Assistive Technology Decision-Making Process
advertisement

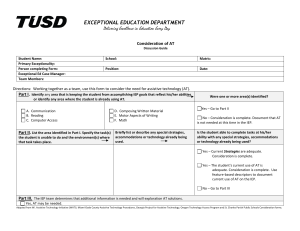
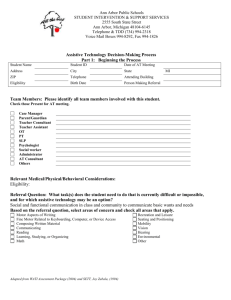
WISD 1/05 WISD Assistive Technology Decision-Making Process Form 1: Beginning the Process Student Name: Birthdate: School: IEP Eligibility: Date of Referral: Age: District: Referring person: Grade/Placement: Team Members: Please identify all team members involved with this student. Check names of those who will serve on the AT team. Name: Phone/Email: Case Manager Parent/Guardian Teacher Consultant Teacher Assistant OT PT SLP Psychologist Social worker Administrator AT Consultant Others Pertinent Medical/Physical Considerations: Health Problems Fine motor Seizures Hand/arm use Fatigue/Attention Other: Hearing Vision Behavior Referral Question: What task(s) does the student need to do that is currently difficult or impossible, and for which assistive technology may be an option? Based on the referral question, select areas of concern and check all areas that apply. Motor Aspects of Writing Recreation and Leisure Fine Motor Related to Keyboarding, Computer or Device Access Seating and Positioning Composing Written Material Mobility Communication Vision Reading Hearing Learning and Studying Environmental Math Other Refer to the AT Guide for optional assessment tools for these areas if more information is needed. Send copies of this form to: Building Principal/Supervisor Identified AT Team Members Special Ed Director Special Ed file/ca 60 Other Date Sent By: Adapted from WATI Assessment Package (2004) WISD 1/05 FORM 2: Problem Identification and Solution Generation WISD Assistive Technology Decision-Making Process Student: Date: AT Contact Person: AT Team members present: Referral Question: What task(s) does the student need to do that is currently difficult or impossible, and for which assistive technology may be an option? Student What specific parts of What is the student’s this task are difficult for present level regarding the student? this task? Environment Environmental Considerations Tasks What are the taskspecific outcomes for the student and what data would show achievement? Star (*) according to priority. Refer to the AT Guide for optional assessment tools if more information is needed. Adapted from WATI Assessment Package (2004) What has already been tried? What was the outcome? Tools Brainstorm possible solutions for the priority outcomes. Star (*) solutions to be tried first. WISD 1/05 FORM 3: Trial and Follow-Up Plan WISD Assistive Technology Decision-Making Process Student: Date: AT Contact Person: AT Team members present: Referral Question: What task(s) does the student need to do that is currently difficult or impossible, and for which assistive technology may be an option? TASKS Task-specific Outcome(s) Being Addressed WHAT What AT will you try? How and where will you try it? HOW How will you: *Acquire the AT *Provide training *Collect data Refer to AT Guide for Optional Data Collection Tools Adapted from WATI Assessment Package (2004) WHO Who will : *Acquire the AT *Provide training *Collect data WHEN Dates for: *Trial periods *Follow-up meetings FOLLOW UP Expected Outcome Next Steps *Criteria Met? e.g. Recommendation for (Show supporting IEP, other AT to be tried, data.) comments FORM 4: AT Notes WISD Assistive Technology Decision-Making Process Student: Date Notes By: