NRP_megacode
advertisement

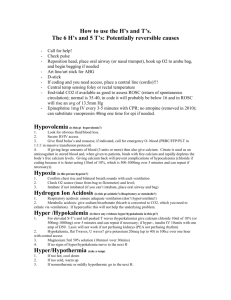
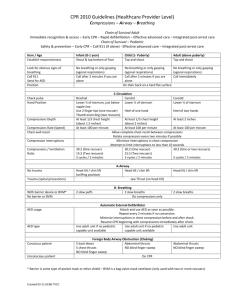
CSC Standardized Curriculum Specialty: Pediatrics Simulation: Neonatal resuscitation (NRP) megacode Submitted by: MAJ Taylor Sawyer Target Audience: Pediatric, Family Medicine, Obstetric/Gynecology residents and Pediatric, Family Medicine, Obstetric/Gynecology Medicine staff ACGME Competencies Addressed: Patient Care Medical Knowledge Practice-Based Learning & Improvement Professionalism RRC Requirements Addressed: Basic and advanced life support Endotracheal intubation Umbilical artery and vein catheterization Case Scenarios Primary: The participants are called to attend the spontaneous vaginal delivery of a 42 week infant with an estimated fetal weight of 4500gms. The mother is a G1PO 35 yo with a history of poorly controlled A2GDM. Prenatal history and labs are otherwise unremarkable. Mother has been in labor for 10 hours and within the last 10 minutes the fetal heart rate tracing has become concerning for late decelerations. Amniotic fluid was clear at SROM. The infant requires forceps assist at delivery and is placed on warmer limp, cyanotic and apneic. Alternate scenario The participants are called to attend a crash C-section of a 39 week infant with a estimated fetal weight of 3500 gms. The mother was seen in labor and delivery triage due to report of decreased fetal movement and fetal heart rate on doppler was 50. Amniotic fluid was clear at AROM. At delivered the infant is noted to have tight nucal cord x 2 requiring surgical reduction. The infant is delivered to the warmer limp, cyanotic and apneic Version 1, 4/11/2008 Basic Instructions for participants Please read the scenario and then enter the room when instructed by your staff. You may ask questions if you have them, and please remember to: 1. Treat the situation as realistically as possible. 2. Think out loud, vocalize abnormal/critical findings, state the doses of drugs, and declare differential diagnoses you are considering. Only with this behavior can we evaluate you and make sure you succeed. 3. If you have questions about the simulation or manikin ask the supervisor 4. If you need further patient information, ask; do not make assumptions; do not declare the answers/results to physical finding/labs without asking 5. Assume that you can request any resource you would have available in the hospital in which you are training. Simulation Setup Simulators to be used: Gaumard PEDI® Blue Neonatal Simulator Simulation Location: Labor and delivery room for primary scenario. Operating room for alternate scenario. Room Setup: The labor and delivery room or OR should be set up in the standard fashion with mother’s bed and infant warmer. The Gaumard NOELLE™ Maternal Simulator can be placed in the bed and confederates acting as obstetricians can be dressed gowns and gloves simulating the delivery. The infant simulator should be delivered to the warmer by obstetrician as in a real delivery. The room should be stocked with the usual instruments (bag-valve mask, laryngoscope, ET tubes, buld suction, De lee suction, etc.) and medications (epinephrine 1:10,000, 4.2% sodium bicarbonate, Normal saline, etc.) used in a delivery/resuscitation. Additional Equipment needed: - Birthing simulator: Gaumard NOELLE™ Maternal Simulator - Infant warmer - Standard Neonatal resuscitation equipment including: Bulb suction Bag-valve mask Laryngoscope ET tubes (2.5-4.0) Stylet De-lee suction catheter and tubing Version 1, 4/11/2008 2 Umbilical line kit Umbilical catheter Syringes Medications: epinephrine, bicarbonate, normal saline Optional Equipment: - Fetal Monitoring: Gaumard NOELLE™ Maternal Simulator includes a fetal monitor that may be used in the primary scenario to produce fetal bradycardia. Personnel needed: - Gaumard PEDI® Blue technician to operate controls and umbilical pulse - Confederates to act as obstetricians and OR personnel : 2-3 - Bedside nurse: 1 - Scenario