Anticardiolipin antibodies in patients
advertisement

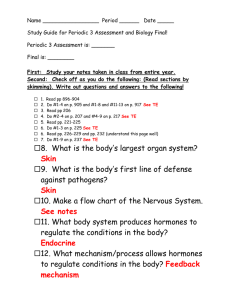
EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Fouad et al ANTICARDIOLIPIN ANTIBODIES IN PATIENTS WITH CHRONIC LIVER DISEASES By Yasser M Fouad* MD, Ashraf M Osman** MD, Hamdy Mokarrab*** MD, Taha Hasanain*** MD, Mahmoud Saad*** MD and Waffa Abdelhameed Departments of *Tropical Medicine, **Clinical Pathology and ***Internal medicine El-Minia Faculty of Medicine ABSTRACT: Anticardiolipin antibodies (aCL) are frequently found in patients with systemic lupus erythematosus and other autoimmune disorders as well as in both chronic hepatitis B and chronic hepatitis C. Aim: To study the anticardiolipin antibodies in patients with chronic liver disease and correlate its presence with clinical features in these patients. Patients and methods: This study included 60 patients with chronic liver disease (10 patients with chronic hepatitis (group A), 30 patients with liver cirrhosis (group B), 20 patients with hepatocellular carcinoma (groupC). Ten healthy persons matched to age and sex were taken as control. All patients and subjects were subjected to the following : history taking ,thorough clinical examination, abdominal Ultrasonography and -Collection of serum blood samples: for liver function tests, serological markers, alpha fetoprotein and anticardiolipin antibodies. Results: there was no statistical significant influence of age, sex, PT, PC, alphafetoprotein, or Child class on the incidence of positive aCL antibodies. The incidence of portal vein thrombosis (PVT) was lower (10.3%) in patients with positive aCL antibodies than in patients with negative aCL antibodies (12.9%). However, the incidence of positive aCL antibodies was higher in patients with positive aCL antibodies and HCC (50%) than in patients with negative aCL antibodies and HCC (28.6%). Conclusion: The aCL antibodies are commonly found in patients with chronic liver disease . The prevalent concept is that, in the majority of cases, aCL antibodies are non-pathogenic and therefore their routine determination is not justified INTRODUCTION: Antiphospholipid (aPL) antibodies are a heterogenous family of immunoglobulins that include lupus anticoagulant and anticardiolipin antibodies. The presence of these antibodies characterises primary antiphospholipid syndrome consisting of recurrent vascular thrombosis, fetal losses, and thrombocytopenia. (Hughes GRV, 1993) HCV have anti-smooth muscle antibodies, rheumatoid factor, antiliver-kidney-microsomal (ALKM) antibodies, anticaridolipin antibodies (acl), and antinuclear antibodies (ANA). (De-larranaga et al., 1996). Infection with hepatitis C virus (HCV) may lead to autoantibody response. It has been reported that chronically infected patients with Zachou et al., (2003), found no significance association between (acl) antibodies and clinical features of antiphospholipid syndrome (APS) in Biron et al., (1998), Found a high frequency of (aCL) antibodies in patients with HCV related liver cirrhosis and alcoholic liver disease. 213 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 patients with HCV infection. And concluded that (aCL) antibodies might not be pathogenic rather than being cofactor dependant. But a study conducted in patients with chronic HCV infection showed a high prevalence of immunological G (IgG) and/or (IgM) acl associated with clinical manifestations of APS. (Prieto et al., 1996). Fouad et al were separated under laminar airflow cabinet with built-ii UV lamp that provided a suitable dust- free environment. Separated sera were divided into 3 screw capped plastic tubes 2 of them will be used for deteremination of routine investigations and the other was kept frozen at minus 20 till the time of serological assay for anticardiolipin antibodies by ELISA. Aim of the Work: To study the anticardiolipin antibodies in patients with chronic liver disease and correlate its presence with clinical features in these patients. It was done in Clinical Pathology laboratory, El-Minia University Hospital. 