HRR m01b Facility Employee Handbook Part One **Refer to Employee Handbook Part 2 –which provides specifics needed for the facility you will be assigned to. As an employee you are responsible for reviewing this handbook on a regular basis to ensure understanding of and adherence to company guidelines, policies and procedures. You are also responsible for adding any memos you receive in your staff mailbox to this handbook. Please check the binder or bulletin board in staff area monthly to view any updates to this handbook or related policies. It is your responsibility to consult with human resources if you do not understand or are not in agreement with any of the statements, policies or procedures provided to you through this handbook or in subsequent memos, bulletins or updates. AdvoCare Health Services has a ratified collective agreement with the union under which we are organized for most sites. If you are assigned to a facility which is not certified, please note staff will be managed according to the same guidelines as those who are certified. Where certified, please refer to your union collective agreement and maintain awareness of contents of union bulletin boards and contact your representative if any items need clarification. Disclaimer: All parts of this Employee Handbook are supplementary to the relevant provincial legislation. In the event of a conflict, the legislation will prevail. D:\533561087.doc Approved by: PG Released by: NS Release Date: 15/07/2011 Page 2 of 64 TABLE OF CONTENTS ................................................................................................................................................. 1 ADVOCARE MISSION & VISION STATEMENT .......................................................................................... 5 1.1 1.2 1.3 2 WELCOME ........................................................................................................................................................... 6 3 ORGANIZATIONAL CHART ........................................................................................................................ 7 4 YOUR ROLE WITH ADVOCARE HEALTH SERVICES ............................................................................. 8 4.1 4.2 4.3 4.4 5.1 5.2 6 7 AFTER HOUR MAILBOX DROP BOX AND ACCESS TO DOCUMENTS................................................................ 11 TEAM COMMUNICATION .............................................................................................................................. 11 EMPLOYEE DEVELOPMENT........................................................................................................................ 12 8.1 9 ADVOCARE CORPORATE OFFICE ADDRESS .................................................................................................. 10 FACILITY TO WHICH YOU ARE ASSIGNED.................................................................................................... 10 ACCESS CODES ............................................................................................................................................ 10 POLICY CHANGES/UPDATES & TEAM COMMUNICATION ................................................................ 11 7.1 7.2 8 PARTNERSHIPS/COMMUNICATION WITH FACILITY OPERATORS ..................................................................... 8 FACILITY AND LICENSING REQUIREMENTS .................................................................................................... 8 WORKING TOGETHER AS A COMMUNITY ....................................................................................................... 8 STAFFING STRUCTURE ................................................................................................................................... 8 ROLE & RESPONSIBILITY ............................................................................................................................... 9 QUALITY IMPROVEMENT PLAN FRAMEWORK .............................................................................................. 10 ADVOCARE OFFICE INFORMATION ......................................................................................................... 10 6.1 6.2 6.4 OPPORTUNITIES FOR CONTINUING EDUCATION ............................................................................................ 12 ETHICAL STANDARDS/CONFLICT OF INTEREST ................................................................................. 12 9.1 ETHICAL STANDARDS/CONFLICT OF INTEREST ............................................................................................ 12 10 EQUAL EMPLOYMENT OPPORTUNITY.................................................................................................... 12 11 HARASSMENT .................................................................................................................................................. 12 11.1 11.2 11.3 11.4 12 GENERAL HARASSMENT .............................................................................................................................. 13 SEXUAL HARASSMENT ................................................................................................................................. 13 WHO THIS POLICY APPLIES TO .................................................................................................................... 13 DEALING WITH COMPLAINTS REGARDING HARASSMENT AND RELATED MATTERS ...................................... 13 RESPECT IN THE WORKPLACE .................................................................................................................. 14 12.1 12.2 ABUSE .......................................................................................................................................................... 14 CHALLENGE OR COMPLAINT RESOLUTION PROCEDURE ............................................................................... 14 13 ASSIGNMENT MODEL .................................................................................................................................... 14 14 INTRODUCTIONS AND RESIDENT IDENTIFICATION .......................................................................... 14 14.1 MEMO REGARDING RESIDENT DAY, FAMILY DAY, EVENING AND NIGHT STORIES ...................................... 15 15 REGARDING BRINGING PETS OR CHILDREN OR OTHERS TO THE WORKPLACE .................... 15 16 MEAL BREAKS ................................................................................................................................................. 15 16.1 17 D:\533561087.doc MISSION STATEMENT ..................................................................................................................................... 5 CORE VALUES ................................................................................................................................................ 5 PHILOSOPHY OF CARE .................................................................................................................................... 5 USE OF FACILITY ITEMS ON MEAL BREAKS ................................................................................................. 16 PUNCTUALITY & LEAVING ASSIGNMENTS EARLY & ATTENDANCE............................................ 16 Approved by: PG Released by: NS Release Date: 03/29/2012 Page 3 of 64 18 PAYROLL/SCHEDULING ............................................................................................................................... 16 18.1 18.2 18.3 18.4 18.5 18.6 19 SCHEDULING .................................................................................................................................................... 19 19.1 19.2 19.3 19.4 19.5 19.6 19.7 19.8 19.9 20 20.5 20.6 20.7 20.8 20.9 20.10 UNACCEPTABLE JOB PERFORMANCE & DISCIPLINARY ACTION ................................................................... 20 UNACCEPTABLE BEHAVIOR (REFER AS WELL TO – CODE OF PROFESSIONAL CONDUCT HRC F06A)............ 20 STAFF ARE EXPECTED TO BE: ....................................................................................................................... 21 PROFESSIONAL IMAGE (SEE ALSO POLICY HRC 03 DRESS CODE) AND, CODE OF PROFESSIONAL CONDUCT WHICH IS SIGNED DURING EMPLOYEE INFORMATION SESSION) .................................................................... 22 ABSENTEEISM, TARDINESS AND SICK TIME .................................................................................................. 23 PHYSICIANS DOCUMENT AND ABSENTEEISM ............................................................................................... 23 ANNUAL FLU VACCINATION ........................................................................................................................ 23 GIFT POLICY ................................................................................................................................................. 23 SMOKING...................................................................................................................................................... 24 PROTECTION OF COMPANY, CONTRACT PARTNER, EMPLOYEE & RESIDENT PROPERTY AND LIVING AND WORKING AREAS. ........................................................................................................................................ 24 EVALUATION PERIOD & PREFORMANCE REVIEWS ........................................................................... 25 21.1 21.2 22 AVAILABILITY & OUTSIDE EMPLOYMENT ................................................................................................... 19 VACATIONS & STATUTORY HOLIDAYS ........................................................................................................ 19 LEAVE OF ABSENCE ..................................................................................................................................... 19 BEREAVEMENT LEAVE ................................................................................................................................. 19 RETURNING CALLS TO SCHEDULING ............................................................................................................ 19 CASUAL REQUIREMENTS .............................................................................................................................. 20 WORKING AT NIGHT .................................................................................................................................... 20 ACCOMMODATING NEEDS OF STAFF ............................................................................................................ 20 SHIFT SWAPS ................................................................................................................................................. 20 WARNING, SUSPENSION AND DISCHARGE ............................................................................................. 20 20.1 20.2 20.3 20.4 21 EARNINGS & PAYROLL DEDUCTIONS ........................................................................................................... 16 BENEFIT PLAN ENTITLEMENT FOR CASUAL STAFF....................................................................................... 18 VACATION PAY ............................................................................................................................................ 18 GARNISHMENT OF WAGES ........................................................................................................................... 18 BIOMETRIC TIME CLOCK ............................................................................................................................. 18 RECORD OF EMPLOYMENT (ROE) ................................................................................................................ 18 ACCOMPLISHMENT REVIEWS ....................................................................................................................... 25 TERMINATIONS ............................................................................................................................................ 25 TELEPHONE USE AND CALL BELL SYSTEMS ........................................................................................ 25 22.1 PORTABLE WORK PHONES/CALL BELL SYSTEM/DOOR ALARMS ................................................................. 25 22.2 USE OF PERSONAL PHONES OR OTHER COMMUNICATION DEVICES WHILE AT WORK ..................................... 26 22.2A COMPUTERS ..................................................................................................................................................... 26 23 SOLICITATIONS & DISTRIBUTIONS .......................................................................................................... 26 24 ADVOCARE PRIVACY POLICY .................................................................................................................... 27 25 CONFIDENTIALITY GUIDELINES .............................................................................................................. 27 26 “PRIDE IN CARING” OUR TRADEMARK LOGO! .................................................................................... 27 27 RISK MANAGEMENT & QUALITY ASSURANCE..................................................................................... 27 27.1 27.2 27.3 27.4 D:\533561087.doc EMERGENCY READINESS PLAN .................................................................................................................... 27 CQI (CONTINUOUS QUALITY IMPROVEMENT) & RISK MANAGEMENT......................................................... 28 RIGHT TO REFUSE UNSAFE WORK AND, SAFETY CONSIDERATIONS FOR THOSE WORKING ALONE OR AT NIGHT. .......................................................................................................................................................... 28 ROLES AND RESPONSIBILITIES ..................................................................................................................... 28 Approved by: PG Released by: NS Release Date: 03/29/2012 Page 4 of 64 27.5 28 UNIVERSAL FALL PRECAUTIONS .............................................................................................................. 31 29 KEEPING SAFE FROM FALLS- 3 EASY QUESTIONS............................................................................... 32 30 WORKPLACE HAZARDOUS MATERIAL SYSTEM (WHMIS) ............................................................... 33 30.1 30.2 30.3 30.4 30.5 30.6 30.7 31 PURPOSE OF WHMIS ................................................................................................................................... 33 MSDS .......................................................................................................................................................... 34 THE NINE CATEGORIES OF INFORMATION OF MSDS .................................................................................... 34 SUPPLIER RESPONSIBILITIES ........................................................................................................................ 35 EMPLOYER RESPONSIBILITIES ...................................................................................................................... 35 WORKER RESPONSIBILITIES ......................................................................................................................... 35 CLASSIFICATION OF HAZARDOUS MATERIAL ............................................................................................... 35 SYMBOLS & LABEL WHMIS LOGO & SYMBOLS ................................................................................... 36 31.1 31.2 D:\533561087.doc INFECTION CONTROL PRACTICES ................................................................................................................. 29 WHMIS LOGO ............................................................................................................................................. 36 WHMIS HAZARAD SYMBOLS ............................................................................................................... 36 32 GENERAL DOCUMENTATION GUIDE ....................................................................................................... 37 33 MEAL PLANNING, DELIVERY & SUPPORT OF LIBERALIZED NUTRITION .................................. 38 34 OBSERVATION MEMO FOR PROGRAM AREA ........................................................................................ 41 35 POLICY: ABUSE FREE ENVIRONMENT .................................................................................................... 42 36 POLICY: NON RESTRAINT/RESTRAINT CONSIDERATIONS .............................................................. 45 37 POLICY: PREVENTING VIOLENCE IN THE WORKPLACE .................................................................. 49 38 RESIDENTS’ BILL OF RIGHTS ..................................................................................................................... 56 39 POLICY: APPROVED ABBREVIATIONS ..................................................................................................... 58 Approved by: PG Released by: NS Release Date: 03/29/2012 Page 5 of 64 1 AdvoCare MISSION & Core Values 1.1 Mission Statement AdvoCare Health Services takes “PRIDE IN CARING” for the residents we support, our partners, employees and the community we serve. 1.2 Core Values 1.3 We honour residents’ choice and right to self-determination through the provision of client focused care, support services, leisure and recreation programs We support Residents to pursue interests and participate in social and recreational activities. These activities serve to enhance ones dignity and support independence while encouraging continued involvement within our community We strive to maintain a culture of safety in all that we do, while honouring Residents’ autonomy We support work environments that attract and retain staff members who share our commitment for care excellence and for a respectful, dynamic work places We support lifelong learning in all disciplines We take pride in the development and sharing of leading health care practices We maintain an awareness of ethical dilemmas and resolutions as they relate to emerging social, cultural and clinical considerations We are committed to promoting and maintaining optimal health and wellness for our residents and employees We celebrate diversity We realize significant synergies as a result of positive collaboration within our departments, and with our communities and partnerships We recognize the intrinsic values in balancing goals with strategic growth AdvoCare is recognized for its ability to integrate the values, policies and processes shared by its contract partners, health authorities and accreditation stakeholders Philosophy of care Our philosophy of care is one which is client/resident/tenant focused, celebrating the unique history, interest and preferred lifestyle of each resident and, the needs of our contract partners. We strive to create family units with one to one care giving by staff who know the clients well and whom the clients recognize as part of their “family” of caregivers. For every task The performance standard is “do it right the first time.” D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 6 of 64 2 WELCOME You have been selected to join the AdvoCare Health Services team (hereafter to refer to as the company) because we believe that you are a caring and effective person. We have always emphasized that outstanding people are the key to our success. Through the efforts of our staff since 1991, we have become a leader in the province for support to clients and their families. This Handbook has been developed to answer some of the questions you may have about our company, our philosophies, policies and expectations. Please keep this handbook in a secure location for your future reference and to add updated policies to. Thank you for taking this first step in knowing your company. A rewarding and challenging experience awaits you. May you experience both personal and professional satisfaction as a member of our team. Please note that most of our worksites are unionized and where they are not, AdvoCare strives to provide the same benefits as other employees receive. In unionized sites, AdvoCare Health Services has made available in the staff area, a union bulletin board where you can access regular updates from the Union. Contact names and numbers of your representatives are posted there as well. Please review on regular basis and contact union reps. as required. All staff is reminded of the availability of support agencies such as the Labor Board should one want to consult with them regarding worker rights etc, Please note that we are often asked to provide care services through a contract agreement with our companies. In such instances, you will be adhering to AdvoCare’s policies and agreements of hire but may also be oriented to the policies and procedures of our contract partners. We make every attempt to understand and adhere to the philosophy of the care home (facility) in which we may be assigned. Please don’t hesitate to ask for any support or clarification you may need at any time. Welcome! John T. Manton Presiden D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 7 of 64 3 D:\533561087.doc ORGANIZATIONAL CHART Approved by: PG Released by: NS Release Date: 03/29/2012 Page 8 of 64 4 YOUR ROLE WITH ADVOCARE HEALTH SERVICES 4.1 Partnerships/Communication with Facility Operators Systems, policies and procedures, have been created and nurtured over the years and are a result of vast and diverse experience and resources. Systems are in place to ensure consistent, quality care and are reviewed and adapted in anticipation of or response to changes in health care and licensing requirements. Our goal is to promote, maintain and advance a ‘total quality culture’ in which the collective organization continually examines ways to improve upon its service delivery. You are required to review and maintain awareness of internal procedures and uphold the principles of their culture of safety which includes a commitment to resident safety at all times. Please contribute suggestions during your staff reviews, on observation memos, responding to staff surveys as well as relaying concerns or suggestions to your Program Manager or, a company representative. For emerging or urgent resident care or safety concerns, report to the nurse in charge at the time. 4.2 Facility and Licensing Requirements AdvoCare Health Services, as a contracting agency and subsequently you, as our employee, work within AdvoCare policies as well as the guidelines and policies established by our contract partner(s), the health authorities and licensing requirements which includes audits of staff competencies reflected in your employee agreement which are conditions of hire and must be maintained by the employee. This includes keeping the employer aware of any emerging factors which may restrict your ability to work in compliance with governing rules such as criminal record clearances, TB status etc. The Administrator/DOC or nurse representative of the operator maintains authority and responsibility for ensuring care and support services (housekeeping/laundry and dietary) provided is in accordance their corporate mandate as well as licensing requirements and best practices. You may receive direction which may include redirection and/or a reminder of what policy guidelines are from one of the above or, a team leader assigned by AdvoCare Health Services. As needed, the team leader may supply additional guidance to the employee while on assignment. The team leader or a representative from the facility will relay outstanding issues to the Program Manager or Program Coordinator. AdvoCare will assume responsibility for subsequent investigation, coaching etc. 4.3 Working Together As a Community There will be ongoing collaboration with the Administrator (aka Site Leader) and clinical/leadership team of the facility regarding how to best meet the needs of the resident population. AdvoCare remains mindful that ultimately the Operator/Clinical Advisor/Clinical Team of the contract partner holds ultimate responsibility for the license of the home and defers accordingly. The focus of the care will be centered on the resident – their needs, preferences, and their day. There will be ongoing collaboration with multiple community partners who may include representatives from the health authority, licensing officers, the primary physician of the facility, trustees’ office, volunteer groups, resident council, AdvoCare employees, facility employees etc. 4.4 Staffing Structure In homes each department is staffed by AdvoCare or only some departments though all staff works as a team. Non-AdvoCare management or nursing personnel retain the right and responsibility, per licensing; to remove any employee (ours or their own) from work duties should they feel an employee’s actions may be harmful to the resident(s) or the reputation of the facility. In such D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 9 of 64 instances, the employee would be asked to leave the unit and proceed to an agreed upon location (depending on situation this may be the staff area or their own home). If an AdvoCare representative is available at the time, they would be contacted to meet with the person issuing the concern as well as the AdvoCare employee. If not available, the facility staff will contact an AdvoCare Manager who will then respond. All parties involved will be required to document what events took place and such documentation will be forwarded to the HR representative at AdvoCare. Progressive disciplinary action, should it be indicated, will be addressed by the HR dept. The union will be advised, in writing, of such events and staff who wish, may have a union steward present during any disciplinary meetings. Outcomes and resolutions will be relayed, in writing, to the facility administrator and agreement sought to minimize reoccurrence. Subsequent reporting to licensing are generally at the discretion of the operator of the home. AdvoCare Health Services retains the right to reassign staff to an alternate area, facility or home within a reasonable geographical distance as required. Should staff be required to travel from one location to another during their shift, travel times and costs will be compensated as per the Collective Agreement. Staff may be called on to provide care in primary or related roles however, will not be paid less for their work than that of the primary role. Staff may be reassigned to other roles or aspect of roles as required to meet operational demands. Staff is advised that reassignment within the home or program area is permitted at the direction of an AdvoCare representative and/or nurse for that home or area. Refusal to be reassigned is a serious infraction which triggers disciplinary action. 5 CONTINUOUS QUALITY IMPROVEMENT 5.1 Role & Responsibility CQI (continuous quality improvement) is a foundation of our company’s operations and employees have a role in this process. Your observations about any changes in the resident’s status are very important. Be sure to report and document such observations in the communication binder as they are noted. Staff is to report noteworthy changes of a resident’s status and any urgent matters to the nurse in charge in accordance with our profession’s duty to report. Update Resident Days (may be referred to as “My Day, My Story” or similar variation) so they reflect the residents’ current needs and preferences. As well, record any concerns you may note regarding equipment or the environment in the maintenance binder. Where it appears a matter should be reviewed by the OH&S committee and/or an AdvoCare Manager, also record on the Observation Memos provided and place in the AdvoCare office mailbox. You are a valuable member of the team and where possible, will be included in client care conferences and other planning session. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 10 of 64 5.2 Quality Improvement Plan Framework Establish Values, Vision Goals & Objectives Identify Processes & Indicators to be monitored Identify Clients & Requirements Monitor to Identify Improvement Opportunities Make Improvements CQI Project Phase Establish Team, Define Opportunity, Analyze, Select Solutions, Evaluate Results, Standardize, Strategize Future Plans 6 ADVOCARE OFFICE INFORMATION 6.1 AdvoCare Corporate Office Address 1450 St. Paul Street Kelowna BC, V1Y 2E6 General Inquires Telephone: 250-861-3446 Toll Free: 1– 866-861-3446 Fax: 250-861-3112 Analyze Results Scheduling Office Telephone: 250-861-3399 Toll Free: 1-877-959-5444 **In case of an emergency which results in no phone lines, you can contact our office on our cell phone number at 250-863-3499 or 250-575-4677 6.2 Facility to Which You Are Assigned Refer to employee handbook part 2 for address, contact and other information you will require for this worksite. 6.4 Access Codes (Please ensure you record for use while on assignment) **Facilitator @ new employee session to fill in blanks @ NES session (as they change too frequently for generic entry though, most homes utilize “the year followed by the # sign or, the street address ie: 1450). Main entrance: _________ Special Care: __________ Elevator:________ Other:________ D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 11 of 64 Days From To Office Hours (payroll / HR) Monday to Friday 0830 1630 Scheduling Hours Monday to Friday Direct Line 250-861-3399 or Toll Free 1-877-959-5444 (to be used during specified scheduling hrs only) 0530 1800 All Sick Calls 7 days a week 250-861-3399 or Toll Free 1-877-959-5445, call a minimum of 3 hours prior if unable to attend a shift 0530 2330 Payday Every 2nd Tuesday by automatic bank deposit ***Please note that in addition to our company’s mailbox @ the worksite, our main office has a drop box at the main front door for after hour's use. 7 POLICY CHANGES/UPDATES & TEAM COMMUNICATION 7.1 After Hour Mailbox Drop Box and access to documents Policies are reviewed as we respond to changes in best practices, licensing and contract requirements. Updates will be relayed via postings in staff area or, copies may be left in employee mailboxes which staff are encouraged to check on a regular basis. 7.2 Team Communication It is prohibited for staff to speak a language other than English while on assignment. To do so excludes coworker and residents. The only exception is when staff who are able to communicate in the language of the resident they are conversing with. Staff is to ensure communication, both oral and written, is polite, professional and courteous at all times while on assignment and within the care areas. Staff is prohibited from voicing or writing derogatory, inflammatory or accusatory comments. Should staff have a concern which they feel needs to be addressed by a manager, please record your concern in an objective, concise manner on the observation memos provided. Staff is to redirect concerns a resident or family member may have to the nurse in charge, DOC or Administrator or Program Manager and, not directly engage in discussions of a negative manner regarding coworkers or others. Staff is also encouraged to discuss concerns with a union representative (away from care areas). Each employee has the responsibility to read the information posted or left in your mailbox, on the staffs’ general information bulletin board, union communication board and Occupational Health & Safety bulletin board. It is a job requirement that employees read the communication book, 24 hour report, resident days (aka My Days) and any other avenues of communication provided, to ensure aware of residents and team needs and responsibilities at the start of every shift. Knowing the residents is a crucial step to ensuring quality care and, keeping you, residents and co-workers safe. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 12 of 64 8 EMPLOYEE DEVELOPMENT 8.1 Opportunities for Continuing Education There are numerous opportunities for all staff to further their knowledge of community health and client care by providing: Staff meetings and care conferences Mandatory and optional training programs Reference materials with sign out privileges Employees’ files will be updated whenever you attend training, which has been coordinated by AdvoCare Health Services. Please relay any other training certificates you may acquire to our office to ensure your employee file is maintained. Please note it is a condition of hire for nurses, care aides, & recreation managers and aides, to provide or commit to participating in training for RAI certification, within 4 weeks of employment. 9 ETHICAL STANDARDS/CONFLICT OF INTEREST 9.1 Ethical Standards/Conflict of Interest We have built our business with a reputation for conducting its business activities with integrity, fairness, and in accordance with the highest ethical standards. As an employee you enjoy the benefits of that reputation and are obligated to uphold it in every business activity. Staff is to represent the company and facility in a positive manner. Staff is not to discuss conflicts while in the presence of a resident or visitor to the facility, as we would not want to cause undue distress. Staff is not to engage in dialogue or activities which undermine the direction or authority of the nurse, Program Manager or Physician or Administrator of the home. Staff is to utilize approved avenues to report or discuss concerns. Staff is prohibited from doing any work, either in return for pay or not, which is not assigned by AdvoCare Health Services while on assignment or, with clients you may be assigned to unless prior, approval is granted by a company manager. 10 EQUAL EMPLOYMENT OPPORTUNITY AdvoCare Health Services takes affirmative action to ensure equal employment opportunity for current and prospective employees. We recruit and retain employees on the basis of personal competence and potential for advancement without regard for race, color, religion, gender, sexual orientation, national origin, age, or physical impairments. Our equal employment opportunity philosophy applies to all aspects of employment, which includes recruiting, hiring, training, transfers, promotion, job benefits, educational assistance, and social and recreational activities. 11 HARASSMENT Company employees, contractors, students, volunteers and visitors are entitled to be treated with dignity, and to be free from harassment based on the protected grounds described in the applicable legislation in our Province. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 13 of 64 11.1 General Harassment Is any unwelcome behavior, conduct or communication directed at an individual that is offensive to that individual and is based on any of the protected grounds. It can be persistent or sporadic and creates an intimidating, offensive or embarrassing work environment for the individual. 11.2 Sexual Harassment Is any offensive sexual comment, gesture, physical contact or demand for sexual favors, real or perceived, that is deliberate and unwelcome, or that should be known to be unwelcome. It can also create an intimidating, offensive or embarrassing work environment. Among the behaviors that may constitute harassment are: differential treatment of employees or co-workers based on race, gender, ethnicity, etc.; racist or sexist humor, unwanted physical contact; pornographic or other offensive materials displayed in the workplace; a promise of better treatment in return for sexual favors; or Implied or expressed threats for refusal of a sexual request. 11.3 Who This Policy Applies To This policy applies to all persons and all activities on company premises, as well as all companysponsored conferences, training seminars, travel, sales calls and social events. If you feel you are being subjected to harassment, you should: make your objection clearly known to the offender and ask him or her to stop; prepare and maintain a written record of the dates, times, nature of the behavior and any witnesses; and report the behavior to your supervisor; Refer to Collective Agreement. 11.4 Dealing with Complaints regarding Harassment and related matters We will deal with the complaint as with any other complaint. The identity of the parties and the details of the complaint will be kept as confidential as possible. A complainant is free to pursue his or her complaint under the appropriate human rights law by contacting the Human Rights Commission and/or their union representative. In the event of a complaint of general or sexual harassment, we will follow this procedure to deal with the complaint: 1. If the complainant has confronted his or her harasser and has not been able to resolve the situation, a report should be made to the complainant’s Supervisor or to the Director if the Supervisor is the alleged harasser. The Supervisor and Director will attempt to resolve the problem. The staff has the option and right to consult with a union representative if they feel the matter is not being addressed or resolved in a timely or sufficient manner by the company. 2. The complainant should keep a detailed record of the event or events, including person(s) involved, place, date, time and witnesses. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 14 of 64 12 RESPECT IN THE WORKPLACE 12.1 Abuse AdvoCare Health Services views abuse very seriously, whether verbal or physical, of a fellow employee, resident, family member, or visitor. Understanding of and adherence to the accompanying employee agreement is mandatory; staff is to remain cognizant of the agreement on maintaining a care and work environment which is free of neglect and abuse. Employees, who encounter challenges with residents, staff, family members, or visitors, are to avoid confrontations and are to report such challenges immediately to the nurse or supervisor for assistance. Actions, such as fighting, arguing, participating in conversations which are of a negative nature, gossiping, spreading rumors, writing anonymous letters of complaint, dialogue which may instill anxiety, fear or uncertainty in residents, coworkers or visitors to the home, use of derogatory or abusive language, in written or oral form, abuse, or neglect in any form is strictly prohibited and will be cause for disciplinary action up to and including dismissal. 