosis pathways in cancer. Eur J Cancer 2011;47(2):163-74. 22. Kouwenhove MV, Kedde M, Agami R. MicroRNA regulation by RNA-binding proteins and its implications for cancer. Nat Rev Cancer 2011;11(9):644-56. 510 23. Uesugi A, Kozaki K, Tsuruta T, Furuta M, Morita K, Imoto I, et al. The tumor suppressive 511 microRNA miR-218 targets the mTOR component Rictor and inhibits AKT phosphorylation in oral 512 cancer. Cancer Res 2011;71(17):5765-78. 513 514 24. Hanash SM, Pitteri SJ, Faca VM. Mining the plasma proteome for cancer biomarkers. Nature 2008;452(7187):571–9. 515 25. Faca VM, Song KS, Wang H, Zhang Q, Krasnoselsky AL, Newcomb LF, et al. A mouse to human 516 search for plasma Proteome changes associated with pancreatic tumor development. PLoS Med 517 2008;5(6):953–967. 518 26. Lo WY, Tsai MH, Tsai Y, Hua CH, Tsai FJ, Huang SY, et al. Identification of over-expressed 519 proteins in oral squamous cell carcinoma (OSCC) patients by clinical proteomic analysis. Clin 520 Chim Acta 2007;376(1-2):101-7. 521 27. Chen WT, Chang SC, Ke TW, Chiang HC, Tsai FJ, Lo WY. Identification of Biomarkers to 522 Improve Diagnostic Sensitivity of Sporadic Colorectal Cancer in Patients with Low Preoperative 26 523 Serum Carcinoembryonic Antigen by Clinical Proteomic Analysis. Clin Chim Acta 524 2011;412(7-8):636-41. 525 526 28. Betel D, Koppal A, Agius P, Sander C, Leslie C. Comprehensive modeling of microRNA targets predicts functional non-conserved and non-canonical sites. Genome Biology 2010;11:R90. 527 29. Cho WC. Contribution of oncoproteomics to cancer biomarker discovery. Mol Cancer 2007;6:25. 528 30. Tanke HJ. Genomics and proteomics: the potential role of oral diagnostics. Ann. N.Y. Acad. Sci 529 2007;1098:330-334. 530 31. Najam-ul-Haq M, Rainer M, Trojer L, Feuerstein I, Vallant RM, Huck CW, et al. Alternative 531 profiling platform based on MELDI and its applicability in clinical proteomics. Expert Rev of 532 Proteomics 2007;4(4):447-52. 533 534 32. Zieske LR. A perspective on the use of iTRAQ reagent technology for protein complex and profiling studies. J Exp Bot 2006;57(7):1501-8. 535 33. DeSouza LV, Grigull J, Ghanny S, Dubé V, Romaschin AD, Colgan TJ, et al. Endometrial 536 carcinoma biomarker discovery and verification using differentially tagged clinical samples with 537 multidimensional liquid chromatography and tandem mass spectrometry. Mol Cell Proteomics 538 2007;6(7):1170-82. 539 540 34. Chen LH, Tsai KL, Chen YW, Yu CC, Chang KW, Chiou SH, et al. MicroRNA as a Novel Modulator in Head and Neck Squamous Carcinoma. J Oncol 2010;2010:135632. 541 35. Jung J, Kim HY, Kim M, Sohn K, Kim M, Lee K. Translationally controlled tumor protein induces 542 human breast epithelial cell transformation through the activation of Src. Oncogene 543 2011;30(19):2264-74. 544 36. Cariati M, Naderi A, Brown JP, Smalley MJ, Pinder SE, Caldas C. Purushotham A. D. Alpha-6 545 integrin is necessary for the tumourigenicity of a stem cell-like subpopulation within the MCF7 27 546 breast cancer cell line. Int J Cancer 2008;122(2):298-304. 547 37. Zhang PY, Zhang WG, He AL, Wang JL, Li WB. Identification and functional characterization of 548 the novel acute monocytic leukemia associated antigen MLAA-34. Cancer Immunol Immunother 549 2009;58(2):281-90. 550 551 38. Calin GA, Croce CM. MicroRNA signatures in human cancers. Nat Rev Cancer 2006;6(11):857–66. 552 39. Komatsu S, Ichikawa D, Takeshita H, Tsujiura M, Morimura R, Nagata H, et al. Circulating 553 microRNAs in plasma of patients with oesophageal squamous cell carcinoma. Br J Cancer 554 2011;105(1):104-11. 555 556 557 558 40. Kozaki K, Imoto I, Mogi S, Omura K, Inazawa J. Exploration of tumor-suppressive microRNAs silenced by DNA hypermethylation in oral cancer. Cancer Res 2008;68(7):2094-105. 41. Tsuchiya Y, Nakajima M, Takagi S, Taniya T, Yokoi T. MicroRNA regulates the expression of human cytochrome P450 1B1. Cancer Res 2006;66(18):9090-8. 559 42. Chen S. H.; Wu P. S.; Chou C. H.; Yan Y. T.; Liu H.; Weng S. Y.; Yang-Yen H. F. A knockout 560 mouse approach reveals that TCTP functions as an essential factor for cell proliferation and 561 survival in a tissue- or cell type-specific manner. Mol Biol Cell. 2007, 18(7), 2525-32 562 43. Tuynder M.; Fiucci G.; Prieur S.; Lespagnol A.; Géant A.; Beaucourt S.; Duflaut D.; Besse S.; 563 Susini L.; Cavarelli J.; Moras D.; Amson R.; Telerman A. Translationally controlled tumor protein 564 is a target of tumor reversion. Proc Natl Acad Sci U S A. 2004, 101(43), 15364-9 565 44. Tuynder M.; Susini L.; Prieur S.; Besse S.; Fiucci G.; Amson R.; Telerman A. Biological models 566 and genes of tumor reversion: cellular reprogramming through tpt1/TCTP and SIAH-1. Proc Natl 567 Acad Sci U S A. 2002, 99(23), 14976-81 568 45. Jung J.; Kim H. Y.; Kim M.; Sohn K.; Kim M.; Lee K. Translationally controlled tumor protein 28 569 induces human breast epithelial cell transformation through the activation of Src. Oncogene. 2011, 570 30(19), 2264-74 571 572 46. ZOU G. M. Cancer initiating cells or cancer stem cells in the gastrointestinal tract and liver. J Cell Physiol. 2008, 217(3), 598-604. 573 47. Wang Y.; Rathinam R.; Walch A.; Alahari S. K. ST14 (suppression of tumorigenicity 14) gene is a 574 target for miR-27b, and the inhibitory effect of ST14 on cell growth is independent of miR-27b 575 regulation. J Biol Chem. 2009, 284(34), 23094-106 576 577 48. Peric D.; Chvalova K.; Rousselet G. Identification of microprocessor-dependent cancer cells allows screening for growth-sustaining micro-RNAs. Oncogene. 2011, 1-10 578 29