5- Routine laboratory investigations: Liver function tests: Using an automated clinical chemistery system dimension ES, Supplied by Dupont Medical products, Wilminagton, Delaware, USA the upper limit of normal for total bilirubin is 1mg/dl (Moseley, 1996); alanine transaminase (ALT) 65u/ml, aspartate transaminase (AST) 37u/ml, and alkaline phosphatase (ALP) 136u/ml (Hultcrantz et al., 1986), serum albumin (3-5g/dl) and total protein (6.4-8.2g/dl) (Tavill,1972). Prothrombine time &concentration (P.T and P.C) was also assayed (Dade behring Inc Newark, DE 19741USA (Mammen,1994) Complete blood count on automated cell counter sysmex K 800. PATIENTS AND METHODS: This study included 60 patients with chronic liver disease (10 patients with chronic hepatitis, 30 patient with liver cirrhosis, 20 patients with hepatocellular carcinoma); they were selected from those attendants of the outpatient clinic and/or admitted to the Tropical Medicine Department, El-Minia University Hospital. The patients of liver cirrhosis and hepatocellular carcinoma were classified according to Child-Pugh classification into group A, B and C (Pugh et al., 1973). Ten healthy persons matched to age and sex were taken as control. All patients were subjected to the following: 1-Careful history taking : 2-Thorough clinical examination: 3-Abdominal Ultrasonography: 4-Collection of serum blood samples: 6- Serological assays: A) Hepatitis B virus surface antigen (HBsAg): The Kit was supplied from Hoechst Orient SAA, Germany. Behring ELISA Processor II apparatus was used for its determination. B) Hepatitis C virus antibody (HCV ab): The kit was supplied from Innotest HCV-Ab III, Innogenetics, Belgium. Behring ELISA Processor II apparatus was used for its determination. About 10 ml of venous blood sample was obtained from each patient and control by sterile clean venpuncture and evacuated in a plain tube, allowed to clot at 37" C for 20 min and centrifuged at 3000r pm. The sera 214 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 HCV-RNA by RT-PCR: The kit was supplied from Promega Inc., USA. Reaction mixtures consisted of 5 ul of target, 100 pmol of each of the oligonucleotide primers, 1.25 U of the enzyme Taq polymerase (Perkin-Elmer cetus, Norwalk, Conn.), 200uM (each) deoxynucleotide triphosphate (Boehringer Mannheim, Indianapolis, Ind.), 5 ul of 10x reaction buffer (500mM KCL, 100mM tris-HCl [PH 8.3], 15mM Mgcl2, 0.01% gelatin), 10 ul of a50% glycerol solution, 25 ug of isopsoralen per ml, and high pressure liquid chromatography-grade distilled water to atotal volume of 50ul in a microcentrifuge tube. C) Serum alpha-fetoprotein (AFP): (Only for patients with HCC on top of chronic liver disease); By ELISA technique. D) Anticardiolipin antibodies by ELISA: Fouad et al * Assay procedure: One hundred uL of positive control/calibrator, negative control and diluted test specimens were dispensed into wells. Then were incubated for 30-35 minutes at room temperature (18-25`c). All wells were filled with diluted wash buffer (300 UL per well), then were shake into disposal container, it was done for three times, the wells were blotted thoroughly on absorbent paper after the last wash. One hundred uL enzyme tracer were pipette , then were incubated for 30-35 minutes at room temperature (18-25`C). Washing step was repeated. One hundred of chromogen were pipetted into all wells then were incubated at room temperature (1825`C)for 9-10 minutes, away from light. 