registration form
advertisement

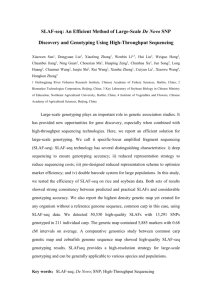
UQBR Registration Request Form – Embryo Thaw and Rederivation Date: ____________________________________________________________________________________ Contact Details Chief Investigator Name: Email Address: Department/Institute: Contact Researcher/Alternative Contact Name: Email Address: Department/Institute: Fax: Contact Phone: Contact Phone: After Hours Phone Contact: Billing/Mailing Address: Dept/Building/Street Address: ____________________________________________________________________________________ Animal Ethics Approval Details (Please attach a copy of the AEC Approval Certificate) AEC Approval No.: Expiry Date: Project Title: IBC/OGTR No: Dealing Type (eg DNIR, NLRD): ____________________________________________________________________________________ Service Required: Embryo Thaw and Rederivation of mouse lines Mice Details Number of strains: ........................................................................................................................ Name of strain/s: .......................................................................................................................... Number of straws/vials available: ............................................................................................... Storage site if not TASQ: ………………………..................................................................................... Screening requirements: All progeny from rederivation will be tissue sampled for genotyping. This will ensure that all mice born from the rederivation are of the correct genotype required by the Client. Samples to be: Collected at AIBN stores Shipped to client. Shipping Address for samples: ………………………………………………………………. ……………………………………………………………………………………….………………………………………………………… Sent to genotyping service. Name and contact for genotyping company: …………………………. …………………………………………………………………………………………………………………………………………………. Strain Description Name of strain (ie short name, what do you call it): Official Nomenclature of Strain Name (Please use information from the IMSR (http://www.findmice.org/index.jsp) or MGI (http://www.informatics.jax.org/) websites if possible and include MGI Accession # if relevant): Other Pseudonyms: If obtained from a commercial institution (eg JAX) please provide Stock No.: Date Acquired: Type of Genetic Modification: Transgenic Knock out Knock in Knock down Conditional (Flox, ER, Frt) Gene-trap Other………………………….................................…… What background is the line? C57BL/6 CD1/ Outbred B6CBF1 (hybrid) 129Sv Other……………………...........................................……… How many generations has this line been backcrossed? N… What breeding protocol is required for this line? Hom x Hom Het x Het Het x Wt Other........................................................................... Are there any abnormal behavioural or physiological phenotypes in the line (eg is this line embryo lethal?)? Yes No If yes, please describe the phenotype (including time of onset). Is animal health, welfare, breeding or lifespan affected in other ways? Yes No If yes, please give details: What method of genotyping is recommended (eg standard PCR, no screening required)? Gender of animals to be genotyped: Male Female Either Please list specific references (eg Source Colony, Publishings): Gene/Allele Details (If there is more than 1 gene of interest, please attach further details. Please use information from the MGI (http://www.informatics.jax.org/) website if possible): Gene Symbol: Gene Name: Allele Symbol: Allele Name: Genetic modification (Briefly describe genetic modification): Affected organs/tissues (eg gene expressed in liver only): Please attach an abstract of the project. DECLARATION OF UNDERSTANDING AND COMPLIANCE I, the undersigned: Have read and understood the terms and conditions of TASQ's Services below and will abide by these stipulations. Understand that the service cannot be commenced until this form is returned to TASQ. Have obtained an Animal Ethics approval and quoted this number and expiry date. Have obtained OGTR approval and quoted this number. Understand that TASQ charges apply for each round of thaw/rederive. More than one round may be necessary for successful rederivation. TASQ cannot guarantee that 100% of embryo transfers will result in live births. Understand that courier costs are the responsibility of the client. Understand that agistment charges will apply once the resulting progeny are weaned. Understand that a Colony Management levy may apply to those rederived lines needing expanding prior to shipment. Have checked/read the TASQ website at http://tasq.uq.edu.au and agree to the charges listed for this service. Signature of investigator: ................................................................ Date: ............................. Signature of TASQ Director: ............................................................. Date: ............................. AIBN Building 75, University of Queensland, St Lucia, QLD 4072, Australia Tel: +61 7 3346 3468 Fax: +61 7 3346 3898 email: Elizabeth.Williams@uq.edu.au