12.2 Challenge or Complaint Resolution Procedure Our mandate is to treat all employees in a fair and consistent manner and address emerging concerns in a thoughtful and timely manner. You are encouraged to make management aware of any concerns or recommendations dealing with workplace safety, health standards, working conditions, performance appraisals, discipline and general practices. Staff is not to complain about coworkers, the company or the facility to which they are assigned while on assignment except in situations where reporting is needed in keeping with our duty to report as health care workers and advocates of those we support. In such situations, staff is to ensure the report is objective and evidence based (only). Staff is to not unfairly attempt to negate the efforts or reputations of fellow employees of AdvoCare or those hired by the facility or on contract for services in the facility to a client, their family or advocates. Staff found to be actively, intentionally or otherwise, undermining the efforts of the company or teams may be removed from such assignments if the matter is not resolved. 1. Contact an AdvoCare representative (refer to Who to Contact List), if you have concerns about your schedules or work conditions. You are to document your concern(s) and provide to an AdvoCare representative. 13 ASSIGNMENT MODEL Each time you give service, think about the resident (or tenant) as someone in your own family whom you care about dearly. In this way, the resident will receive the same degree of dignity and respect that you would give your own loved ones. We support a social model of care which recognizes and supports the physical, emotional, social, intellectual and spiritual needs of the resident. Master all the details of your resident’s care needs within your level of competency. 14 INTRODUCTIONS and RESIDENT IDENTIFICATION When you meet a resident, tenant or their visitor, offer your first name and wear your name tag. Name tags are a very basic courtesy to others especially residents and their family members who deserve to know who is caring for them yet may have difficulty remembering names. Noncompliance is not tolerated. Staff who require a new nametag are to provide written note of same immediately & leave D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 15 of 64 in the AdvoCare mailbox or office. A temporary tag will be provided to staff while the new one arrives and for those who arrive to work and have forgotten their primary name tag @ home. Staff is not to engage in conversations which may instill fear or anxiety in a resident or their family member. This includes discussing other employees, residents, family members or others in a negative manner within the program area. Staff is not to disclose personal aspects of their own lives which may result in the resident or their family member worrying about you and your personal concerns. Staff to ensure correct resident identifiers in place – do not guess who one may be. Guidelines for safe practice include use of TWO resident identifiers which may include: 14.1 Ask person what their name is – first and last name, (do not say “are you Mary Smith?”) Verify ID by referring to resident photo on treatment or medication record or in Family Binder, Ask coworker to verify identity, DO NOT rely on labels on clothing as person may be wearing someone else’s clothing. Memo regarding Resident Day, Family Day, Evening and Night Stories See part 2 of handbook for samples of My Day/ Resident Day and Family Stories. A reminder that ALL staff, including Recreation staff are to routinely update the Resident Days 15 REGARDING BRINGING PETS OR CHILDREN or OTHERS TO THE WORKPLACE Staff is prohibited from bringing pets to the workplace without direct approval from the recreation manager of the home. Care homes have policies in place reflecting guidelines for “Pet Therapy” and staff must be in compliance with all aspects of that policy. Should permission be granted, staff must ensure that the pet does not limit the ability to fulfill their duties that shift. AdvoCare will hold no responsibility for any related injury or mishaps that may occur. Staff is reminded that in relation to confidentiality, Risk Management specifically safety of residents and children or others and Quality Control, no children, spouses or friends of the employee are permitted in the workplace unless authorized as above. 16 MEAL BREAKS Your lunch and beverages are your responsibility. Timing of meal and coffee breaks will be coordinated within each program area upon consideration of resident and team needs allow. Resident meal times are a priority and staff is to arrange their own breaks around these peak needs times and, in consideration of other urgent matters which may arise. Management retains right to establish set times for staff or teams who can’t manage independently. LPNs are reminded to contact the RN/Program Manager of the facility for cardinal/urgent matters when the RN is on break. LPNs @ AdvoCare Health have full scope practice and, assume responsibility for all but cardinal issues and should contact D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 16 of 64 the RN/Program Manager only in situations where the concern appears so significant that it cannot await the 30 minute break time of the RN (who is free to leave the home during all breaks other than night shifts). Examples of such cardinal events include: Unanticipated death or significant injury to a resident under troubling circumstances such as evidence of self harm causing death, presence of unsecured medications, evidence of another causing death. Mass emergency such as fire, bomb threat etc. ** Staff is prohibited from taking/eating food or other items that are intended for residents. Doing so will result in disciplinary action up to and including dismissal as is considered a form of theft. 16.1 Use of Facility Items On Meal Breaks Items in the facility to which you are assigned are the property if the operator and use of their items (ie. coffee cups, dishes) are to be respected (put away after use, tided up, ect.). Blankets in the home are for residents only; if staff prefer to nap during approved breaks, staff are to provide their own blankets from home or use a coat. 17 PUNCTUALITY & LEAVING ASSIGNMENTS EARLY & ATTENDANCE Never leave an assignment early unless you have permission from an AdvoCare representative or, are directed to do so by the nurse in charge which may occur if he or she feels your presence is having a detrimental impact. Staff is to plan in advance in order to arrive to shift as scheduled. Staff is to refer to policy HRC 9 and the collective agreement regarding hours of work which outlines the minimum number of shifts one must maintain to be considered an active employee. 18 PAYROLL/SCHEDULING The pay period is biweekly. Your pay will cover all hours worked in the two weeks prior to payday up to and including the night shift on the Sunday midnight cut-off. Those disciplines which require a tally of the hours worked i.e.: nurses or those applying for EI benefits are to keep track of their own hours worked through the year. (This is done by retaining your payroll stubs.) Staff holds responsibility for checking their payroll stubs and if questions or concerns, to report same that pay period to the payroll department. Staff holds responsibility for recording, by exemption form, any overtime they feel they are entitled to including the rationale. Such exemptions must be authorized by the Program Manager prior to submission to payroll clerk. 18.1 Earnings & Payroll Deductions Payroll earnings and deductions are reflected on your payroll stub. Deductions required by federal law and/or the union agreements are as follows: Federal Income Tax D:\533561087.doc Canada Pension Plan (CPP) Employment Insurance Premiums (EI) Union dues (as per collective agreement). Approved by: PG Released by: NS Release Date: 03/29/2012 Page 17 of 64 D:\533561087.doc Benefit package contributions where applicable, as per collective agreement. (for those who are not covered by benefit plan elsewhere) RRSP contributions (as per collective agreement). Approved by: PG Released by: NS Release Date: 03/29/2012 Page 18 of 64 18.2 Payroll forms (by exception only to their regular schedule - will be explained by facilitator). Benefit Plan Entitlement for Casual Staff As of August 1, 2011, John Manton, Company President, has approved the benefit package to be available to casual staff members. To be eligible you must have averaged 20 hours/ week over 13 weeks of employment. To maintain your benefit plan you must continue to average 20 hours/ week. Your union is aware of and supports this action. When you qualify, Brenda Saretzky, Benefits & Payroll Manager will email you your enrollment paperwork for those who would like to participate. 18.3 Vacation Pay Is at the provincial rate, is given on each pay, or is held for your use at holiday time request and in keeping with the collective agreement. 18.4 Garnishment of Wages A garnishment is legal permission for creditors to collect part of an employee’s pay directly from the company. Although, the company does not wish to become involved in employee’s private matters, we are compelled by law to comply with the court’s order. 18.5 BioMetric Time Clock As we seek increased employment opportunities for our staff in various areas of the province, there is increased pressure to keep up with the technological changes related to this industry. This practice is common at other sites and has been approved by your union. Please note at sites where the BioMetric system is in place, you are required to confirm your start and departure time from each and every shift. The process ensures your right to privacy is not compromised. This process enables us to confirm attendance of staff on any shift and respond to queries from the operator or others in an evidence based manner. Staff is expected to be punctual for all shifts and leave only at approved times. We remind you to take your authorized breaks throughout your shift. Missing a break to then leave early is not permitted. We appreciate when there are circumstances outside one’s control in regards to prompt arrival to the workplace; however, in keeping with our contract obligations and fairness to all staff, those who display a pattern of tardiness, leave shift(s) early or are significantly absent from the shift will face discipline. In keeping with company and contractual obligations, pay is based on actual hours worked: for example, if you are scheduled to work a 7.5 hour shift and show up for work 25 minutes late, you will only be paid for time worked. 18.6 Record of Employment (ROE) Upon receipt of a request for an ROE due to leave of absence, resignation, dismissal, etc. Payroll prepares and submits the ROE electronically to Service Canada. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 19 of 64 If you wish a copy for your records, you should visit the My Service Canada Account page on the Web. From My Service Canada Account, you can view and/or print copies of ROEs. To access My Service Canada Account, you should visit www.servicecanada.gc.ca/eng/online/mysca.shtml. 19 SCHEDULING Scheduling is done in accordance with the collective agreement. While every attempt is made to provide regular work opportunities and schedules, assignments are subject to change based on operational needs of the company and contract partners. 19.1 Availability & Outside Employment Staff is recruited at times when we are expecting growth or are experiencing challenges staffing existing lines. To minimize the need for recruitment, all staff is to be available for some weekends or part thereof. 19.2 Vacations & Statutory Holidays Refer to guidelines in your collective agreement. 19.3 Leave of Absence AdvoCare Health Services grants time off in keeping with the terms of the Collective Agreement, however operational requirements will be considered in the decision to approve or decline such requests. A written request for a leave of absence must be presented to the employee’s immediate supervisor at least two weeks before the start date of the proposed leave of absence. Failure to report to the office after the expiration of the leave of absence, without approval, will be considered a voluntary termination of employment. 19.4 Bereavement Leave Please refer to the Collective Agreement. 19.5 Returning Calls to Scheduling Employees are reminded of the importance of returning calls as soon as possible. Please check your cell phone/pager regularly for any messages and return as required. Ensure that your mailbox is cleared on a regular basis, and that your answering service/machine is turned on, so scheduling staff can leave messages for you. Ensure our office is notified of any phone or address changes. All calls to scheduling are recorded to ensure the quality of our service and for training purposes. Please note operators may have audio & video recording devices in the home as rsk management strategies. This is to re-enforce our policy on recording conversations between individuals: it is a VIOLATION of the Privacy Act, AdvoCare Health Services Policy and Procedures, and a breach of the Confidentiality Agreement which all employees have read and signed. Effective January 1, 2010, the use of cell phones and text messaging equipment was banned while driving a vehicle. It is AdvoCare’s policy to support this law; AdvoCare staff are advised they are prohibited from answering cell phones and/or text messaging equipment, while driving. If scheduling calls while you are not available, they will leave a voicemail message; staff can return the call once no longer driving. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 20 of 64 19.6 Casual Requirements Casuals are required to maintain a minimum of six (6) shifts over a twelve (12) week period, in order to maintain awareness of and familiarity with AdvoCare policies, systems and procedures and, to ensure sufficient, viable casual pool of staff. Shifts are monitored accordingly. 19.7 Working at Night We recommend that employees who depart from the worksite when it is dark or isolated, strive to do so with a coworker, to remain together untill one is in their vehicle and has secured the door. AdvoCare is prepared to pay for transportation in instances where risk cannot be otherwise managed. 19.8 Accommodating Needs of Staff AdvoCare welcomes the ability to accommodate short and long term needs of its employees. To ensure timely and proactive actions to minimize risk to yourself, fellow employees, clients and the company, we ask that staff advise the company of any need for accommodation. We assure employees that such information will be handled in the most confidential manner possible and, will incur the costs for related medical directives should they be required. 19.9 Shift Swaps AdvoCare’s policy allows a maximum of 6 shift swaps in a calendar year. However, the employer is receptive to discussion and possible exceptions, on a “without prejudice” basis in extenuating circumstances, though such consideration will include what impact this will have on fellow workers and the worksite. 20 WARNING, SUSPENSION AND DISCHARGE 20.1 Unacceptable Job Performance & Disciplinary Action Acceptance of employment with our company means acceptance of those personnel policies that apply to all staff members. By signing the Acknowledgement Form, one indicates they agree and will comply with the policies in this employee handbook. The policies are subject to revision from time to time in light of circumstances that may prevail in the future. Staff may access current policies at any time through the Program Manager or HR rep. One is also agreeing to comply with future policies or revisions as they occur unless they advise the HR department in writing of their inability or unwillingness to comply. Staff will be consulted if there are concerns they may have breached a company policy or if they are not performing adequately. Staff will review the event with the goal of identifying any challenges, seeking opportunities to correct the behavior and discussing the implications if such behavior is repeated. Staff is encouraged to contact their union representative to accompany them to any and all disciplinary meetings. 