50 ul of stop solution were dispensed into all wells in the same order and at the same rate as for chromogen, and were mixed by gently tapping the plate. The color changed from blue to yellow. The absorbance of each well was measured at 450/620-690 nm. By special equation anti-cardiolipin concentration was obtained. * Principle of the assay: The kit is a solid-phase enzyme immunoassay. Microtitre wells are coated with cardiolipin and B2glycoprotein (B2-GPI, apolipoprotein H), the latter being cardiolipin cofactor, which forms complexes with cardiolipin. The presence of cardiolipin and B2-glycoprotein l complexes allows specific cardiolipin antibodies to bind to the solid phase. Antigenprecoated microplate wells are incubated with controls and serum specimens. During the incubation, antibody present in the test sample binds to the coated wells. Horseadish peroxidase-cojugated anti-human IgM and IgG is incubated in the wells to recognize the autoantibodies bound to the coated wells. Chromogen is added and autoantibodies are measured using a spectrophotometric plate reader. At the end of each incubation, aspirating and washing remove the unbound material. STATISTICAL METHODS: Data were statistically represented in terms of range, mean, standerd deviation (±SD), and percentage of the total number. Comparison between different groups in the present study was done using analysis of variant tests (ANOVA), Chi square tests and multiple linear regression test. A probability values (P value) less than 0.05 was considered significant (S), less than 0.01considered highly significant (HS), and less than .001 considered significant (VHS). All statistical calculations were done using 215 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 computer programs Microsoft Excel version 5 and SPSS (statistical Package For Social Science) statistical program. Fouad et al PC, alpha-fetoprotein, or Child class on the incidence of positive aCL antibodies. The incidence of portal vein thrombosis (PVT) was lower (10.3%) in patients with positive aCL antibodies than in patients with negative aCL antibodies (12.9%). However, the incidence of positive aCL antibodies was higher in patients with positive aCL antibodies and HCC (50%) than in patients with negative aCL antibodies and HCC (28.6%). The results are shown in tables (1-10) and figures (1-2) RESULTS: This study included 60 patients with chronic liver disease (10 patients with chronic hepatitis (group A), 30 patients with liver cirrhosis (group B), 20 patients with hepatocellular carcinoma (groupC)). Ten healthy persons matched to age and sex were taken as control. There was no statistical significant influence of age, sex, PT, Table (1): The demographic data of the different groups of patients with chronic liver disease and the control. Demographic data Age (mean±SD) Male Sex Female Residence Rural Urban Group A (N=10) 49.7±7.3 4 40% 6 60% 8 80% 2 20% Group B (N=30) 51.3±10.7 15 50% 15 50% 23 76.7% 7 23.3% Group C (N=20) 54.3±8 14 70% 6 30% 20 100% 0 0% Controls (N=10) 36.7±14.9 5 50% 5 50% 2 20% 8 80% Table (2): Thrombotic complications in the studied groups of patients with chronic liver disease. Thrombosis Group A Group B Group C P-value (N=10) (N=30) (N=20) 0 0 7 0.002** PVT 0% 0% 35% 0 1 0 DVT 0% 3.3% 0% 10 29 13 No thrombosis 100% 96.7% 65% (Data are expressed as number and percent (%). Kruskal-Wallis test was used. ** high significant). 