Review of Systems form
advertisement

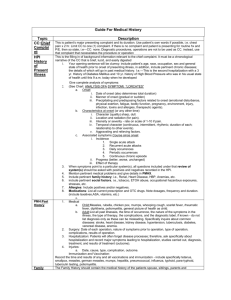
Fulton Family Health Associates, P.C. 2613 Fairway Dr, Suite C, Fulton, MO. 65251 Phone: (573) 642-1990 Fax: (573) 642-5089 Robert P. Pierce, M.D. Andra M. Walker, PA-C Lisa J. Pierce, M.D. Ashlea E. Horstman, PA-C Brice P. Windsor, D.O. REVIEW OF SYSTEMS Patient Name: _______________________________________ PLEASE CHECK ALL SYMPTOMS THAT APPLY: CONSTITUTIONAL: Weight Gain Weight loss Fatigue Weakness Fever Chills Night sweats Loss of appetite EYES: Vision problems Blurred vision Double vision Pain Redness Excessive tearing Dry eyes EARS, NOSE, MOUTH, THROAT: Hearing loss Ringing in ears Ear pain Discharge from ears Vertigo Runny nose Nasal congestion Bloody noses Bleeding gums Sore tongue Sore throat Hoarse voice Mouth lesions CARDIOVASCULAR: Chest pain or pressure Frequent irregular beats Shortness of breath with exertion Shortness of breath with laying flat Wake up short of breath Swelling in legs RESPIRATORY: Wheezing Cough Productive cough Coughing up blood GASTROINTESTINAL: Abdominal pain Nausea Vomiting Diarrhea Constipation Heart burn Vomiting blood Black/ tarry stools Jaundice Passing blood Pain with swallowing GENTITOURINARY: MALES & FEMALES: Burning with urination Urgency Frequency Blood in urine Frequent urination at night Incontinence Reduced stream Urinary hesitancy FEMALES: Last menstrual period: _________ Absence of periods Irregular periods Heavy periods Pain with periods Vaginal discharge Pain with intercourse Bleeding after intercourse Hot flashes MALES: Penile discharge Penile lesions Erectile dysfunction MUSCULOSKELETAL: Excessive joint pain Joint swelling SKIN AND/ OR BREAST: Rash Lumps Changing moles Date: ______/______/______ SKIN AND/ OR BREAST (cont.) : Itching Nail changes Breast pain Breast lumps Nipple discharge NEUROLOGICAL: Headache Fainting Near fainting Paralysis Weakness Tremor PSYCHIATRIC: Disorientation/ confusion Nervousness Restlessness Anxiousness Impaired recent memory Impaired remote memory Trouble sleeping Increased sleep Obsessions Delusions Hallucinations ENDOCRINE: Excessive urination Excessive thirst Cold intolerance Heat intolerance Excessive sweating HEMATOLOGIC/ LYMPHATIC: Easy bruising or bleeding Bloody nose Enlarged lymph nodes ALLERGIC/ IMMUNOLOGIC: Hives Clear nasal discharge Recurrent infections Sneezing QUESTIONS Average drinks per day? _______________ MEN: Last time you had more than 5 drinks in one sitting? (circle one) : Never > 1 year < 1 year < 3 months < 30 days WOMEN: Last time you had more than 4 drinks in one sitting? (circle one) : Never > 1 year < 1 year < 3 months < 30 days In the past month, have you often been bothered by feeling depressed, down or hopeless? (circle one) : YES NO In the past month, have you often bothered by little interest or pleasure in doing things? (circle one) : YES NO