20.2 D:\533561087.doc Unacceptable Behavior (Refer as well to – Code of Professional Conduct HRC f06a) Possession of or being under the influence or after effects of alcoholic beverages, narcotics, or hallucinatory drugs on company or clients property. Approved by: PG Released by: NS Release Date: 03/29/2012 Page 21 of 64 Repeated absences from work due to indulgence in any of the above and/or other reasons which leads to above norm pattern of absenteeism. Immoral, rude, discriminatory or indecent language or conduct, texting or use of personal phones while on duty. Theft or illegal use or possession of client or company property. Failure to carry out any reasonable order by a nurse, administrator or supervisor. Falsification of application form, employment record, time sheets or any other company record. Speaking to or in the presence of resident, clients, coworkers or others and/or while in any program area in a derogatory or abusive manner which includes, negative comments about the company or coworkers or instilling fear and anxiety while on assignment or on company premises. Actions which permit or support abuse or neglect of any kind including horizontal violence as well as deviation from accepted standards of care which may put resident, coworkers, company or yourself at risk.. Failures to comply with operating guidelines such as time sheet and documentation policies. Accessing or utilizing electronic equipment during work times, such as cell phone, text devices or computer for personal use. Utilizing company or contract partners’ computers or other equipment or supplies for nonwork approved related purposes. Sleeping while on duty, failure to respond to the needs of residents, emergency procedures and/or direction from the nurse in charge or supervisor. Failure to comply with dress code. Failure to maintain confidentiality agreement. Failure to perform the work to which you are assigned or accept redirection from a manager or nurse in charge which may be indicated for resident care or safety. Failure to maintain criteria required upon hiring such as professional licensing, current vaccinations, first aide certificate, WHMIS and CPR (where applicable). Failure to maintain criminal record clearance as required under the Criminal Records Review Act (CRAA) 20.3 D:\533561087.doc Staff is expected to be: Free of any odor that may be offensive to residents or others. On time and alert when scheduled to work. Careful, conscientious, and honest in performance of duties and reporting. Approved by: PG Released by: NS Release Date: 03/29/2012 Page 22 of 64 20.4 Courteous and helpful, both when dealing with residents, visitors to the home, coworkers from AdvoCare or our partners. Professional Image (See also policy HRC 03 Dress Code) and, Code of Professional Conduct which is signed during Employee Information Session) As a company employee, you are expected to reflect a professional image at all times while in the workplace or while representing AdvoCare which includes: Wearing of company nametag unless advised otherwise, Should an employee lose or break their nametag, they will utilize a temporary nametag & notify AdvoCare that a replacement is required. D:\533561087.doc Wearing footwear in conjunction with WSBC guidelines – closed heel and toe with exception of cooks’ shoes which have open back. Being perfume, scent and odor free. Nails must be trim, clean and not of dark colors. Ensuring shoulder length hair is tied back or up, use of hairnets in kitchens and, male staff will ensure beards or mustaches are neatly trimmed. Minimal facial studs which are flesh colored are permitted. Earrings must be of a style which restricts others from pulling on them ie: small hoop or stud. Necklaces that may be pulled or caught are restricted as are rings or other jewelry which may scratch a resident or harbor bacteria. Unless restricted by the operator, care and nursing staff may wear scrubs though preference is given to those with design that may appeal to residents and reflect a non-institutional appearance. Casual dress attire may be worn by care and nursing staff though must comply with stipulations noted elsewhere in this policy. Pants may include capri’s, long dress shorts or full pants. Servers wear black cargo style pants with the bibbed aprons provided by the operators. Cooks wear the cooks’ jackets provided though may remove while working in the kitchen. Tops must have a small or short sleeve and not expose ones cleavage or midriff. Logos are strictly prohibited as is camouflage pattern. Jeans, tank tops, sleeveless tops, t-shirts, tight or suggestive clothing, stretchy material, jogging suits, leggings or hoodies are strictly prohibited. Chewing gum and the use of slang is prohibited. Approved by: PG Released by: NS Release Date: 03/29/2012 Page 23 of 64 20.5 Absenteeism, Tardiness and Sick time You are expected to attend work on time and as per your agreed schedule and, to be alert and ready to perform the duties associated with your role. Employees with urgent request for an absence from work are to call the office no less than three (3) hours prior to the start time of your shift and is the employee’s responsibility. Less time is accepted if scheduling hours restrict ability to provide same, in which case, AdvoCare accepts that staff for a day shift will notify us immediately upon rising for expected shift if at the time, one realizes they are ill. Exceptions may also be made for extenuating circumstances which may result in less notice being accepted. Non urgent requests for time off require two weeks’ notice. Employees are reminded of the expectation that they will remain fit and prepared for the work they are providing. An employee is to advise the company in a timely manner should they require support in any area including modification to the workplace or their role. The company will make reasonable accommodations where possible. Any employee who feels they should not attend work because they may pose a threat to the health of their client, residents or co-workers is to advise the scheduling or on-call representative immediately. 20.6 Physicians Document and Absenteeism A physician’s document verifying absenteeism due to illness may be required at the discretion of the company. Pattern absenteeism or tardiness will be addressed by the company in keeping with labor practices as we have the right and responsibility to ensure our workforce is in place as per client or contract requirements. Provision of a physician’s declaration that you are in suitable health including having the required vaccinations for a health care environment is a condition of hire. 20.7 Annual Flu Vaccination All employees who have not provided evidence they have received their annual flu vaccine in any given year may without pay be restricted from working during a flu outbreak (per licensing requirements). AdvoCare retains the right to ensure a reasonable percentage of their employees have been vaccinated each year to ensure our workforce is in place as per client or contract requirements and, requests verification of yearly compliance or, note from physician re personal exemption. 20.8 Gift policy Those we support may be in positions of vulnerability. Accordingly, it is a policy that as an employee you must refuse to accept any monetary or other rewards or presents from any resident or individual with which you have come into contact with as a result of your employment. In the event a resident insists you accept gifts please confer with the Program Manager or Coordinator. Breach of this rule may result in disciplinary action up to and including dismissal. In keeping with AdvoCare policy HRC 02 and, the union’s direction that staff should not set themselves apart from peers by the provision of gifts (items) or, gifts of time please note that staff are restricted from providing gifts of any kind to clients or residents nor are they to attend to the client or resident on other than approved shifts. Should an employee wish to contribute to the well being of others, we suggest one contacts the recreation manager to explore opportunities to volunteer at the home in accordance with volunteer guidelines D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 24 of 64 20.9 Smoking Smoking is not permitted on or in close proximity to client or premises, as per WSBC ruling 2008. 20.9a We want our staff to remain healthy! Sun Life Financial: If you are on AdvoCare’s extended benefits program, products to help a person quit smoking that require a prescription are covered up to a lifetime maximum of $500 for each person. This includes an Employee Assistance Program which is strictly confidential. A booklet regarding the benefits will be provided to you once you qualify. Related Websites and Links: Health Canada www.hc-sc.gc.ca/hl-vs/tobac-tabac/index_e.html Canadian Cancer Society www.cancer.ca Canadian Health Network www.canadian-health-network.ca Smokers Helpline: It’s free and anonymous; specialists can support you while you make good choices for a healthy future. 1-866-33AADAC (1-866-332-2322). BC will now cover costs related to smoking cessation programs and medication – ask your physician for more information! 20.10 Protection of Company, Contract Partner, Employee & Resident Property and Living and Working Areas. Respect and protection of company, home and resident property is everyone’s concern. If you find property missing or damaged, report it to the nurse in charge at the time. Ongoing maintenance issues are to be recorded by the staff observing them, in the maintenance binder. Should you notice small spills or, food that appears dated in fridge, take care of at the time. While each home has cleaning and maintenance staff, it is all of our responsibilities to safeguard work and living areas of the home. A reminder to ensure yellow “wet floor” signs are placed as required to alert residents, visitors and coworkers. Staff is cautioned to follow operating procedures for equipment and report deficiencies or new learning needs as required. Staff is reminded to ensure proper footwear is worn and that you are rested and fit for the work required. Staff is advised of their responsibility to exercise reasonable caution in order to utilize and safeguard equipment in the manner intended on operating guidelines. Special care and attention is to be given to call bell phones as replacement costs are over $600. Staff who damage or lose equipment will face disciplinary action including dismissal. Staff must ensure phones are not immersed or splashed by D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 25 of 64 water so special attention when washing dishes, bathing residents, bending over water etc. Phones are to be secured to lanyards (which are worn around neck) or holster with swivel clip which are attached to waistband or pocket. Operators of the home you are assigned to may have a deposit system in place for access (door) fobs. If a deposit is required, it would be returned at the completion of your employment or, transfer to another work location. Care staff is reminded to clear items from resident’s personal clothing prior to placing in laundry bags. Ensure no bulky items are discarded in toilets. Employees are encouraged not to bring personal items of value or money with them to work. In the event that you choose to do so, AdvoCare will not be responsible for items or money that go missing. 21 EVALUATION PERIOD & PREFORMANCE REVIEWS New employees are hired on a probationary period as are those who transfer to a new role. It gives you a chance to decide whether the job suits you and it allows us time to decide whether your work performance, skills and abilities meet our requirements. Please refer to collective agreement for details. 21.1 Accomplishment Reviews Accomplishment reviews are intended to be a constructive and positive experience. The Program Manager/HR rep. will provide feedback on your performance and help you understand where you stand relative to the job standards, expectations, goals and objectives. At the same time, the review provides you with an opportunity to discuss future developmental needs and career aspirations. Your first review will take place prior to the completion of your probationary period. Thereafter, performance reviews will be conducted yearly or sooner if requested. 21.2 Terminations We hope to retain good employees. Just as you are free to leave for any reason, we reserve the same right to end our relationship with you with notice, for reason not prohibited by law and, in keeping with our collective agreement. The employee is expected to give at least two weeks’ notice in writing before voluntarily terminating employment. All company items which were provided pertaining to your employment here must be returned at the time you resign or are dismissed - this includes all written materials, name tags, access fobs etc. Refer to the Collective Agreement regarding progressive discipline and terminations. 22 TELEPHONE USE and CALL BELL SYSTEMS 22.1 Portable Work Phones/Call Bell System/Door Alarms Portable work phones may be available to staff during shift times and are the property of the facility owner. All portable phones are connected to a call-bell system which you are responsible for responding to during work time. Phones are to be carried in the case and clipped onto the lanyard provided to ensure it doesn’t come into contact with water. In cases where it appears wiser to remove the phone (ie while leaning over tub of water), you may remove the phone, place in secure location but then put it back on as soon as task is complete. You are responsible to ensure coverage of their portable phone by a coworker while on breaks or while working in a restricted area (in some homes, the Spa room). Phones are to be replaced to appropriate location (usually charger @ care centre) @ end of your shift. Staff may be held responsible for inappropriate use or storage of phone. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 26 of 64 On administration, residents are oriented to the call bell system, as Employees are in their orientation. 1. Staff must answer the call promptly in a timely manner responding by re-assuring the resident in a courteous voice. Example “Hi Bob/ Helen I will be with you shortly” or if in the case of an emergency go immediately. 2. The resident will then hear it and be reassured-the telephone rings again to prompt the LTCA to go and provide assistance to bedroom number as indicated on the phone. 3. On attending the patient call, the LTCA will cancel the call by pressing the call bell-off. 4. Staff may be oriented to other style of call bell system. Staff own responsibility for prompt attention to any calls received. Staff is responsible for responding to door alarms each and every time to ensure no resident has inadvertently left the program are or building via a door to stairwell or exterior door. Staff is to alert nurse in charge immediately if unable to locate resident(s) who are to be checked on routinely throughout their shift with special attention to known wanderers. 22.2 Use of personal phones or other communication devices while at work Staff is prohibited from carrying personal cell phones, text messaging equipment, and/or any electronic devices with picture-taking capability, while on duty, with the exception of recreation staff or team leaders who may be asked to do so in order to facilitate quicker access during shift. Staff may check messages or place personal calls while on breaks away from program areas. While we appreciate that staff feel it is important to be available for scheduling department or personal calls, the significant frequency of staff using phones excessively which takes them away from their duties and, focus of attention being on the residents we care for necessitates us enforcing this rule in all worksites as does the importance of ensuring residents’ rights are not violated through use of photo or recording devices without express permission. Should you answer a company phone while on duty, please identify yourself to the caller and, if taking a message, ensure you record the information correctly and relay data to the appropriate person in a timely manner. 22.2a Computers Staff are restricted from utilizing computers provided other than for approved duties. 23 SOLICITATIONS & DISTRIBUTIONS As your employer, we respect and encourage employee participation in community activities however, employees are not to solicit others for such purpose during working time or distribute literature of any kind in work or care areas. Staff must not solicit donations from residents or ask them to purchase any items regardless of cause. Staff is not to enter into any contractual agreement with a resident/tenant in their care. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 27 of 64 24 ADVOCARE PRIVACY POLICY At AdvoCare, we recognize and adhere to provincial and federal legislation, specifically the privacy standards established by BC’s Personal Information Protection Act (PIPA), regarding confidentiality and privacy considerations in regards to client and staff data. Except for records and information that law requires us to provide, no information about you will be released unless there is a signed authorization on your file giving permission for the requesting agency or person your permission. 25 CONFIDENTIALITY GUIDELINES It is of utmost importance that all matters pertaining to residents and your assignments be kept in strictest confidence. To ensure ongoing confidentiality and privacy of the residents, please make sure you close the door to their room and/or draw the curtain(s) in their room when providing care. Ensure that conversations are held in a private location and that you use a quiet tone of voice as needed. Information you are privy to is not to be discussed with residents or their family other than in the context of the goal of our service and your role and, one is prohibited from speaking to one resident about another. Please place all internal information in the shredding bin(s) provided. DO NOT DISCARD IN GARBAGE! 26 “PRIDE IN CARING” OUR TRADEMARK Logo! It has long been known that we pride ourselves in providing residents with the finest of care and service. We ask our staff to treat others with the same respect and courtesy they would a family member. There are numerous accounts of staff “Going the Extra Mile” – a soothing massage, a flower at one’s bedside. Together, as a caring, competent and professional team, we will continue to excel and grow as health care provider of choice in our community. 27 RISK MANAGEMENT & QUALITY ASSURANCE 27.1 Emergency Readiness Plan AdvoCare Health Services has an active, comprehensive emergency readiness plan for its community care operation. Staff will be oriented to and included in ongoing emergency procedures for the home you are assigned to. Review related manuals and notices routinely. In facility care, we defer to the emergency plans and codes of the operator (owner) of the care home. Staff is to maintain familiarity with in home emergency procedures and actively participate in emergency drills. Emergency Codes include: **ensure you know these codes! Code Red – fire Code Blue- cardiac arrest Code Black - bomb threat Code Orange – mass casualties/disaster Code Green – evacuation Code Yellow – missing resident Code Brown – hazardous spill Code Grey – air shutdown D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 28 of 64 Power Outage Alert Please note that during power outages, secured doors automatically are released. Staff are to attend to such doors to ensure no residents inadvertently leave secure areas. 27.2 CQI (Continuous Quality Improvement) & Risk Management CQI and Risk Management is everyone’s responsibility. You are a key member of the team who may observe areas of service, which can be enhanced to bring the best possible care to those we serve. You are also a key person to identify and report possible risk situations so they can be avoided and minimized whenever possible. “Risk” may be from a number of sources, visitors leaving matches in the home etc. Our foremost concern is for the safety and well being of all staff and the residents. Please use good judgment and common sense in matters of safety, and observe any safety rules set out by the company and Health & Safety Standards. Work only on tasks that have been assigned to you. If you are in doubt about your assignment, or the safe way to do it, ask your supervisor. Be committed to life long learning! *Reminder: Staff is NEVER permitted to prop doors open. Any falls, incidents i.e.; needle prick, injuries, or any other incident which, while appearing insignificant at the time but may result in a health concern, must be reported immediately to the first aide attendant/nurse in charge. Staff is to obtain emergency or non-emergency medical consultation following any workplace injury. In the event of a workplace injury/disease, Advocare requires the Worksafe BC form “6A” to be completed by the employee, signed and dated, and submitted to the AdvoCare office within 48 hours of injury. A Form 6A is included near the end of this handbook and is also available at the program area in each neighborhood or cottage, and also in the staff room. Unusual or aggressive behavior from a resident is to be reported to the nurse in charge and documented. 