216 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Fouad et al Table (3): Showed the relation between the presence of aCL antibodies and the age of patients with chronic liver disease. Age Median (range) P-value ACL antibodies Positive patients Negative patients (N=29) (N=31) 52.5 54.5 (45-67) (35-70) 0.59 NS (Data are expressed as median (range). Mann-Whitney test was used for comparing positive and negative aCL antibodies s groups. NS: non significant). Table (4): Showed the relation between the presence of aCL antibodies and the sex of patients with chronic liver disease. Sex aCL antibodies Positive patients (N=29) 17 Male Female Negative patients (N=31) 16 58.6% 51.6% 12 15 41.4% P-value 48.4% 0.58 NS (Data are expressed as number and percent (%). Chi-square test was used. NS: non significant). Table (5): Relation between Child's classification of patients with positive and patients with negative aCL antibodies. Child class. Child A Child B Child C aCL antibodies Positive patients Negative patients (N=29) (N=31) 6 3 20.7% 9.7% 13 11 44.8% 35.5% 10 17 34.5% 54.8% P-value 0.23 NS 217 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Fouad et al Table (6): Relation between PC% and PT of patients with positive and patients with negative aCL antibodies. Coagulation profile PC (%) P-value PT (sec.) aCL antibodies Positive patients Negative patients (N=29) (N=31) 63 53.5 (40-67) (32-66) 0.06 NS 15.7 (15.1-20) P-value 16.6 (15.3-30) 0.20 NS (Data are expressed as median (range). Mann-Whitney test was used for comparing positive and negative aCL antibodies groups. NS: non significant). Table (7): Relation between aCL antibodies and alpha-fetoprotein in patients with HCC (n=20). Alpha-fetoprotein Median (range) P-value aCL antibodies Positive patients Negative patients (N=29) (N=31) 306.5 235.5 (111-499) (44.4-3584) 0.32 NS (Data are expressed as median (range). Mann-Whitney test was used for comparing positive and negative aCL antibodies groups. NS: non significant). Table (8): Incidence of thrombotic events (PVT) in relation to aCL antibodies in patients with HCC (n=20). PVT No PVT HCC+Positive aCL antibodies (N=6) 3 50% 3 50% P-value HCC+Negative aCL antibodies (N=14) 4 28.6% 10 71.4% 0.35 NS (Data are expressed as number and percent (%). Chi-square test was used. NS: non significant). 218 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Fouad et al Table (9): Comparison of median of aCL antibodies in patients with HCC with and without PVT. aCL antibodies HCC with PVT (N=7) 6.1 (4.6-15.4) Median (range) HCC without PVT (N=13) 5.6 (2.3-18.9) P-value 0.241 NS (Mann-Whitney test was used. NS: non significant). Table (10): Independent risk factors for Anticardiolipin antibodies. Risk factors Beta Age .170 Child classification .018 Portal vein thrombosis -.079 Platelets -.087 ALT -.098 Sex -.15 AST -.161 PT -.162 PC -.325 Beta (multiple linear regression analysis) P value .174(NS) .922(NS) .551(NS) .592(NS) .542(NS) .961(NS) .337(NS) .513(NS) .283(NS) 100% 90% 80.00% 80% 70% 70% 60% 50% 50% 50% 40% 30% 30% 20.00% 20% 10% 0% Positive ACAs Group I Negative Group II Group III Fig. 1: Percentage of patients with positive or negative aCL antibodies in the studied patients. 219 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Fouad et al 35% 65% HCC and PVT HCC w ithout PVT Fig. 2: Incidence of PVT in-group III (HCC). protein cofactors (Roubey et al., 1995; Arvieux et al., 1995). DISCUSSION: Infection with HCV tends to induce nonspecific autoimmune reactions, as demonstrated by the high prevalence of various non-organspecific autoantibodies, usually in low titers. The non-organ-specific antibodies include the antinuclear, smooth muscle, antineutrophil, and liverkidney microsomal antibodies (Cacoub et al., 2000). Anticardiolipin antibodies (aCL) have also been reported in patients with HCV infection (OrdiRos et al., 2000). Goldberg et al., (1995) suggest that aCL-related illnesses may be familial. They determined the frequency of anticardiolipin antibodies (aCL) and their clinical sequelae