Case Management Monthly Report in the Forms Section.
advertisement

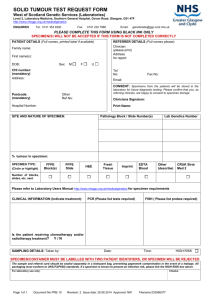
Please fill out completely for all pt.’s and send after the 2nd specimen or confirmed BLL result has been filled in. Confirmed specimen: venous 2nd capillary Childhood Lead Poisoning Prevention Program (CLPPP) Report Form Please send copy to CLPPP and place this form in the Medical Chart. Any updates made on this page please send updated form to: Lead Case Manager 275 E. Main Street HS2WA Frankfort, KY 40621 or fax to: 502-564-8389 County/Health Dept: ___________________________________________ Case Manager: ________________________________________Phone #:__________________ Name of Child: ___________________________________________DOB:__________________ Pt. Address:_____________________________________________Zip Code:__________________ Payer source: ___________________________Medicaid: Yes / No #_______________ Parent/Guardian: ________________________Relationship to child: _______________________ Guardian Ph #:__________________________Alternative Phone #:________________________ Physician: ______________________________________Phone #:________________________ Initial BLL: ________ Venous / Capillary__________µg/dL Date: ________ Venous / Capillary _________ µg/dL Date: Confirm BLL: If Initial Blood Lead level is greater than 10 ug/dL and not a venous, you must get a confirmed BLL. Verbal Risk Assessment: Child:_____Prenatal:______PerformedDate:________Positive:_____Negative:_____ Family Relocated: Yes ______No________ Relocation Address: _____________________________________________ ____________________________________________________________________________________________________ Class IIA: Blood Lead Levels at 10-14 µg/dL: Repeat BLL q 12 weeks until <10 ug/dl Home Visit if second specimen remains at this level. Parent notified of Blood Lead Level? Parent Education: C L A S S I I A Date Notified: __________ Pamphlets given and reviewed with parent: ____Lead Poisoning: Are Your Children at Risk? ____Prevent Lead Poisoning: Eat Healthy ____Pregnancy and Lead ____Other:____________________________________ Refer for WIC Services: Date:________RN initials:__________ Date:________RN initials:__________ Date:________RN initials:__________ Date:________RN initials:__________ Ref / Appt: Date: ________________ Home Visit if second specimen remains at this level. Home Visit Visual Assessment / Draw Blood Lead Level (Circle one or both) Per: RN: ____________________Environmentalist:________________ Date Performed: _______ Must make a HV with 2nd level >10 or any confirmed level >15 µg/dL For Levels: 10-14 µg/dL within 2 weeks 45-69 µg/dL within 48 hours 15-44 µg/dL within 1 week >70 µg/dL within 24 hours Family Relocated: Yes ______No________ RelocationAddress: ______________________________________________________________________________ Lead-4 07/08 Please fill out completely and send after the 2nd specimen or confirmed BLL result has been filled in. Confirmed specimen: venous 2nd capillary Childhood Lead Poisoning Prevention Program (CLPPP) Report Form Please send copy to CLPPP and place this form in the Medical Chart. Any updates made on this page please send updated form to: Lead Case Manager 275 E. Main Street HS2WA Frankfort, KY 40621 or fax to: 502-564-8389 County/Health Dept: _________________________________________________________ Case Manager: _________________________________________Phone #:____________________ Name of Child: __________________________________________DOB:______________________ C L A S S I I B & I I I C L A S S I V Class IIB &III: Blood Lead Levels 15-44 µg/dL: Repeat BLL q 1-2 months Continue with ALL of the above interventions in addition to; Medical Nutrition Therapy: Appt Date:________________/ Completed_________________ Refer to PCP for Medical Evaluation: Referral Date: __________________________________________ Performed by Physician: __________________ Medical Evaluation Date Completed: _______________ Refer to Certified Risk Assessor: Performed by: Certified Risk Assessor Name: Referral Date:___________________________________ Assessment Date with Samples Taken: ______________ Hazards Identified:__________________________ _________________________________________ (A Certified Risk Assessor is an Environmentalist who has been certified to take lead samples, if your Local Health Department or district does not have a Certified Risk Assessor, please contact the Childhood Lead Poisoning Prevention Program at 502-564-2154) Family Relocated: Yes ______No________ RelocationAddress:______________________________________________________________________________ Class IV: Blood Lead Levels 45-69 µg/dL: Repeat BLL in 48 hours Continue with ALL of the above interventions in addition to; BLL: Confirm BLL: Date: ________Venous / Capillary_____µg/dL Date: ________Venous / Capillary _____ µg/dL A venous specimen in a purple top is needed before initiating Chelation Therapy. Please refer immediately to the PCP if your HD does not draw venous lab specimens. Venous specimen submitted within 48 hours ~~~~~~~~~~~~~~~~~~ Date 2nd specimen received:______ Refer to PCP for Medical Evaluation and possible chelation ~~~ Date Referred:_________________ If referred to Specialist by PCP for chelation therapy: ~~~~~~~~~ Referred to____________________ ~~~~~ Date: _________________________ ~~~~~ Chelation Date Started: _________ If Chelation therapy initiated, BLL’s will need to be drawn q month during and post chelation until: *BLL <10µg/dL for 6 months C L A S S V * Hazards have been removed and there are no new hazards * As ordered by the physician Class V: Blood Lead Levels 70 µg/dL and greater: Repeat BLL in 24 hours Continue with ALL of the above interventions in addition to: BLL: Confirm BLL: A venous specimen in a purple top is needed before initiating Chelation Therapy. Please refer patient immediately to the PCP for Medical Evaluation. Date: ________Venous / Capillary______µg/dL Date: ________Venous / Capillary _____ µg/dL Venous specimen submitted within 24 hours~~~~~Date 2nd specimen received: __________ Referred to PCP for Medical Evaluation while awaiting results of confirmatory~~Date: _______Time:_________ If referred to Specialist by PCP for chelation therapy: Referred to_________________Date:_________________ Chelation Date Started:______________ Lead-4 07/08 Fill out with monthly updates and fax or mail copy to KY CLPPP Childhood Lead Poisoning Prevention Program (CLPPP) Monthly Report Form Place this form in the Medical Chart. Any updates made on this page please send updated form to: Lead Case Manager 275 E. Main Street HS2WA Frankfort, kY 40621 or fax to: 502-564-8389 County/Health Dept: _____________________________________________________________ Case Manager: _________________________________________Phone #:_________________ Name of Child: __________________________________________DOB:___________________ Date F/U BLL Test Results Action/Interventions Please fill out information legibly in appropriate boxes, and place BLL test results in results box only PHPR Guidelines to Case Closure: BLL <10 µg/dL for Class I and BLL <10 µg/dL for 6 months on Classes II and greater Hazards have been removed and there are no new hazards Date closed to follow-up: Reason closed: Administrative Closure procedures followed: Phone call: Date & Response:_ Letter: Date & Response: Certified Letter: Date & Response: Case Manager Signature: Lead-4 07/08