27.3 Right to Refuse Unsafe Work and, Safety considerations for those working alone or at night. If you have reason to believe that any task or the environment is likely to endanger you or a coworker, speak to your supervisor or, the nurse in charge immediately and, record concerns on an observation memo and submit to AdvoCare office. You are encouraged to participate in the Health & Safety Committee which may be included in this and other day to day activities which may affect your work environment. Please refer to Policy RM 07 and, WSBC Regulations 3.9-3.13 regarding Rights related to Refusal of Unsafe work. Staff is to park in nearby well lit areas and we suggest doors remain locked to your vehicles. When exiting the home at night, strive to exit along with coworkers at same time. 27.4 Roles and Responsibilities You will be oriented to the shift routines, roles & responsibility for the home you will be assigned in and as they relate to your discipline (title). One must ensure adherence to the shift routines and processes of the operator. Do confer with your direct supervisor for the department you are assigned to or should you need further support or clarification. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 29 of 64 Alert to Nurses should they accept responsibility to mentor a student nurse Nurses are reminded of their roles and responsibilities as they relate to the worksite but also incumbent in one’s license or registration as a nurse at all times. Schools of nursing have responsibility for the placement, continued mentorship and supervision of students on practicum placements. It is also crucial that you, as the nurse, be aware of what tasks the student nurse may undertake and, the level of supervision the student requires. Please review the agreements and practicum guidelines from the school before delegating any tasks. Should there be any questions, please confer with your Program Manager or, the liaison from the school of nursing. Ultimately, you, as the nurse for the program area and/or, nurse in charge, carry ultimate responsibility for the care of the residents. The operator enters into the agreement to accept students from the school of nursing and ensures there is agreement in place regarding scope of practice, routine supervision of the student from the instructor and, clarification in writing regarding the scope of the student and related level of supervision required by the nurse on a weekly basis. AdvoCare nurses are cautioned not to proceed until such agreements are in place and, guidelines readily available to follow. “ 27.5 Infection Control Practices Routine Practices & Infection Control Infection control is a term that describes ways of preventing infections for residents and you. Routine Practices are followed to protect caregivers from coming in contact with blood or body fluids. These precautions apply to blood, body fluids containing blood, semen, vaginal secretions, cerebrospinal fluid, pleural fluid, peritoneal fluid, pericardial fluid and symbiotic fluid, feces, vomit, urine or drainage from open wounds. Clean up spills promptly using absorbent material first then clean more thoroughly as per facility policy. Soiled items are to be double bagged before discarding. Soiled sharps of course will be in sharp’s container only. Personnel will wear gloves when: o Performing any procedure, which could involve exposure to blood and/or body fluids ALWAYS treat as potentially infectious! o Staff has lesions or weeping dermatitis. o Cleaning surfaces or instruments that may be contaminated. o Disposing of anything that is soiled with blood or other infectious fluids. D:\533561087.doc Hand washing is the most effective way of preventing transmission of infections. Use warm soapy lather & running water. Keep your hands in good condition to prevent chapping, keep nails trimmed and clean. Wash your hands thoroughly before and after any client contact and after removing medical gloves. Adhere to stringent hand-washing practices. Remain aware of the risk for cross contamination and be mindful of the steps to avoid cross contamination. Avoid areas of facility it is unnecessary to be in, washing your hands after leaving the premises (we provide a waterless hand wash system to carry in your bag or car.) Approved by: PG Released by: NS Release Date: 03/29/2012 Page 30 of 64 D:\533561087.doc Keep soiled laundry in specific area. Use gloves when handling soiled, wet or damp fabrics. Garbage should be disposed of in proper bags to avoid leakage. Double bag when items potentially infectious. When bags are full, tie at the top and dispose of by dropping in the garbage container. Do not compress bags with your hands. Wash hands thoroughly afterwards. Wash hands thoroughly before and after food preparation. Dishes should be washed in warm soapy water. Use a cutting board to cut raw meat and clean board thoroughly after use. All surfaces touched should be cleaned after use. Pregnant caregivers are at no greater risk of HIV transmission, but should avoid direct contact with someone who is infected with CMV, Toxoplasmosis, Chicken Pox or Herpes. If unsure of your risks, please check with the office. All caregivers are required to report evidence of infectious diseases/process specific to clients and to report any personal reportable infections to the HR department or program manger. The company reserves the right and ability to restrict employees from the home if the employee appears to have an infectious process which could have an impact on coworkers or those we serve. In such instances, the employee will be reimbursed based on employment standards. (RM 02: Infection Control Practices) Approved by: PG Released by: NS Release Date: 03/29/2012 Page 31 of 64 28 Universal Fall Precautions * ALL residents are at risk for falls * EVERYONE has a role in fall prevention afe environment No bed rails unless assessed otherwise Pathways clear of clutter and tripping hazards Bed and chair brakes are “on” for safe transfers Lights are working and “on” as required ssist with mobility Mobilize at least 2x/day, as appropriate Safe and regular toileting Document and post resident’s transfer/mobility status Glasses, hearing and mobility aides within resident’s reach all risk reduction Call bell within resident’s reach Bed lowered to appropriate height Personal items within resident’s reach Proper footwear available and in use ngage resident and family Discuss risk factors and interventions with resident and family Develop Fall/Injury Prevention Plan with resident and family Remind to ask for help and wait 20 seconds before standing D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 32 of 64 29 Keeping Safe from Falls- 3 Easy Questions Keeping from falls Ask these 3 questions before leaving the resident’s room: Do you need to use the toilet? Do you have any pain or discomfort? Do you need anything before I leave? Asking these simple questions before you leave the room can: decrease the chance of a fall decrease the use of a call bell increase resident satisfaction D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 33 of 64 30 WORKPLACE HAZARDOUS MATERIAL SYSTEM (WHMIS) AdvoCare supports a working environment that is safe and healthy for every person at all times. WHMIS is a national system designed to ensure that everyone working with chemicals is properly informed and uses them according to health and safety procedures. WHMIS certification is required as a condition of hire though, the company accepts those who had it included within their curriculum. WHMIS applies to hazardous materials known as controlled products. All employees will review this handout upon hire and periodically throughout employment. Yearly reviews are conducted by the education department and all staff will be required to complete an annual quiz on this topic. WHMIS gives everyone in the workplace the right to know about the hazards of materials used in the workplace. It does this by means of: a) Warning labels on the containers of hazardous materials; b) Material safety data sheets (MSDS) to supplement the label with detailed hazards and precautionary information; and c) Worker training programs on how to use the information. d) WHMIS rules apply in every province and territory, as well as workplaces covered by federal law. 30.1 Purpose of WHMIS WHMIS is designed to give all working Canadians a uniform and appropriate quantity and quality of information about hazardous materials used in the workplace. WSBC dictates that all staff receive a WHMIS review annually and, non care or nursing staff must provide evidence they have received WHMIS certification as a condition of hire. Basically, the three goals of WHMIS are: To provide information about hazardous materials. To help identify hazards in the workplace. To ensure the consistency of information about hazardous materials in all Canadian workplaces. WHMIS is able to meet these three goals without compromising confidential business information or trade secrets. The flow of information about hazardous materials under WHMIS goes from producers, suppliers and importers to employers and from employers to workers who use those materials in the workplace. The information is contained on Labels and Material Safety Data Sheets. All hazardous materials used in the workplace will be labeled with a valid supplier or workplace label. No employee will deface or remove labels and will report defaced or missing labels to their supervisor immediately. The person receiving new products will ensure it is properly labeled and a copy of MSDS is placed in the MSDS binder. Managers are responsible to ensure receipt of a Material Safety Data Sheet (MSDS) from a supplier for every controlled product purchased. As well, they must make these sheets available to all staff upon request. MSDS shall be stored in a three ringed binder, appropriately labeled for MSDS, or on computer and shall be readily accessible to all Employees. The MSDS describes the hazard created by the product, safe handling procedures and the steps to take if you come into contact with the product. Employees are responsible for knowing where these are located. Employees must always check the MSDS, if they have not handled the product before, or are unsure about the proper procedure. A container of any controlled product will be labeled according to its hazard and the MSDS will be available to anyone dealing with it. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 34 of 64 All workers will wear personal protective equipment as required. 30.2 MSDS The three parts of WHMIS information delivery are: Labels MSDS (Materials Safety Data Sheet) Worker Training The two types of labels are: 30.3 Supplier labels Workplace labels Workplace labels must include: Name of the product, Safety precautions, and Reference to the MSDS The Nine categories of Information of MSDS 1. Hazardous ingredients – to provide information on the name, concentration and toxicity of each hazardous ingredient of a controlled product. 2. Preparation information – means the name and phone number of the person or group who prepared the MSDS, and the date of the preparation. 3. Product information – to identify the product, the supplier/manufacturer, and to describe the use of the product. 4. Physical data – information that describes the physical properties of the product, such as whether the product is a solid, liquid or gas. 5. Fire or explosion hazard – include information on how likely the product is to ignite or explode under various conditions. 6. Reactivity data – provides information on the chemical stability of the product, and how likely it is to react with other chemicals. 7. Toxicological properties – provides information on how the product enters the body and what its short and long-term health affects are. 8. Preventative measures – provides information on the measures to protect worker health and safety during the transportation, storage, use and disposal of the product, as well as emergency procedures. 9. First Aid measures – provides information for the safe evacuation and immediate treatment of anyone overexposed to a controlled product. It is the employer’s responsibility to educate any employee who works with or near hazardous agents. The education program must be workplace specific. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 35 of 64 30.4 Supplier Responsibilities a) Determine which products are controlled b) Obtain, prepare and provide information via labels and MSDS c) Revise and update information as necessary and once every three years d) The labels must be in English and French 30.5 Employer Responsibilities a) Workplace labels on all hazardous materials b) MSDS for each controlled product c) Assessment of products produced d) Worker education and training e) Provision of information in medical emergencies 30.6 Worker Responsibilities a) To work in compliance with the Act and regulations b) Participate in training c) Apply knowledge 30.7 Classification of Hazardous Material The classifications of hazardous materials are: CLASS A: Compressed Gas CLASS B: Flammable and Combustible material CLASS C: Oxidizing Material CLASS D: Poisonous and Infectious Material which includes: a) Materials causing immediate serious toxic effects b) Materials causing other toxic effects c) Biohazardous Infectious Materials CLASS E: Corrosive Material CLASS F: Dangerously Reactive Materials D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 36 of 64 31 SYMBOLS & LABEL WHMIS LOGO & SYMBOLS 31.1 WHMIS Logo WHMIS logo color Blue pantone 293 Orange pantone 151 WHMIS logo black WHMIS label border 31.2 WHMIS HAZARAD SYMBOLS There are eight WHMIS hazard symbols. Employers must train workers to recognize these symbols and to know what they mean. CLASS A: COMPRESSED GAS This class includes compressed gases, dissolved gases, and gases liquefied by compression or refrigeration. CLASS B: FLAMMABLE AND COMBUSTIBLE MATERIAL This class includes solids, liquids, and gases capable of catching fire in the presence of a spark or open flame under normal working conditions. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 37 of 64 CLASS C: OXIDIZING MATERIAL These materials increase the risk of fire if they come in contact with flammable or combustible materials. CLASS D: POISONOUS AND INFECTIOUS MATERIAL Division 1: Materials Causing Immediate and Serious Toxic Effects These materials can cause death or immediate injury when a person is exposed to small amounts. Examples: sodium cyanide, hydrogen sulphide. CLASS D: POISONOUS AND INFECTIOUS MATERIAL Division 2: Materials Causing Other Toxic EFFECTS These materials can cause life-threatening and serious long-term health problems as well as less severe but immediate reactions in a person who is repeatedly exposed to small amounts. CLASS D: POISONOUS AND INFECTIOUS MATERIAL Division 3: Biohazardous Infectious MATERIAL These materials contain harmful micro-organisms that have been classified into Risk Groups 2, 3, and 4 as determined by the World Health Organization (WHO) or the Medical Research Council of Canada. CLASS E: CORROSIVE MATERIAL This class includes caustic and acid materials that can destroy the skin or eat through metals. Examples: sodium hydroxide, hydrochloric acid, nitric acid. CLASS F: DANGEROUSLY REACTIVE MATERIAL These products may self-react dangerously (for example, they may explode) upon standing or when exposed to physical shock or to increased pressure or temperature, or they emit toxic gases when exposed to water. 32 GENERAL DOCUMENTATION GUIDE Staff is to document according to the policy of the operator utilizing their approved forms and, those provided by AdvoCare. A reminder that all documentation is to adhere to standards as follow: D:\533561087.doc All entries must be signed by the person writing them, along with their classification. Do not leave blank lines between entries. Approved by: PG Released by: NS Release Date: 03/29/2012 Page 38 of 64 If the line is not full, draw a single line to the end of that line or to the signature. Write exact time of entries – do not round off or chart in blocks; i.e. 0800 – 1600 hours is unacceptable. Strive to document actions and observations as close to the actual time occurrence as feasible. Late notes: The staff must write down the time of entry and refer to the actual time of the situation being referred to in the notes. To correct an error, draw a single line through the error and write “error” above that line and initial it. Ensure your notes are objective in nature and are not a forum for making accusatory or derogatory remarks about coworkers or others. Subjectively – affected by personal emotion and bias. Objectively – not influenced by personal feelings or opinions. Objective reports should not contain the words: “I think”, “I believe”, “she seemed”….all of these are leaders into personal opinions and bias. Be concise, record only the essential facts and stay observant but detached. “Cheat sheets” are discouraged as this practice leads to errors and gaps in timely communication and documentation. Staff is advised to utilize the company’s and the contract partner’s approved avenues of communication and documentation. Should an employee choose to use “cheat sheets” during a shift, please ensure the following to minimize associated risk.: a) Do not allow the practice to replace required documentation at the time, b) Avoid sharing your cheat sheet notes with others as they may be incomplete etc., c) Ensure such notes are placed in appropriate box for shredding (not brought home in pocket etc) and d) be mindful of your responsibility to ensure approved and proper avenues to communicate, report & document are complete. 