in family members of aCL-positive patients, and concluded that antinuclear antibodies (ANA), aCL, and clinical events associated with antiphospholipid antibodies occur with increased frequency in relatives, but not spouses of aCL-positive probands. Both chronic HBV and chronic HDV infections are considered potent stimulants for the production of ACAs. The presence of ACAs in a great proportion of HBV-cirrhosis-related HCC patients with PVT suggests their possible participation in thrombotic mechanisms and in the hypercoagulable state that occurs in advanced liver disease and HCC (Elefsiniotis et al., 2003). The mechanism by which anticardiolipin antibodies serve their role in chronic infectious diseases is explained in different studies indicated that, as well as cardiolipin, the phospholipid binding proteins ß2glycoprotein I and prothrombin can behave as real antigens as well as Similarly, several reports have described a high prevalence of acl antibodies in chronic hepatitis C virus (Matsuda et al., 1995, Prieto et al., 1996, Violi et al., 1997, Mangia et al., 1999, Harada et al., 2000, and OrdiRos et al., 2000). It has been proposed that the release from HCV-infected cells of pro-coagulant products consisting of membrane fragments and negatively charged macromolecules might stimulate the synthesis of ACA. In most cases these antibodies are cofactor independent and of nonpathogenic type (Dalekos et al., 2000, 220 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Harada et al., 2000, and Ordi-Ros et al., 2000). However, cofactor dependency of aCL antibodies has been described in some patients with chronic HCV as reported by Alric et al., (1998) and Leroy et al., (1998). Fouad et al Further, sera from all but one anticardiolipin antibody-positive HCV patient were negative for phospholipid-dependent anti-beta2 glycoprotein I antibodies. These results suggest that anticardiolipin antibodies are frequently found in patients with chronic HCV infection, but they do not appear to be of clinical importance. In the present study, there was no statistical significant influence of age, sex, AST, ALT, PT, PC, alphafetoprotein, or Child class on increase the incidence of positive aCL antibodies. Thus, the positive aCL antibodies levels might not have a major clinical significance in patients with chronic liver diseases infected by HCV. Harada et al., (2000) reported that, immunologic disturbances induced by HCV or prolonged tissue damage in systemic organs as a result of the extra hepatic manifestations of HCV infection may induce the production of antibodies to various cardiolipin-binding proteins or phospholipids. Nevertheless, Prieto et al., (1996) showed a high prevalence of portal hypertension, thrombotic events, and thrombocytopenia. Biron et al., (1998) found more liver fibrosis in patients with HCV and aCL antibodies. In agreement with our study, most of published reports did not find a clinical significance for the presence of aCL antibodies as such reported by Matsuda et al., (1995) and Cacoub et al., (1997). Similarly, and in order to evaluate the prevalence and importance of antiphospholipid antibodies in various chronic liver diseases, Harada et al., (2000) determined the levels of anticardiolipin antibodies, platelet numbers, and levels of platelet-associated immunoglobulin G (PA-IgG) and thrombinantithrombin III complex (TAT) in patients with chronic HCV infection, chronic hepatitis B virus (HBV) infection, and primary biliary cirrhosis (PBC). The prevalence of anticardiolipin antibodies in patients with HCV infection was significantly higher than that in control subjects or individuals with the other liver diseases examined. However, there was no significant correlation between