request for ancestral documents
advertisement

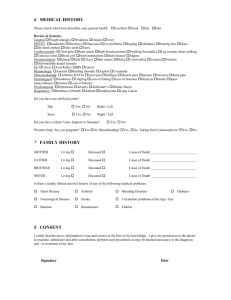
REQUEST FOR ANCESTRAL DOCUMENTS Please complete the following information as thoroughly as possible. Name of Deceased:____________________________________________ Date of Birth: _________________Date of Death:_____________________ Relationship to Deceased Member:________________________________ Branch Number:_______________________________________________ Contact:_____________________________________________________ Address:_____________________________________________________ _____________________________________________________ Home Phone:______________________Cell Phone:___________________ Email:_______________________________________________________ I would like to have my family story appear in The ZARJA, The Path Taken: ☐ Yes ☐ No Please send the form along with your check in the amount of $25.00 to: Slovenian Women’s Union of America 431 N. Chicago Street Joliet, IL 60432 For questions regarding completion of the form, or any other questions you may have regarding your request, please contact: Mary Lou Voelk Email: ottolou@gulftel.com Phone: 715.372.8578 or 251.968.4364