Breathing Apparatus Medical Assessment Form
advertisement

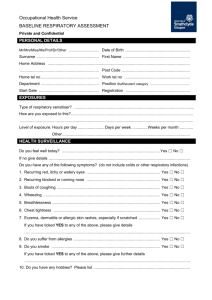
Occupational Health Service MEDICAL ASSESSMENT FOR WORKING WITH BREATHING APPARATUS Complies with Respiratory Protective Equipment at Work – A Practical Guide, HSG 53 and COSHH (2002) PERSONAL DETAILS Name .………………………………………………………………. Date of Birth …………………………………………… Department/Location .……………………………………………………………. …………………………………………… Job Title .……………..…………………………………………….. Contact No ……………………………………………. TO BE COMPLETED BY EMPLOYEE Have you ever had … 1. 2. Yes A condition affecting your heart or circulation, including any of the following: heart attack, angina, valve disease, heart surgery, high blood pressure, pacemaker, other? A condition causing any respiratory problems eg asthma, pneumonia, injury or operation to chest? 3. Diabetes? 4. A condition affecting your nervous system including any of the following: epilepsy, fit, brain surgery, stroke, head injury requiring hospital admission, blackouts, dizzy spells, problems, brain tumour/haemorrhage, other? A mental illness, including any of the following: claustrophobia, panic attacks, any other mental health condition or admission to hospital for a mental health problem? A condition affecting your eyesight including any of the following: cataract, glaucoma, eye injury, double vision, other? 5. 6. No 7. A condition affecting your joints or mobility? eg sciatica, recurrent back pain 8. Do you have difficulties with 9. Do you have any allergies? Neck movements Lower limb movements Upper limb movements Lifting/carrying loads 10. Are you taking any prescribed medicines? If “Yes”, give details …………………………………………………………………………….. 11. Do you drink alcohol? If “Yes”, how much in a typical week?.................................... 1 unit = ½ pint beer. 1 unit = 1 small glass wine. 1 unit = 1 pub measure spirits. 12. Do you smoke/have you ever smoked? If yes how many? How long did you smoke? When did you stop? …………………………………………………………………………………………. 13. Do you have any health concerns regarding this work? If you have answered “Yes” to any of questions 1-12, please give brief details ……………………………………………………………………………………………………………………………………… ……………………………………………………………………………………………………………………………………… DECLARATION I have answered all questions to the best of my knowledge and belief. I agree to notify the Occupational Health Service of any changes to my health/physical status? Signature: ……………………………………………………………………. Date: …………………………………………. Processed in accordance with the Data Protection Act 1998 Page 1 The University of Strathclyde is a charitable body, registered in Scotland, with registration number SC015263 MEDICAL ASSESSMENT Respiratory Results Measurement FVC FEV1 FEV1/FVC Predicted Actual Audiometry Results Is there wax in the external meatus? Left: Yes □ No□ Drum fully visible / partially visible / not seen Right: Yes □ No□ Drum fully visible / partially visible / not seen Any abnormalities of the external meatus? Yes □ No□ Is the tympanic membrane? Left: Normal / scarred / perforated / not seen Right: Normal / scarred / perforated / not seen Any abnormalities of the tympanic membrane? Yes □ No□ Snellen’s Test Results Left Eye 6/ Peripheral Vision Right Eye 6/ Satisfactory Both Eyes 6/ Not Satisfactory Other Results Height …………………...................... Weight............................................... BMI ………………………………… Blood Pressure …………………………………………….. Pulse………………………………………………….. Urinalysis Protein …………………..................... Glucose ........................................... Blood ………………………………… 1. 2. Medically fit for working with Breathing Apparatus? Referred to Occupational Health Physician? Yes No Yes No Nurse Signature ……………………………………………………………………… Page 2 Date …………..……………………