anticardiolipin antibodies and platelet counts or TAT. The frequency of thrombotic complications was similar in anticardiolipin antibody-positive and -negative patients with chronic HCV infection. Differences in demographic and genetic background, HCV subtypes, and lengths of follow up periods may explain the differences between the various studies. In the present study, the incidence of portal vein thrombosis (PVT) was 10.3% (3/29) in patients with positive aCL antibodies that were lower than its incidence in patients with negative aCL antibodies (12.9%; 4/31). However, the incidence of was higher in patients with positive aCL antibodies and HCC (50%) than in patients with negative aCL antibodies and HCC (28.6%). Some authors have found a higher prevalence of thrombotic events in aCL antibodies-positive patients than in aCL antibodies -negative patients as stated by Prieto et al., 221 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 (1996), who found that thrombotic processes occurred in 45.5% of aCL antibodies-positive chronic hepatitis C patients and in only 15.3% of those who were aCL antibodies-negative. Interestingly, some of aCL antibodies positive patients suffered from repeated thrombotic processes (myocardial infarction and retinal central vein thrombosis in one case and ischaemic stroke plus deep vein thrombosis in another case). Fouad et al It should also be recognized that antiphospholipid antibodies with pro-coagulant activity might occur in isolated cases of HCV infection (Josi and Prieto, 2003). In this respect, Alric et al., (1998) described an interesting case of a patient with HCV infection who presented with cofactor-dependent aCL antibodies and associated thrombotic disorder. In this case, interferon therapy induced elimination of the virus and negativization of cofactordependent aCL antibodies together with improvement of the thrombotic disease. Discontinuation of the therapy and a subsequent relapse of viral infection were accompanied by the reappearance of cofactor-dependent aCL antibodies and recrudescence of the thrombotic process. Oksuzoglu et al., (2003) found that anticardiolipin antibody concentrations were significantly higher in cirrhotics with portal vein thrombosis. Thus, they concluded that anticardiolipin antibodies might play a role in the development of portal vein thrombosis in cirrhosis. In a study by Elefsiniotis et al., (2003), the presence of aCL antibodies in a great proportion of HCC patients with PVT suggests their possible participation in thrombotic mechanisms and in the hypercoagulable state that occurs in advanced liver disease and HCC. The present study clearly revealed that, aCL antibodies are one of the most common autoantibodies found in patients with chronic liver disease (mainly in chronic viral hepatitis). The prevalent concept is that, in the majority of cases, aCL antibodies are non-pathogenic and therefore their routine determination is not justified. However, in particular patients with special immune reactivity or with abnormal haemostatic regulation, they may exert a pro-coagulant effect and be involved in the genesis of thrombotic events. The question as to whether aCL antibodies are purely neutral epiphenomenic autoantibodies or whether they have a role in disease progression or in the pathogenesis of extrahepatic manifestations of viral hepatitis, as yet, an unresolved issue. Most reports clearly indicate that, in chronic HCV, aCL antibodies are a mere epiphenomenon of the disease possibly secondary to activation of the clotting system in this infection as reported by Violi et al.,. (1997). Also, Mangia et al., (1999) found that, in patients with nonautoimmune liver disease, aCL production is an epiphenomenon of the liver damage and is not associated with thrombotic complications. These data do not support the hypothesis that HCV is a cause of the antiphospholipid syndrome. REFERENCES: 1. Alric L, Oskman F, GarciaRicart F, et al., (1998):. Association of antiphospholipid syndrome and 222 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 chronic hepatitis C. Br J Rheumatol 1998; 37:589-590. 