33 MEAL PLANNING, DELIVERY & SUPPORT OF LIBERALIZED NUTRITION We recognize that proper nutrition is of significant value to a person's health, enjoyment and sense of well being. Accordingly, AdvoCare adheres to public health, food safe guidelines and, related policies and procedures as directed by contract partners regarding food storage, preparation and serving. Items placed in fridges must be dated & initialed by staff placing them there and contents of fridges checked daily to ensure dated items are discarded routinely. AdvoCare recognizes residents’ right to choose and support such choice though, foster environments where individuals are making informed decisions where possible and reasonable. In general, AdvoCare defers to the direction of the dietician and/or Director of Nursing in homes to which we may be providing care in. AdvoCare strives to offer healthy choices and, where indicated to minimize risk, modification of food products as recommended by a Speech and Language Pathologist. Where provision of a food or beverage is likely to cause significant harm (ie: choking risk, brittle diabetic) and, the client or resident is unable to make an informed decision (weigh risks and benefits), AdvoCare employees will refrain from providing the substance considered harmful and will offer an appealing alternative or, consult with the nurse in charge for further direction. AdvoCare will D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 39 of 64 collaborate with contract partners and/or health care professionals – specifically a Registered Dietician or Speech and Language Pathologist - to gain agreement on acceptable care plan/resident day. Maintaining Food Safe certification is a condition of hire. Should you need to renew yours, please visit www.foodsafe.ca for more information (and provide evidence of completion to local office for HR purposes). General Guidelines 1. Client's religious beliefs and cultural preferences will be respected and accommodated where possible. 2. Diet restrictions or modifications as recommended by a client's physician, diabetic consultant and/or dietician will be adhered to however, a client or residents’ right to choose will be respected as per statement of this policy and, in agreement with a facility’s Director of Care and/or Dietician. 3. Staff will have access to meal planning suggestions and special recipes (See Binder in Staff area "Meal Planning and Special Recipes"). 4. Teaching opportunities which may be of benefit to clients and staff will be utilized, and clients will be involved in meal planning where possible. 5. Canada's Food Guide will serve as a guideline for nutritional requirements. 6. Within a long term care environment where the focus is on quality of daily life and, persons may need incentive to eat, regular diets will be the diet of choice. Alternative diets will be adhered to as directed by the dietician and, modifications to texture as directed by the dietician or speech and language pathologist. 7. Staff will encourage hydration (unless restricted) through frequent offerings of water and other non caffeinated beverages. 8. Staff will support adequate nutrition (unless restricted) through regular offerings of high vitamin/protein/roughage snacks which are in addition to regularly planned meals. 9. Staff will modify the texture of food (unless restricted) to aid with chewing and swallowing. If unsure whether modification or offering of a food is permitted, the staff will consult with a nurse or care manager. Examples of this practice may include blending dry cake with cream or ice cream to become acceptable texture for one with swallowing issues. 10. Staff will report to coworkers/document for next shift if a resident/client has not eaten well so that more food or fluids can be offered in upcoming shifts. 11. Fortified drinks and puddings will be available as will supplementary snacks. 12. Staff will be empowered to document and report should they have concerns that a client’s nutritional requirements are not being met. 13. Special consideration, consultation and education will be sought if meal planning and support for clients with eating disorders such as Prader-Willi, anorexia, Pica, Bulimia etc. 14. Staff will document as per AdvoCare's documentation guidelines by exception regarding observations or challenges associated with meal planning or tolerance. 15. Staff will report urgent needs to the facility nurse immediately. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 40 of 64 16. Staff will, in the home environment, support clients with urgent health issue ie: choking, within their area of competency and/or contact 911. As time permits, the AdvoCare office will be notified. 17. Every effort will be made to serve meals in an esthetically pleasing manner and one by which the client /resident can access effectively and safety. Staff will ensure dialogue during the dining experience is pleasant and focused on the client or resident. 18. Staff involved in meal preparation or serving will possess a Food Safe certificate. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 41 of 64 34 Observation Memo For Program Area _____________________ Please utilize this form for outstanding issues which require the attention of an AdvoCare manager regarding issues or opportunities related to care or safety in the home (ONLY). This is NOT TO BE USED to complain about working or other relationships you may have with others in the home. Staff to ensure they adhere to approved and required avenues of documentation in the home (communication book, maintenance book etc.). This tool does not replace that primary need. Only those reports which are submitted according to professional documentation practises will be accepted – signed, dated, written in objective, evidence based manner etc. Please select the type of Memo you are describing: Employee Safety/Concerns Resident Safety/Concerns Policies and Procedures Scheduling Harassment Other Job Well Done/Positive Feedback Educational Requirements Date of Report: _____________ Date & Time of Incident: _________________________________________ Staff completing memo________________________________________________________________________ Please attach additional pages if necessary Where did the incident occur:______________________________________________________________________ _______________________________________________________________________________________________ What happened: _________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ *Who was involved: ______________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ *Who saw or heard the incident: ___________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ * Please provide full names and positions, full names of residents and/or guests/ family members involved in the incident, affected by the incident or who saw/heard the incident. Comments: _____________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ Action Plan: ____________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ _______________________________________________________________________________________________ D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 42 of 64 35 POLICY: Abuse Free Environment Reviewed Date: 11/29/11 Reviewed by: PG Approved Date: 11/29/11 Approved by: PG Released Date: 11/29/11 Released by: NS Statement At AdvoCare Health Services, we maintain and support a care and work environment that is free of harassment and discrimination and, ensures staff, residents, tenants, contract, community partners, contract partners, other contracted personnel in the worksite and visitors are treated with respect. Staff will be made aware of this policy during the Employee Information Session. Staff must sign agreement to understanding and abiding by this policy and will be empowered to address and report any incidents of harassment, abuse, bullying, violence or discrimination. Employees must agree in writing to the principles of the Code of Professional Conduct which reflects the Health Care Professionals Act and one’s Duty to Report. Residents receive the Provincial Resident Bill of Rights which is made available to them or their representative from the operator. AdvoCare’s employees shall remain mindful of tenants and residents’ rights regarding selfdetermination. This refers to adults rights to live in the manner they wish and to accept or refuse support, assistance or protection as long as they do not harm others and they are capable of making decisions about those matters. Adults are presumed capable of making decisions about their health and personal care, legal and financial matters until the contrary is demonstrated. Please refer to document CMd 3b “Basic Differences between Independent Care and Complex Care” regarding differences between role of staff supporting tenants or residents in assisted living versus complex care homes. AdvoCare recognizes there are situations especially in health care where a significant percentage of residents present with dementia and other mental health issues where, the ability to reason is significantly compromised. As AdvoCare strives to advocate for a care and work environment free of harassment, bullying, violence or discrimination, we recognize there may be limitations in the actions we take with those whose cognition is comprised. If while supporting such individuals, an employee makes the staff member feel uncomfortable, they are to report the situation to the nurse in charge for support and guidance and, if not resolved to their satisfaction, to one’s direct supervisor. Interaction which may instill discomfort includes but is not limited to discomfort caused because of discriminatory statements made by the residents, suggestive comments or actions and negative commentary. In situations where we are not able to change the behavior of the resident or, increase the comfort level of the employee through education and support and have determined withdrawing care is not justified, the employee may request in writing to be reassigned and AdvoCare will do all it can to accommodate this request. Similarly, if a resident or their advocate requests that a specific employee not provide care, to respect the personal privacy and dignity of the client and avoid putting the staff member into an uncomfortable situation, and after reasonable efforts to remedy the situation and considering all options, the resident’s request will be respected unless doing so negatively impacts D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 43 of 64 the overall care and wellbeing of other residents and staff. Such discussions will include the Site Leader and DOC/Program Manager and/or HR Director. Related Definitions – Please also refer to Policy A 21 Abuse: Deliberate mistreatment of an adult that causes the adult physical, mental or emotional harm or, damage to or loss of assets. Domestic Violence: Domestic violence is a pattern of behavior used by one person to gain power and control over another with whom he/she has or has had an intimate relationship. Domestic violence is Workplace Violence as soon as it occurs in the workplace and can threaten the safety of not only the employee victim but also his or her coworker, supervisors and clients. Neglect: Failure to provide necessary care, assistance, guidance or attention to an adult that causes, or is reasonably likely to cause within a short period of time, the adult serious physical, mental or emotional harm or substantial damage to or loss of assets. Self-neglect: Failure of an adult to take care of him/herself that causes, or is reasonably likely to cause within a short period of time, serious physical or mental harm or substantial damage to or loss of assets. Workplace Bullying: Repeated and persistent negative acts towards one or more individuals, which involve a perceived power imbalance and create a hostile work environment. Bullying may also be known as mobbing, abuse, workplace aggression, horizontal or lateral violence, victimization and social undermining. Workplace Violence: The exercise or attempt of physical force by a person against a worker, in a workplace that causes or could cause physical injury to the worker; a statement or behavior that it is reasonable for the worker to interpret as a threat to exercise physical force against the workers, in a workplace, that could cause physical injury to that worker Application 1. The HR Director/VP of Operations and CEO will be made aware of allegations related to discrimination, abuse or harassment so prompt investigation and intervention can occur in keeping with the Adult Guardianship Act and Regulations, Residential Care Legislation or, for employees, Employee Standards and Labor Relations guidelines. Abuse or neglect in any form will not be tolerated. 2. The Program Manager will ensure the Site Leader/Administrator is kept aware of concerns and investigations underway from the employer’s position including, providing evidence as required to fully investigate and resolve matters. 3. The Site Leader/Administrator serves as primary contact for licensing investigations however, AdvoCare participates in investigatory meetings upon request and makes affected employees available for interviews by licensing. 4. Abuse may include physical or emotional harm or, destruction or theft of resident, tenant, operator’s, employer’s or co-worker’s property. Abuse may include intimidation, physical or sexual assault, invasion of personal property or privacy, over or under medicating, restricting choice or access, intimidation, exploitation and/or failing to report or meet the needs of the client or others. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 44 of 64 5. Abuse can take the form of harassment as well which may include the initiation or spreading of falsehoods about another and will not be tolerated in the workplace. 6. Abuse can occur in the written form as well so staff is cautioned to not utilize accepted avenues of communication for purposes of threats, harassment, intimidation or accusations. Ensure all communication, oral or written, is objective and professional in nature. 7. Refer to policy RM 10 for more information specific to preventing violence in the workplace including, the topic of horizontal violence. 8. The HR Director, VP of Operations and CEO will be apprised of each reported incident of abuse, harassment or discrimination from or about a staff member immediately upon receipt of such a complaint and will ensure outcomes of subsequent investigations that indicate possible litigious incidents are reported to the company Director. 9. Matters that may trigger reporting to the BC Care Aide registry will be reviewed by a company Director and, approved by John Manton President prior to reporting. 10. Those involved in addressing any complaints or incidents of discrimination, abuse, neglect or harassment will maintain strict confidentiality. AdvoCare strives to protect he anonymity of those involved however, cannot assure that names or details which may lead others to deduce the source of data, can be strictly controlled. 11. Employees who knowingly allow their refusal to account for their behavior or conduct ie: decline to disclose relevant facts or intentionally mislead others are subject to discipline if such action serves to damage the legitimate business interest of the employer or compromise the well-being of those we serve. 12. Each complaint of harassment or discrimination will be documented and addressed as an incident. The incident report will generate the further report documents, interventions, followups and debriefing and will be included in the semiannual Incident Report Summary. 13. Complainants maintain the right to contact the Human Rights Commission as well as their union representative should they feel the matter has not been resolved to their satisfaction. 14. Sexually explicit, religious, political or other controversial material within the workplace is not permitted. 15. A staff member involved in acts of discrimination, harassment, neglect or abuse will be disciplined up to and including termination. 16. Employees are made aware of these principles at time of hire and, at annual education sessions and, throughout the year where need and opportunities arises. Please refer as well to policy RM10 Preventing Violence in the Workplace for employees. Policy RM11 is to be posted in staff areas at each worksite and, at AdvoCare office. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 45 of 64 36 POLICY: Non Restraint/Restraint Considerations Reviewed Date: 01/27/2009 Reviewed by: PG Approved Date: 01/27/2009 Approved by: PG Released Date: 11/10/2011 Released by: NS Statement AdvoCare recognizes that there are variations of non-restraint policies and related equipment such as bed and chair alarms and defers to the policies of the operator we are in contracts with. Employees must agree to AdvoCare’s policies which mirror those of the health authorities, regarding abuse and restraint free care as a condition of hire. AdvoCare recognizes that its’ employees may be working under the direction of external consultants such as a physiotherapist or occupational therapist and, ensures employees receive appropriate support for any new learning or direction required. Definitions related to this policy: Restraint – the use of chemical, electronic, mechanical, psychological, physical or other means of controlling a person in care’s freedom of movement, without the person’s in care’s consent. This does not include an electronic device that is only used to monitor the whereabouts of a person in care. Chemical Restraint – the administration of any medication that incapacitates the person in care. Environmental Restraint – any action or location utilized to restrict physical or social freedom. Mechanical Restraint – Includes vests, mittens, back closing lap belts or seat belts, front closure seat belts which residents can’t open, geri-chairs, table tops, lap trays, positioning devices, side rails and brakes on wheelchairs. Psychological Restraint – use of force by one or more persons. This is justified only in an emergency situation when dealing with an aggressive, violent resident. Physical Restraint – defined as any manual method, or any physical or mechanical device, material, or equipment, that is attached or adjacent to the person’s body that the person cannot remove easily, and that does, or has the potential to restrict the resident’s freedom of movement or normal access to his/her body. Application Care of residents will be according to a non restraint approach. Restraints will be considered a very unusual occurrence and will be permitted only when all alternatives have been considered, tried and failed and, are approved by the physician, Director of Care of the facility and in conjunction with the D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 46 of 64 case manager from the health authority. In such cases a risk management plan must be in place which includes frequency of resident checks (typically every 15 minutes). Staff will recognize that the use of restraints INCREASES caregiver responsibility. Ongoing assessment, monitoring and evaluation will occur as per the Emergency Restraint Policy – Restraint Free Environment (Central Okanagan Residential Services Residential Care Manual) highlights of which include: Restraints will only be used (as a temporary measure) in an emergency situation where it is required to prevent serious physical harm to the resident or others, and If the person in care consents to the use of the restraint and an Interdisciplinary Assessment has been completed. Safety and security devices may include coded or alarmed doors and bedside monitors or bed alarms. Safety devices or restraints must NEVER be used for convenience of staff or, as a substitute for effective care. Caregivers must know when and how to use such devices. Review for the need of such equipment will occur as per the policy/direction of the nursing/rehab team. Caregivers must ensure direction for use is from a nurse and, is clearly indicated on the residents’ day/plan of care. Caregivers MUST maintain awareness of the risks associated with the use of any form of restraint and monitor usage/residents’ status accordingly. Caregivers MUST intercede and report apparent risk immediately to a nurse. Staff must understand why monitoring is vital and subsequently ensure the resident being restrained is monitored (according to the operator’s policy which is typically every 15 minutes) and such monitoring is monitored on the facility’s Safety Monitoring for Temporary Physical Restraints form. All mechanical safety devices must be manufactured by a recognized health service provider and NOT have been modified in any way. Positional devices may include: Tilt recliner wheelchair Wheelchair trays Go chairs pedal chair Commode with front closure seat belt Safety belts with front closures Side rails alone are not a deterrent to a confused resident. To ensure safety and comfort: Side rails – if and where they are approved - must be in good working condition, Rails will be securely fastened to the bed frame (exception is use of ½ rails in home care environment), ½ rails are preferred over full rails, One full rail is preferred over 2 full rails and where full rails have been approved by the physio/nursing team, a risk management plan must be in place, There must be minimal space between the side rails and the mattress, Call bell and other personal items the resident may want are within reach, For those deemed at risk, a skil (bed or chair) alarm in utilized and, D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 47 of 64 The bed is in the lowest position possible while the resident is resting. Rather than restraints, the following options are to be considered: Provide companionship and supervision through family, friend, volunteers, co-residents, caregivers, added care and others, Provide physical and diversionary recreation including music, exercise, outdoor walks etc., Maintain as home like environment for the residents as possible including having familiar things in their room etc., Help residents feel safe and secure in the care environment, Implement psychosocial interventions based on the activities, interest and habits which have been part of the resident’s life and culture. Use environmental measures such as adequate lighting, glare reduction, individualized seating, coded doors, non-slip strips on the floor, well placed furniture, decreased stimulation or increased diversion. Individualized care planning, Seating and related OT assessments and plans, Visual barriers (camouflage) and secure doors, Beds without side rails though ½ rails may be indicated to provide comfort, Crash mat (mattress) on floor beside bed when resting, Appropriate assistive devices for mobility including proper footwear, Anti-tip devices on wheelchairs, Decreased or increased lighting as needed, Lowered beds – some can be 7 inches from ground, typical is 19 inches and maximum is 31 inches and Alarm systems – bed/chair pressure devices. Residents should be assessed to determine why he/she might be confused or agitated. Further investigation is warranted if there is a positive answer to any of the following: Did the symptoms appear suddenly? Does the resident have a history of UTI Are Coryzal (cold) symptoms present? Is the B12 below normal limits? Is the hemoglobin within normal limits? Is there an electrolyte imbalance? Does she/he have a catheter? Is he/she constipated? Is he/she having pain? Observe for non –verbal S&S. Has thyroid function been tested? Is he/she taking a psychotropic or hypnotic drug? Has a medication been added or discontinued? Have medications requiring serum levels been checked i.e.: Digoxin? Is a restraining device being used? Has there been recent surgery requiring general anesthetic? D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 48 of 64 Is his/her nutritional status poor? Has there been a recent fall with behavior change? Has he/she been isolated from sensory stimulation? Is there a sensory loss? Has he/she been relocated recently? Are there symptoms of clinical depression? Has he/she suffered a recent loss? Is there a history of alcohol and/or drug misuse or abuse? Refer also to Adult Care Regulations D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 49 of 64 37 POLICY: Preventing Violence In The Workplace Reviewed Date: 04/19/12 Reviewed by: PG Approved Date: 04/19/12 Approved by: PG Released Date: 04/19/12 Released by: PG Statement At AdvoCare Health Services, we maintain that staff has the right to work in a violence-free workplace and that residents, tenants and others have the right to receive care and/or reside in an environment free from violence in any manner. AdvoCare takes action to prevent violence in the workplace through education, awareness and management which includes how to recognize potential of, minimize exposure to, and respond to violence in the workplace. AdvoCare notes that the health care field carries with it a greater risk of aggression/responsive or defensive behaviors where there may be no intent to cause harm specifically supporting adults with underlying physical and psychological conditions however, takes those actions necessary to empower staff to work safely, report concerns and work within the team and medical community to investigate and mitigate further risk. AdvoCare recognizes the potential for violence in the workplace stemming from client (aka resident) to worker/worker to client/client to client/supervisor to worker/worker to supervisor and worker to worker relationships. AdvoCare also recognizes that domestic violence is workplace violence once it enters the workplace and must therefore also be considered. AdvoCare enters into contract partnerships with those who value and are in compliance with best practices to support a work and care environment which is free of violence. Refer to AdvoCare documents RM11 Abuse Free Environment, HRC f06a Code of Professional Conduct and, A 21 Approved Definitions, as well as OH&S Regulations 4.28 to 4.30. Application Potential AdvoCare employees review and sign agreement to Preventing Workplace Violence guidelines during the Employee Information Session – prior to entering the worksite. These guidelines and other supporting documents or in-service education sessions will be provided as per AdvoCare’s Annual Education Calendar (HRRf03h). D:\533561087.doc The clinical team evaluates indicators for potential or demonstrated aggressive or defensive behaviors when determining suitability for placement of a resident in the care environment given available resources, staffing levels and physical environment. The clinical team ensures a plan of care is in place for each resident which includes tips for comfort, safety and risk management plans as required. The resident is reassessed routinely and associated plans of care/Residents’ Days are updated and, relayed to staff. Care conferences or other information sharing and education which may be formal or informal in nature occurs proactively and routinely. Approved by: PG Released by: NS Release Date: 03/29/2012 Page 50 of 64 D:\533561087.doc Annual Violence and Aggression Hazard Risk Assessments will be completed for all designations at each site, including staff input. These will be completed more often, as necessary, especially if any change to work or program processes may indicate an increased risk of violence/ aggression in the workplace. In addition to guidance and interventions by the nurse, the employee is supported through ongoing education regarding the needs of the residents we serve which includes understanding of dementia, responsive (or defensive) behaviors and, related care needs as well as risk management strategies. Incident reports reflecting defensive or aggressive behavior will trigger debriefing, support to staff and resident and care management strategies to further mitigate risk. Such meetings are inclusive of all affected staff. If a resident or other in the worksite treats a staff member in a way which makes the staff member feel uncomfortable, the employee is to report the concern to the nurse in charge and, to their supervisor verbally or by an Observation Memo. This includes but is not limited to, discomfort caused by discriminatory statements made by the resident. AdvoCare recognizes there are situations in health care where a significant percentage of clients/residents present with dementia and other mental health issues where, the ability to reason is significantly or totally lacking. As AdvoCare supports a work environment free of harassment, bullying, violence or discrimination, we recognize there may be limitations in the actions we take with those whose cognition is compromised. If such a resident/client treats a staff member in a way which makes the staff member feel uncomfortable, they are to report the situation to a supervisor. In situations where the employer, in isolation or in conjunction with the operator and/or medical community are not able to change the behavior of the resident and have determined withdrawing care is not justified, the staff member may request in writing to be reassigned and AdvoCare will strive to accommodate this request. Similarly, if a resident requests that a staff member not provide care, to respect the personal privacy and dignity of the resident and avoid putting the staff member into an uncomfortable situation, and after reasonable efforts to remedy the situation and considering all options, the residents request will be respected. Reports of aggression, hostility, bullying or violence will be handled as an incident and needs to be reported on the required WSBC form and an Incident Report will be generated. A violent incident must be reported whenever an employee is threatened verbally or physically, at risk of being injured or harmed, traumatized psychologically or physically injured as a result of aggression/violence. Such reports will be investigated in a timely manner by an informed, objective company representative though, in cardinal incidents which may trigger litigation, liability, criminal implications or compromise of a contract relationship, AdvoCare may consider obtaining an independent investigator. Such investigation will include debriefing with affected personnel, witness statements, thorough documentation and where indicated, report to licensing authority and/or police. Approved by: PG Released by: NS Release Date: 03/29/2012 Page 51 of 64 Incidents will be reviewed by the OH&S committee, evaluated for effectiveness by the Program Manager in conjunction with the OH&S committee representative and, reported to the HR Director/ CEO and VP of Operations. The President is made aware of unresolved matters or those which may impact AdvoCare’s reputation/trigger insurance claims or legal representation. Staff who work or arrive at work sites alone are to park in nearby, well lit areas ensuring vehicle doors remain locked, attend inservice education on safety awareness, report any risk they may observe or become aware of and, secure door locks and or alarms at all times. In addition to the support made available through the debriefing process, Interlock counseling services is available to AdvoCare employees who are provided with the contact information directly. AdvoCare welcomes collaboration with and inservice or team building events with union representatives to reflect our joint interest in supporting workplaces which are free of violence. General Guidelines re Preventing Workplace Violence WSBC indicates: “Work should be carried out without risk or fear of safety, we are responsible for the residents, but not to the detriment of our own well being”. The nursing profession is governed by a standard, which mandates that where a nurse has been assigned to a patient, there is a legal duty to use her skills, knowledge and care as would be of a reasonably prudent nurse. The health care provider must involve other members of the team as support and to seek the safest, most appropriate action given the particular circumstance. In a residential care setting, the nurse is the primary contact for immediate interventions. Early intervention and reporting of escalation or trends in problematic behavior can prevent escalation to violence, thereby safeguarding staff and residents. What is Workplace Violence? The exercise or attempt of physical force by a person against a worker, in a workplace that causes or could cause physical injury to the worker; a statement or behavior that it is reasonable for the worker to interpret as a threat to exercise physical force against the worker, in the workplace, that could cause physical injury to the worker. What is Workplace Bullying? Repeated and persistent acts towards one or more individuals which involve a perceived power imbalance and creates a hostile work environment. Bullying may also be known as mobbing, abuse, workplace aggression, horizontal or lateral violence, victimization and social undermining. Please note bullying is also referred to as Horizontal Violence. Refer to AdvoCare’s training modules regarding this topic (in education document folder). What is Aggression? It is the verbal or physical acting out of anger or hostile feelings. Aggressive behavior may be directed towards self, other people or objects and may include agitation, restlessness, and threatened aggression, destruction of environment, self abuse or physical injury to others. What is Domestic Violence? Domestic violence is a pattern of behavior used by one person to gain power and control over another with whom he/she has or has had an intimate relationship. Domestic D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 52 of 64 violence is workplace violence as soon as it occurs in the workplace and can threaten the safety of the employee or others in the workplace. What is Hostility? It is referred to as “anger with a hook”. It shows itself in negative attitudes and behavior intended to hurt, undermine or belittle. Venting hostility often enhances a feeling of power. The manifestation of hostility often enhances a feeling of power. The manifestation of hostility ranges from rudeness to rape. Aggressive behavior is predictable in 90% of incident; thereby have the potential to be prevented. That is why it is so important for staff to report all incidents of aggression or hostility. Prompt attention to such concerns may prevent actual occurrences of abuse. Chronic exposure to verbal abuse may lead one to feel that they are at fault; therefore it is important to speak with your supervisor if any incidents arise. Criticism can be demoralizing and should not be tolerated. Reporting such behavior will result in intervention on our part so that no staff is subject to abuse. Abuse of any kind must be reported immediately. We will make arrangements for you to discuss the incident with your supervisor or HR Representative. A hand written, legible, accurate report will be required of the staff as soon after the event as possible. It should be in chronological order, dated and signed. Practical Suggestions for Dealing with Potentially Violent Situations Specific to Residential Care Settings This is supplementary information only – defer to risk management strategies, care plans, resident days, tips for comfort specific to the resident or workplace and, other guidelines reflected within this policy and education related to preventing violence in the workplace. Knowing the residents is paramount. Ensure you receive or read report at the beginning of every shift. Do report unusual behavior to the nurse for early intervention and support. Recording observations in a concise and consistent manner helps others identify patterns, precursors. Ensure others working with you are aware if behavior may be escalating. Be prepared to modify your approach and, delay planned actions according to the needs of the resident. As dementia progresses, residents lose the ability to express themselves so we must use our skills to help anticipate and understand what their needs may be. Like all of us, residents have the need and right to feel secure, valued and cared for. The old term of “behavior” has been replaced with defensive or responsive behavior….this helps remind us that he resident who is acting out is doing so as a defense mechanism. The resident may be feeling: hunger but can’t say that lost…trying to find his room fearful of people around him…he doesn’t remember faces pain…from so many sources as one ages noise…is it noisy in the dining area, are a lot of people talking at once confused by words….you are saying something but it is not understood insecurity….loss of self-esteem D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 53 of 64 grief…missing home/loved ones anxiety/altered thought processes Be familiar with the resident days/my days etc. before entering their personal space. Personal space may differ from person to person so pay attention to the resident’s body language and verbal or non verbal communication. In general, personal space/proximity is categorized as: Crowd zone (6-18 feet)…degree of comfort with which we tolerate many people around us in a public area Stranger zone (4-5 feet)…how we tolerate relative strangers in a conversation Friendship zone (3-5 feet)…we allow our best friends to be in this space Whisper zone (18 inches – 3 feet)…off limits to only those with whom we are intimate. How does the resident who is confused, anxious or paranoid perceive you? Use gentle care to help the resident feel comfortable with your presence. If that is not realized at the time, STOP. Redirection is often effective…it directs the resident away from an item or thought that is distressing. Tips to help redirect include: Validate the resident’s feelings – it is his reality, Join in that reality, listen to what they are feeling then, Distract and Redirect to new action/item/thought. Example: Validate: “You think your purse was stolen? I understand why you are upset.” Join: “You need to keep looking for your purse? I’m trying to find something too, let’s look together.” Distract: “Let’s look for your purse over there where people are having coffee.” Redirection: “That coffee smells good, do you want a cup?” Aggression develops in stages and is part of the crisis cycle. By knowing your residents and recognizing early signs of discomfort or anxiety on their part, you can greatly minimize the occurrence of violence. Consider the following strategy as you approach your daily duties in a resident focused care environment: S Stop…What you are doing if there is resistance or lack of consent T Think…Is the resident comfortable and at ease? O Observe…The residents response and receptiveness to care P Plan…Do you need to change your approach? (or obtain support from team) Observe for early signs of distress