funeral claim form Form to be completed by beneficiary or policy
advertisement

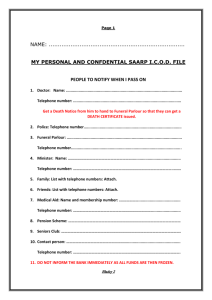
funeral claim form Form to be completed by beneficiary or policy owner All claim documentation to be certified by commissioner of oaths POLICY NUMBER: A. BENEFICIARY DETAILS: Surname: Full Names: Identity Number / Passport Number: Telephone Number: ( ) Postal Address: Postal Code: Please Indicate the relationship to the Deceased: (I.E. The Deceased was my:) Father in Mother in Brother / Spouse Father Mother Law Law Sister Child Other If other please specify: B. LIFE ASSURED (DECEASED) DETAILS: Surname: Full Names: Identity Number / Passport Number: Physical Address: Postal Code: Cause of Death: Natural Causes Accident Suicide If Deceased was a child, please provide the name of the Educational Institution (if applicable): Should the child be a full time student and 21 years or older, please attach proof from the Educational Institution. C. MEDICAL PRACTITIONERS DETAILS: (Please Provide the Details of the Doctor and Hospital who treated the Deceased) Telephone Name of Hospital/ ( Number: Doctor ) D. FUNERAL PARLOUR DETAILS (Where The Deceased was / will be Buried): Name of Funeral Parlour (UNDERTAKER): Address details: Telephone Number: Name of Person who confirmed body of Deceased: ( ) funeral claim form continued (Page 2) E. BANKING DETAILS: (Please provide the details of the Account Holder-(If benefits should be paid directly into the Parlour’s Account) – Please provide Funeral Parlour’s banking details. Bank Name: Branch Name: Branch Code: Account Name: Account Number: Type Of Account: (Please Tick Box) Cheque Savings Transmission DECLARATION I,____________________________________________________(full names and surname), hereby as Legal Owner / Beneficiary of Policy Number _________________ authorise Rentmeester Assurance Limited / Channel Life Limited to deposit the benefits under the said policy into the stated bank account by Electronic Transfer / Cheque particulars of which are mentioned above. I hereby indemnify Rentmeester Assurance Limited/ Channel Life Limited against any responsibility or liability resulting from erroneously depositing the said benefits into any other bank account owing to the incorrectness of the bank details provided above. In my capacity as ____________________________ to the above mentioned deceased as well as the claimant on the above mentioned policy, i hereby authorise any hospital / doctor to provide to Rentmeester Assurance Limited the information requested in order to finalise the claim against the said policy. I further declare that all information given above is true and correct. I acknowledge and agree acceptance of this statement and the supporting documentation will not constitute or be considered as an admission by the company that any assurance on the life assured was in fact in force, nor waive the Company’s right or defenses. I further agree that no other benefits / costs / fees are payable in terms of this policy. ___________________________ Date ________________________________ BENEFICIARY (Signature / Thumbprint) PLEASE ENSURE THAT THE FOLLOWING CERTIFIED DOCUMENTS ARE ATTACHED:Certified copy of Death Certificate Certified copy of Main Member’s Identity Document Certified copy of Deceased Identity Document Certified copy of Beneficiary’s Identity Document (In case of third party payments, a certified ID copy of the third party is required) Copy of Invoice / Quote from Funeral Parlour, responsible for the Funeral Copy of Bank Statement (Indicating account holder’s details and account number / cancelled cheque) Police Report (If Death was unnatural) If the Surname of the Spouse is different, attach any of the following:Copy of Marriage Certificate / Confirmation of Customary Union issued by a Magistrate / Lobola Letter / Letter from Tribal Chief If the Surname of the Children is different, attach any of the following:Copy of Registration / Birth Certificate reflecting Parent Details / Baptismal Certificate reflecting Parents Details / Adoption Papers Other