2. Arvieux J, Darnige L, Caron C, et al., (1995):. Development of an ELISA for autoantibodies to prothrombin. Thromb Haemost 1995; 74: 1120–5. 3. Biron C, Andreani H, Blanc P, et al., (1998): Prevalence of antiphospholipid antibodies in patients with chronic liver disease related to alcohol or hepatitis C virus: correlation with liver injury. J Lab Clin Med 1998; 131:243-250. 4. Cacoub P, Musset L, Amoura Z (1997): Anticardiolipin, anti-b2glycoprotein I, and antinucleosome antibodies in hepatitis C virus infection and mixed cryoglobulinemia. J Rheumatol 1997, 24: 139-144. 5. Cacoub P, Renou C, Rosentha lE (2000): Extrahepatic manifestations associated with hepatitis C virus infection. Medicine 2000, 79: 47-56. 6. Dalekos GN, Kistis KG, Boumba DS, et al., (2000): Increased incidence of anti-cardiolipin antibodies in patients with hepatitis C is not associated with aetiopathogenetic link to anti-phospholipid syndrome. Eur J Gastroenterol Hepatol 2000; 12:67-74. 7. De Larranaga G., Harris EN, Pierangeli SS, et al., (1996): Low prevalence of autoimmune antiphospholipid antibodies in infectious disease of live lupus 5.521. 8. Elefsiniotis IS, Diamantis ID, Dourakis SP, et al., (2003):. Anticardiolipin antibodies in chronic hepatitis B and chronic hepatitis D infection, and hepatitis B-related hepatocellular carcinoma. Relationship with portal vein thrombosis. Eur J Gastroenterol Hepatol. 2003 Jul; 15(7):721-6. 9. Goldberg SN, Conti-Kelly AM, Greco TP (1995): A family study of anticardiolipin antibodies and associated clinical conditions. Am J Med.1995 Nov; 99(5): 473-9. Fouad et al 10. Harada M, Fujisawa Y, Sakisaka S, et al., (2000): High prevalence of anticardiolipin antibodies in hepatitis C virus infection: lack of effects on thrombocytopenia and thrombotic complications. J Gastroenterol 2000; 35:272-277. 11. Huges GRV (1993), The antiphospholipid syndrome: ten years on Lancet; 342:341-344. 12. Hughes G.R.V. (1983): Thrombosis, abortion, cerebral disease and lupus anticoagulant. B.M.J; 187; 1088. 13. Hulterantz R, Glaumann H, Lindberg G, et al., (1986): Liver investigation in 149 asymptomatic patients with moderate elevated activities of serum transaminases. Scand . j. Gastroenterol.21:109. 14. Josi Y, Prieto R. (2003) Anticardiolipin antibodies in chronic viral hepatitis. Do they have clinical consequences? European Journal of Gastroenterology & Hepatology 2003; 15(7): 717-719. 15. Leroy V, Arvieux J, Jacob MC, et al., (1998): Prevalence and significance of anticardiolipin, antibeta2 glycoprotein I and antiprothrombin antibodies in chronic hepatitis C. Br J Haematol 1998; 101:468-474. 16. Mammen E F, (1994): coagulation defects in liver diseases. 17. Mangia A, Margaglione M, Cascavilla I, et al., (1999): Anticardiolipin antibodies in patients with liver disease. Am J Gastroenterol 1999; 94:2983-2987. 18. Matsuda J, Saitoh N, Gotoh M (1995): High prevalence of antiphospholipid antibodies and antithyroglobulin antibody in patients with hepatitis C virus infection treated with interferon-a. Am J Gastroenterol 1995, 90: 1138-1141. 19. Moseley RH, (1996): Evaluation of abnormal liver function 223 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 teste. Med. Clin. North AM. Vol(80)887-906. 20. Ordi-Ros J, Villarreal J, Monegal F, et al., (2000): Anticardiolipin antibodies in patients with chronic hepatitis C virus infection: characterization in relation to antiphospholipid syndrome. Clin Diagn Lab Immunol 2000; 7:241-244. 