or agitation and modify your approach by referring to known tips for comfort or, conferring with the nurse and coworkers. Are you familiar with the crisis cycle….signs that behavior is escalating from anxiety to violence? D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 54 of 64 3. Physical Biting, Running away The Crisis Cycle 2. Anger and Hostility 1. Anxiety 4. Recovery General tips: D:\533561087.doc Respect the residents personal, maintain a safe distance, if possible remove objects, which may be used as a weapon i.e. cane, sharp objects. Ask permission before entering the space/touching resident’s belongings. Use a gentle approach to the resident, make genuine/courteous eye contact and use positive body language. Introduce or remind the resident of who you are…you are there to help, be mindful of the inflection of your voice. Use the name the resident likes to be called by, know in advance whether he is comfortable with others in his personal space or, whether you should maintain a distance. Speak slowly, brief, clear statements at a time. Allow enough time for the resident to think through the statement and respond. Provide visual clues where possible….show him the pudding to eat/offer the spoon. Maintain open, non threatening body language yourself - open posture, do not stare, hands at your side, and palms turned outwards. Give positive redirection using simple statements and visual clues where possible ie: Let’s go for walk. Give client an opportunity to choose “shall we go over there?” Do not issue threats or make unrealistic promises. Do not minimize or argue with their views i.e. “that is silly”, or “it could not be that bad”. Encourage the person to talk i.e. “go on”, “I see”. Stay calm and patient. Be mindful of what your body language is saying…do you look rushed? Use gentle touch if appropriate and with permission though not if a resident appears agitated. In such cases, one must maintain a physical distance. Where possible, match the resident’s voice pace and slow it down. Do not ask why, ask how and when…avoid quizzing the resident. Approved by: PG Released by: NS Release Date: 03/29/2012 Page 55 of 64 If the resident resists care, walk away and return later….do not attempt to force a resident to do something. Remain aware of exits and don’t allow yourself to be blocked into a corner if the resident appears volatile. If you observe signs of aggression, STOP, remove yourself from the space and seek support and report. Know the Code White Policy! (included in each employee handbook part two, specific to the workplace) The above principles may also apply to worker to worker/intruder to worker and other scenarios. Remember that any incidents of aggression, bullying or violence should and must be reported. You have the right to work in a healthy and positive workplace just as the residents have the right to live in a home that is resident focused and harmonious. Tips to help you defuse! STOP, take a breath, Consider taking a break at this time or, debrief with the nurse or coworker, Don’t take what the resident said personally – understand their disease process, Be aware of yourself…what are your triggers and, What do you need to be a healthy, positive employee in the health care field….talk to your employer and/or union representative. Refer to AdvoCare’s education folder for more information on this and related topics. Speak to your Program Mgr/Coord. and/or OH&S committee for specific info. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 56 of 64 38 Residents’ Bill of Rights Residents’ Bill of Rights Commitment to care 1. An adult person in care has the right to a care plan developed: (a) specifically for him or her, and (b) on the basis of his or her unique abilities, physical, social and emotional needs, and cultural and spiritual preferences, Rights to health, safety and dignity 2. An adult person in care has the right to the protection and promotion of his or her health, safety and dignity, including a right to all of the following: (a) to be treated in a manner, and to live in an environment, that promotes his or her health, safety and dignity; (b) to be protected from abuse and neglect; (c) to have his or her lifestyle and choices respected and supported, and to pursue social, cultural, religious, spiritual and other interests; (d) to have his or her personal privacy respected, including in relation to his or her records, bedroom, belongings and storage spaces; (e) to receive visitors and to communicate with visitors in private; (f) to keep and display personal possessions, pictures and furnishings in his or her bedroom. Rights to participation and freedom of expression 3. An adult person in care has the right to participate in his or her own care and to freely express his or her views, including a right to all of the following: (a) to participate in the development and implementation of his or her care plan; (b) to establish and participate in a resident or family council to represent the interests of persons in care; (c) to have his or her family or representative participate on a resident or family council on their own behalf; (d) to have access to a fair and effective process to express concerns, make complaints or resolve disputes within the facility; (e) to be informed as to how to make a complaint to an authority outside the facility; (f) to have his or her family or representative exercise the rights under this clause on his or her behalf. Rights to transparency and accountability 4. An adult person in care has the right to transparency and accountability, including a right to all of the following: (a) to have ready access to copies of all laws, rules and policies affecting a service provided to him or her; (b) to have ready access to a copy of the most recent routine inspection record made under the Act; (c) to be informed in advance of all charges, fees and other amounts that he or she must pay for accommodation and services received through the facility; D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 57 of 64 (d) if any part of the cost of accommodation or services is prepaid, to receive at the time of prepayment a written statement setting out the terms and conditions under which a refund may be made; (e) to have his or her family or representative informed of the matters described in this clause. Scope of rights 5. The rights set out in clauses 2, 3 and 4 are subject to: (a) what is reasonably practical given the physical, mental and emotional circumstances of the person in care; (b) the need to protect and promote the health or safety of the person in care or another person in care, and (c) the rights of other persons in care. These rights are pursuant to section 4(4)(a) of the Hospital Act D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 58 of 64 39 Policy: Approved Abbreviations (and commonly referenced terms) Reviewed Date: 04/01/2011 Reviewed by: PG Approved Date: 04/01/2011 Approved by: PG Released Date: 04/01/2011 Released by: KW Statement At AdvoCare we maintain a record of commonly used abbreviations and descriptions related to core AdvoCare operations as well as those commonly referred to by our contract and related partners. This policy contains the listing of abbreviations NOT TO BE USED in a health care setting. Abbreviations will only be used when space is limited, communication is enhanced and where clarity of communication is not compromised. Application Medical abbreviations recommended or referred to in The Clinician’s Ultimate Reference (Global RPh.com), Perry & Potter Reference manual and Taber’s Cyclopedia Dictionary will be utilized as needed by AdvoCare employees. Nurses maintain responsibility for awareness and appropriate use of medical abbreviations though; the most commonly used by AdvoCare employees are noted in this policy for quick reference. Abbreviations or acronyms commonly utilized at AdvoCare Health or in keeping with contract relationships are noted in this policy. Abbreviations specific to forms utilized by AdvoCare employees are accepted as long as they are referenced in a legend on the form. Please note atomic symbols are not considered to be abbreviations therefore may be used ie: K is potassium, Na is sodium etc. This policy will be posted in staff areas and given to new office employees as part of orientation to the company. AdvoCare specific: CEO - Chief Executive Officer CFO – Chief Financial Officer CIHI- The Canadian Institute for Health Information CISO – Chief Information & Security Officer COO – Chief Operating Officer HR QAM – Human Resource Quality Assurance Manager CM – Care Manager (nursing managers, client care managers) Care Levels: Refer to Collective Agreement D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 59 of 64 OTHERS: Abuse: Deliberate mistreatment of an adult that causes the adult physical, mental or emotional harm or, damage to or loss of assets. Accident: An unplanned, unwanted event that disrupts the orderly flow of the work process. It involves the motion of people, objects or substances. AgeCare Communities of Care and Wellness – Contract partner for Harmony Court in Burnaby Association – means the BCGEU or HEU Baltic Properties – Operators of Lake Country Lodge and Manor BCGEU – British Columbia Government Employees Union Biohazardous Materials – a pathogenic organism including a blood borne pathogen, which due to its known or reasonably believed ability to cause disease in humans, would be classified as Risk Group 2, 3 or 4 as defined by Medical Research Council of Canada, or any material contaminated with such an organism CAPS- Clinical assessment protocols CCHSA – Canadian Council on Health Services Accreditation CLAC – Christian Labor Association CLBC – Community Living British Columbia – division of Provincial Government we provide service to adults or children with developmental needs Common-law spouse – includes same sex and opposite sex individuals that have been living in a common-law relationship or have been co-habituating for at least 12 months CP – Care Plan, which may also be known as Resident Day (PPSL contract) or, Tenant Services Plan (Assisted Living Homes) CQI – Continuous Quality Improvement (processes) CRNBC – College of Registered Nurses of BC Day of rest – a day other than a holiday which an employee is not required to perform job duties Document Manager - ISO term referring to person who approves contents of AdvoCare documents (COO) Domestic Violence: Domestic violence is a pattern of behavior used by one person to gain power and control over another with whom he/she has or has had an intimate relationship Domestic violence is Workplace Violence as soon as it occurs in the workplace and can threaten the safety of not only the employee victim but also his or her coworker, supervisors and clients Employee – a member of the bargaining unit – refer to ca regarding categories EIS – Employee Information Session where applicants learn more about conditions of hire to which they must agree to in writing prior to becoming an AdvoCare employee Employer – refers to Slizek Investments Inc. dba AdvoCare Health Services ERP – Emergency Response Plan – program all new office and leadership staff require copy and updates of ETA – Estimated Time of Arrival (for client who may be arriving from other location) ETD – Estimated Time of Discharge (typically from hospital or private clinic) Gold Care – scheduling and payroll system being implemented 2007 Hazard Event – The first undesired event that could start the accident sequence. HEU – Hospital Employees Union HR – Human Resources, department or personnel – coordinators or managers IHA – Interior Health Authority INTRATELA – Henri Fournier, our IT (internet technology) support ISO – International Standards Organization D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 60 of 64 KGH – Kelowna General Hospital LOA – Leave of Absence MCF – Ministry for Children & Families ML – Mountain Lake Care Centre, extended care Nelson BC (extended care facility) M/L – Message Left Neglect: Failure to provide necessary care, assistance, guidance or attention to an adult that causes, or is reasonably likely to cause within a short period of time, the adult serious physical, mental or emotional harm or substantial damage to or loss of assets Occupational Exposure – reasonably anticipated, harmful contact with blood or other potentially bio hazardous material that may result from the performance of a worker’s duties Quality Management - Term ISO utilizes to reflect what we and our partners commonly refer to as Continuous Quality Improvement, CQI or Quality Assurance P/C – Phone Call PC – Program Coordinator, works under supervision of PM PIPA – Personal Information Protection Act PIPEDA – Personal Information Protection and Electronic Documents Act PM – Program Manager for facility location P.O. – Process Owner (ISO term indicating AdvoCare rep. who approves content of docs.) P.M. – Process Manager (ISO term indicating person responsible for approving format of docs. And ensuring appropriate distribution/access rights) this role is interchangeable with the QAM. PPE – Personal protective equipment, may include physical equipment, individual engineering control and/or specific instruction. PPSL - Park Place Seniors Living (company we are contracted by for staffing in independent or assisted or extended care homes such as Sun Village, Mountain Lake and Springvalley) RAPS- Resident assessment protocols RM – Risk Management (strategies/actions) ROE – Record of Employment RUGS - Resource utilization groups Routine Practices – formerly referred to as Universal Precautions Safety Engineered Needles – include a self-sheathing needle device and a retractable needle system Self-neglect: Failure of an adult to take care of him/herself that causes, or is reasonably likely to cause within a short period of time, serious physical or mental harm or substantial damage to or loss of assets. Spouse – indicates husband, wife and common-law spouse STML – Short-term memory loss SV – Sun Village (Park Place Independent Living Home we staff in Penticton) Sup.V – Supervised Visits TBA – To Be Announced TOC – Table of Contents TSP - Tenant Services Plan Union – indicates BC Government and Service Employees’ Union (BCGEU) and/or Hospital Employees Union (HEU), Workplace Bullying: Repeated and persistent negative acts towards one or more individuals, which involve a perceived power imbalance and create a hostile work environment. Bullying may also be known as mobbing, abuse, workplace aggression, horizontal or lateral violence, victimization and social undermining. D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 61 of 64 Workplace Violence: The exercise or attempt of physical force by a person against a worker, in a workplace that causes or could cause physical injury to the worker; a statement or behavior that it is reasonable for the worker to interpret as a threat to exercise physical force against the workers, in a workplace, that could cause physical injury to that worker Worksite – refers to various facilities or communities we serve, WSBC – Work Safe BC Common Medical Abbreviations: ac ADL abd. ad. Lib amt Appt. b.i.d. BM BP BR c C&S C.A.T./C.T. C.O.L.D. C.O.P.D. c/o Ca Cap cath. CHF CNS CPR CVA D.A.T. Daily D.O.B. discharge Dx E.C.T. E.E.N.T. ECG/EKG EEG Emerg. G.I. G.U. gtt. H. Hx D:\533561087.doc before meals Activities of daily living Abdomen as desired amount appointment twice a day bowel movement blood pressure bathroom with culture & sensitivity computerized aerial tomography Chronic Obstructive Lung Disease Chronic Obstructive Pulmonary Disease complains of cancer capsule(s) capsule congestive heart failure Central Nervous System Cardio Pulmonary Resuscitation cerebrovascular accident diet as tolerated daily date of birth discharge diagnosis electroconvulsive therapy eye, ear, nose & throat electrocardiogram electroencephalogram Emergency gastrointestinal genitourinary drop(s) hour history Approved by: PG Released by: NS Release Date: 03/29/2012 Page 62 of 64 HOB head of bed I&O Intake & Output i.e. that is incont./inc. incontinent IV intravenous kg. Kilogram l litre lb. pound Med(s) medication Mg milligram Min. minute(s) mL millilitre MSU Midstream urine NAS no added salt N.A. sugar no added sugar NKA no known allergies N.O.K. next of kin neg. negative NPO nothing by mouth NYD not yet diagnosed O.T. Occupational Therapy O2 oxygen PRN when necessary Pericare Perineal, as in pericare Physio physiotherapy p.m. afternoon/evening PT Prothrombin time PTO-pto please turn over Q every Qam every morning qlh every one hour q2h every 2 hours q4h every 4 hours qam every morning use daily use daily q.i.d. four times a day every other day every other day q.s. quantity sufficient qh every hour ROM range of motion Rehab. Rehabilitation Rt. Right Rx prescription s without SOB short of breath sang. of blood, sanguineous spec specimen D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 63 of 64 stat. supp. susp. T.B. T.I.A. t.i.d. T.O. T.U.P.R. tab. tbsp. TPR tsp. unit URI UTI ung. v.o. v.s. vag. w.b.c. w/c wt. immediately Suppository Suspension tuberculosis transient ischemic attacks three times a day telephone order Trans-urethral prostatic resection Tablet tablespoon temperature, pulse, respiration teaspoon unit upper respiratory infection urinary tract infection Ointment verbal order Vital signs (being TPR) Vaginal white blood cell count wheel chair weight Abbreviations NOT TO BE Used! Do Not Use Use Abbreviation Correction U IU unit unit QD QOD OD OS OD D/C cc μg AD, AS, AU BT IJ IN HS/ hs OJ daily every other day daily, right eye left eye both eyes discharge ML or millilitre mcg “right ear”, “left ear”, “each ear” “bedtime” “injection” “intranasal” or “NAS” “half-strength” or “bedtime” “orange juice” Abbreviations Do not abbreviate for drug names drug names D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012 Page 64 of 64 Per os “PO”, “by mouth” or “orally” qhs “nightly” qn “nightly” or “at bedtime” q.o.d. or QOD “every other day” q1d “daily” q6pm “daily at 6pm” or 6pm daily” SC, SQ, sub q “subcut” or “subcutaneously” ss spell out “sliding scale”, use “one-half” or “1/2” SSRI/ SSI spell out “sliding scale (insulin)” i/d “1 daily” TIW or tiw “3 times weekly” BIW or biw “two times weekly” UD “as directed” Do Not Use Symbols Use Correction 3 M x3d > and < / (slash mark) @ & + ° Ø Use metric system for 3 days “greater than” OR “less than” “per” rather than a slash mark to separate doses at and and “hr”, “h” or “hour” the number “)” or the word “zero” Dose Designation Use Correction Trailing Zero ever use a decimal by itself after a decimal point. “Use 0.xmg” Lack of leading always use a zero before a decimal point. Use “0.xmg” zero D:\533561087.doc Approved by: PG Released by: NS Release Date: 03/29/2012
 0
0
advertisement
Related documents





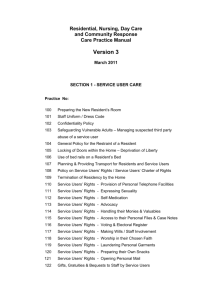


Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users