supervisor: 1 - Scenario grader: 1 Basic Scenario Tips: Participants should be paged STAT on the regular delivery pagers to the DR or OR you are using for simulation. Upon arrival the residents should be given a brief history by one of the confederate obstetrician. Give the participants 60 seconds to set up the warmer and equipment prior to ‘delivering’ the baby. When the infant is delivered it should be walked by the confederate obstetrician and placed on the warmer. Once on the warmer the PEDI® Blue technician will need to operate the controls for HR, and cyanosis. Umbilical pulse will need to be simulated using the hand pump for this manikin. Case Flow/Algorithm with branch point and completion criteria: Initial state: (both scenarios) Apperance= central cyanosis (Blue lights on both face and hand with PEDI® Blue) Pulse = 30 (selected on PEDI® Blue control and simulated with hand pump) Grimace= none Activity/tone = limp Respirations = absent In both scenarios the infant is born basically lifeless, except a slow pulse. Participants must proceed through the complete NRP resuscitation algorithm (see ‘Brief Didactic’ for review) including the placement of an emergency umbilical vein catheter (or IO line for the very intrepid) and administration of IV epinephrine before clinical status improves (HR increases to 150, central cyanosis resolves). Endotracheal epi administration does not change scenario. Version 1, 4/11/2008 3 Case Flow/Algorithm: INITIAL STATE: HR: 30 No respiratory effort Limp Cyanotic + No change - Dry and stimulate infant No change + No change No change - Bag/mask ventilation + No change Chest compressions No change - + No change - Intubation No change + No change Endotracheal Epi - No change HR to 150 Central cyanosis resolves + Epi given via umbilical vessel catheter No change + - No change if given NS bolus given via umbilical vessel catheter No change if given No change + Version 1, 4/11/2008 Bicarbonate via umbilical vessel catheter - No change 4 Critical Actions 1. Must warm, dry and stimulate infant 2. Must re-position airway 3. Must provide at least 30 seconds EFFECTIVE positive pressure ventilation before moving to chest compressions, intubation, line placement, drugs, etc. (40-60 breaths/min) 4. Must use 100% FIO2 during the resuscitation 5. Must provide positive pressure via BVM with good hand position and seal of mask on face* 6. Must check for HR and communicate rate to code leader 7. Must give compressions once HR is < 60 BPM and positive pressure ventilation has not been successfully delivered x 30 seconds 8. Must use proper chest compression technique (two finger or hand around chest) Check depth with compression gauge on PEDI® Blue 9. Must use proper ratio of chest compressions/ventilations 3:1, 90 compressions:30 ventilations per minute 10. Must place emergency umbilical vein catheter using sterile technique 11. Must pre-flush UVC with fluid to avoid air embolus 12. Must give proper dose/concentration of epinephrine via umbilical catheter followed by 2-3ml of flush before HR will rise back above 30 bpm 13. Must use correct IV epinephrine dose: 0.1-0.3 ml/kg (0.01-0.03 mg/kg) of 1:10,000 Please note 2005 NRP dosing for endotracheal epinephrine = 0.3-1ml/kg * Intubation not required if team thinks they are providing adequate ventilation with BVM, but should be considered when infant does not improve with BVM alone. Version 1, 4/11/2008 5 Common pitfalls to monitor for: Not position airway correctly- ‘sniffing position’ Not providing at least 30 seconds EFFECTIVE positive pressure ventilation before moving to chest compressions, and meds Improper hand position and/or poor seal of mask on face Not communicating HR rate to code leader Not using NRP ratio of chest compressions/ventilations Not using sterile technique during emergency umbilical vein catheter placement Not pre-flushing UVC prior to placement in order to avoid air embolus Not using proper dose/concentration of epinephrine