21. Oksuzoglu G, Bayraktar Y, Arslan S, Celik I, Arslan M, Sivri B, Kirazli S, Kayhan B (2003): Portal vein thrombosis in cirrhotics: related with anticardiolipin antibodies? Hepatogastroenterology. 2003 SepOct; 50(53): 1527-30. 22. Prieto J, Yuste JR, Beloqui O, et al., (1996): Anticardiolipin antibodies in chronic hepatitis C: implication of hepatitis C virus as the cause of the antiphospholipid syndrome. Hepatology 1996; 23:199204. 23. Pugh R. N., Murray-Lyon I.M., Dawson J.L., Pietroni M .C, R. Fouad et al Williams R, (1973): Transection of the oesophagus for bleeding oesophageal varices, Br J Surg 1973;60: 646-649 24. Roubey RA S, Eisenberg RA, Harper MF, Winfield JB(1995):.‘Anticardiolipin’ autoantibodies recognize ß 2 -glycoprotein I in the absence of phospholipid. Importance of antigen density and bivalent binding. J Immunol 1995; 154:950–60. 25. Tavill AS, Robert J, Marting and Jak2 (1972): The synthesis and degeneration of liver produced protein. Gut 13:255. 26. Violi F, Ferro D, Basili S, (1997): Hepatitis C virus, antiphospholipid antibodies, and thrombosis. Hepatology 1997; 25:782. 27. Zachou K, L askos C, Christodoulou D K, et al., (2003). anticardiolipin antibodies in patients with chronic viral hepatitis are indepedant of beta 2-glycoprotein- co factor or features of antiphospholipid syndrome. Feb; 33(2): 161-8. 224 Fouad et al EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 األجسام المضادة للكارديوليبين فى أمراض الكبد المزمنة ياسر فؤاد* – أشرف عثمان** – حمدى مقرب* – طه حسانين* – محمود سعد** – وفاء عبد الحميد** أقسام *طب المناطق الحارة و**الباطنة العامة و***الباثولوجيا األكلينيكية كلية طب المنيا دلت العديد من الدراسات التى أجريت علي األجسام المضادة للكارديوليبين على مصااببتاا للعديد من األمراض الفيروسية مثل االلتااب الكبدي الفيروسي (سى) وبعض باالت مرض تليف الكبد الناتج عن إدمان الكبوليات ومنذ وقت طويل كانت أصابع االتاام تشير الى ان الفيروسات قد تسبب اإلصابة بالعديد من األمراض المناعية و ذلك عن طريق التشابه الجزيئى مع االنتيجينات الذاتية او بالتفاعل مع بروتينات الجسم ذاته إلبداث مولدات اجسام مناعية0 وماان التعااارف عليااه أن االلتااااب الكباادي الفيروسي(سااي) يصاااببه العديااد ماان األجسااام المضادة الذاتية إال أن هذه األجسام المضاد الذاتية وعالقتاا باذا المرض غير مبددة بتاى اآلن .و فى الوقت الراهن أصبح فيارو االلتاااب الكباد (ساى) موضاع اتااام مان بعاض الدراسات بأنه قد يسبب مرضاى متالزماة الفوسافات الشابمى ولااذا كاان ال ارض مان هاذه الرسااالة هااوا مباولااة معرفااة الااربط بااين اإلصااابة بماارض الكبااد وأرتفااا نساابة األجسااام المضادة للكارديوليبين ومد إمكانية وجود أعراض مرض متالزمة الفوسفات الشبمي في هذه الباالت. و قد اشتملت الدراسة على 00مريضا ,تراوبت اعماار المرضاى باين 00-00سانة وكاان عدد الذكور 23وعدد اإلناث 23ومنام 23من الريف و 2من البضر وقد تم تقسيمام الى ثالث مجموعاتا - 1مرضى مصابون بالتااب كبدي فيروسي مزمن. -3مرضى مصابون بتليف بالكبد. -2مرضى مصابون بأورام كبدية باالضافة الى 10أشخاص كمجموعة اختبار. وقد تم إجراء االتى لكل مريضا -1التعرف على التاريخ المرضى الكامل. -3إجراء فبص اكلينيكى دقيق وشامل. -2عمل أشعة تليفزيونية على البطن بالموجات فوق الصوتية. -0عمل تباليل كاملة لوظائف الكبد. -2عول اختبار لوجود الجسام المضادة للكارديوليبين . ثم بساب نتائج الدراسة وجدولتاا وتبليلاا إبصائيا .وقاد أوضابت النتاائج وجاود األجساام المضاااادة للكاااارديوليبين فاااي نسااابة غيااار قليلاااة ( )%0282مااان مرضاااى االلتاااااب الكبااادي الفيروسي. كمااا لااوبظ عاادم وجااود عالقااة بااين تواجااد مثاال هااذه األجسااام المضااادة وباادوث التجلطااات الدموية أو جلطة الوريد البابي الكبدي ,كما نفت الدراسة بدوث مرض متالزمة الفوسافات ألشبمي في مثل هؤالء المرضى . وبذلك القول ال توجد عالقة إبصائية دالة على ابتمال وجود صلة تالزم بين المرضين وفي النااية ينصح باالستمرار في الدراسات واألبباث في مثل هذا المجال . 225