Not continuing chest compressions and ventilation for at least 30 seconds after epinephrine dose Version 1, 4/11/2008 6 Physician # / Name ____________________________ Date _______________________ Training Site __________________________________ Grader __________________ Training Level: (Circle One) Fellow Staff PGY-1 PGY-2 PGY-3 Completed Not Completed Indeterminate History/Preperation (4 points) Obtains relevant history (2 point) Prepares infant warmer prior to delivery (2 point) Physical Exam (6 points) Recognizes cyanosis (1 points) Recognizes apnea (2 point) Recognizes bradycardia (3 points) Diagnostic evaluation (3 points) Recognizes secondary apnea (3 points) Management (11 points) Warms, dries and stimulates infant to breath (1 points) Provides PPV via BVM (3 points) Provides chest compression and ventilation in a 3:1 ratio (2 points) Places emergency umbilical venous catheter (UVC) (3 points) Gives correct dose of epinephrine via emergency UVC (2 points) Version 1, 4/11/2008 7 Completed Not completed Indeterminate Time goals (6 points) Starts PPV via BVM within 30 seconds of birth (3 points) Gives IV epinephrine within 10 minutes of birth (3 points) Incorrect Incorrect Actions and Interventions Starts chest compressions prior providing 30 seconds of PPV (-2 points) Does not intubate infant after PPV via BVM fails to improve the heart rate (-2 points) Gives incorrect dose of epinephrine (-3 points) Scenario score: Assign points for all items checked as ‘Completed’ or ‘Incorrect”. No points are given for “Not completed” and ‘Indeterminate’ actions. (Maximum points possible for this scenario = 30) Correct action points = _____ Incorrect action points = _____ Total scenario points = _____ Percent scenario score (Total scenario points /30) = _____ Overall scenario performance rating: 1 (poor) 2 (fair) Version 1, 4/11/2008 3 (good) 4 (Very good) 5 (Excellent) 8 Please answer the following questions about this provider’s performance: 1. Provider performed airway evaluation in timely fashion Strongly Disagree 0 1 2 Neither agree Or disagree 3 4 5 6 Strongly Agree 7 8 9 10 2. Respiratory status exam was accurate and complete Strongly Disagree 0 1 2 Neither agree Or disagree 3 4 5 6 Strongly Agree 7 8 9 10 3. Provider initiated appropriate diagnostic evaluation in a timely fashion Strongly Disagree 0 1 2 Neither agree Or disagree 3 4 5 6 Strongly Agree 7 8 9 10 4. Provider made appropriate therapeutic decision Extremely Poor 0 1 Average 2 3 4 5 6 Outstanding 7 8 9 10 4. How prepared do you feel the provider was to manage this scenario? Not prepared at all 0 1 Reasonably prepared 2 3 4 5 6 Very prepared 7 8 9 10 Perceived competency: Not competent to handle a similar scenario on a patient even with supervision* Competent to handle a similar scenario on a patient with supervision Competent to handle a similar scenario on a patient independently Competent to teach others about this scenario * If student not competent to perform procedure please refer for remedial simulation training Version 1, 4/11/2008 9 Key Teaching Points/Critical Actions to discuss in debriefing: - Discuss primary and secondary apnea Primary: resolves with stimulation Secondary: does not resolve with stimulation- Needs PPV! - Discuss/review the NRP algorithm and any deviations - Demonstrate proper performance of chest compressions and proper ratio of compressions/ventilations - 3:1 coordinated - Review epinephrine dosage, concentration and routes of administration. According to the 2005 NRP Textbook intravenous dosing is the preferred route. - Emphasize importance of crisis resource management skills Emphasize importance of EFFECTIVE positive pressure ventilation as the corner stone of NRP Suggested time length for modules: Total time: up to 30 minutes. 10 min simulation 20 min feedback session Brief Didactic: NRP flow: Ventilation rate: 40-60 breaths/min Compression rate: 120 events/min (90 compressions interspersed with 30 ventilations). Compression-ventilation rate: 3:1 coordinated (pause compressions for ventilation). Version 1, 4/11/2008 10 Medications (epinephrine, volume): Indicated if heart rate remains <60 bpm despite adequate ventilation with 100% oxygen and chest compressions. 30 second intervals between each step NRP Algorithm: (Taken from Neonatal Resuscitation Textbook, 5th Ed. 2005) Version 1, 4/11/2008 11 ET Tube Size and Depth of Insertion: Weight (g) Gestational Age (wk) Blade ET Size (mm) Insertion Depth (cm) Below 1000 < 25 00 2.5 6-7 1000-2000 30- 35 0 3.0 7-8 2000-4000 35-40 0-1 3.5 8- 9 >4000 >40 1 4.0 9-10 ETsize: equal to gest age: 25wks=2.5 tube, 30 wks= 3.0 tube, 35wk-3.5 tube, etc. ET Depth: 6cm + weight in Kg: 1kg= 7 cm at lip, 2 kg= 8cm at lip, 3kg= 9cm at lip, etc. NRP Medications: Medications Dose/Route Epinephrine IV (UVC preferred) Concentration Wt (kg) 1:10,000 1 IV Volume (ml) 0.1-0.3 2 0.2-0.6 Give rapidly followed by NS flush 3 0.3-0.9 Repeat q3-5 min 4 0.4-1.2 Higher dose for ET route 1 10 2 20 3 30 Indicated for hypovolemic shock (cord accident, abruption, etc.) 4 40 IV: 0.10.3ml/kg Higher IV doses not recommended Precautions ET: 0.3-1ml/kg Volume expanders Sodium Bicarb 10 ml/kg IV 1-2 meq/kg IV Version 1, 4/11/2008 0.5 meq/ml 1 2-4 (4.2% solution) 2 4-8 Give over 5-10 minutes Reassess after bolus Establish adequate ventilation first 12 Naloxone 0.1mg/kg Neonatal vial: 0.4 mg/ml IV or IM preferred route 4 8-16 1 0.25 2 0.50 3 0.75 4 Adult vial: 1 mg/ml 2ml/kg, D10W IV 6-12 Only for prolonged NRP Slow push over 2 min Address ventilation first with routine measures: PPV Repeat q2-3min ET route not recommended Dextrose (10% solution) 3 0.1g/ml 1 1 0.1 2 0.2 3 0.3 4 1 0.4 2 2 4 3 6 4 8 Caution in opioid addiction- can cause seizure Check bedside glucose. Positive pressure Ventilation: Indications: Positive pressure ventilation with the Bag-valve mask is THE most critical skill to learn in NRP. PPV should be provided to all infants who do not establish good respiratory effort after 30 seconds of warming and stimulation. The provision of effective PPV via BVM will resolve secondary apnea and result in improvement in HR and respiratory effort in the vast majority of depressed neonates. Review with participants the correct mask fit and positioning: Version 1, 4/11/2008 13 (Taken from Neonatal Resuscitation Textbook, 5th Ed. 2005) Chest Compressions: Indications: Heart rate is less than 60 beats per minute after 30 seconds of EFFECTIVE positive pressure ventilation. If BVM not effective then intubate and give PPV x 30 seconds before going to compressions. Heart rate is evaluated by either auscultation or palpation at the umbilicus or brachial artery. Compression Technique: Chest compressions should be performed over the lower half of the sternum. Version 1, 4/11/2008 14 (Taken from Neonatal Resuscitation Textbook, 5th Ed. 2005) Compression on the xiphoid process can cause trauma to the liver, spleen, or stomach, and must be avoided. The effectiveness of compressions can be maximized by attention to the following: The chest should be depressed by one-third to one-half of its anterior-posterior diameter with each compression. The optimum rate of compressions is 90 per minute. Each compression and decompression phase should be of equal duration. Chest compressions may be performed with either two fingers or with the two thumbencircling hands technique. Two fingers technique is recommended when there is a single rescuer. Compressions are performed with two middle fingers, placed on the sternum just below the nipples. Two hands encircling chest technique recommended when there are two rescuers. The thorax is encircled with both hands and cardiac compressions are performed with the thumbs of both hands. The thumbs compress over the lower half of the sternum, avoiding the xiphoid process, while the fingers squeeze the thorax. Supporting Literature and Suggested Readings: Neonatal Resuscitation Textbook, 5th Ed. 2005 Version 1, 4/11/2008 15