nfsc 370 clinical nutrition
advertisement

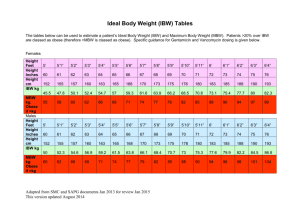
NFSC 370 CLINICAL NUTRITION Review for Exam I Fall, 2006 McCafferty In writing your responses to case study questions, I will be looking for “concise but thorough” answers. In other words, you’ll want to organize your thoughts before you begin to respond to the question. Understand all steps involved with the Nutrition Care Process. Be able to apply these steps to a case study. (Also, who are the participants in the care process? What are their respective roles? ) Know the components involved in assessing nutritional status, and be able to apply them to a case study. Example: If I give you X information about a patient, what else do you need to ask him/her? What information is missing, why is it important, and how can it be obtained? Some specifics: In terms of Anthropometric Measurements: Be able to calculate and interpret IBW range, %IBW, %UBW, and unintentional wt. loss. Be able to recognize factors that might skew your anthropometric measurements so you can take these into account when looking at a case study. In terms of Biochemical Tests: Understand each of the biochemical tests we went over in class. Know the reference values for normal albumin, sodium, and fasting glucose levels. Be able to write a SOAP note – in other words, if I give you a case study, you should be able to decipher what is nutritionally significant information, put it logically into the SOAP format, and come up with a basic plan of care (nothing fancy at this point). In terms of analyzing assessment data and coming up with a plan of care: Be able to estimate energy needs using the Harris-Benedict Equation and Long’s Method. Know the activity factors. I will provide necessary injury factors in a case study. Of course, be able to determine other nutrient needs as necessary. We’ll be using these methods throughout the semester. Remember: for protein, use actual weight if they’re not obese, adjusted weight if they are using the adjusted body weight calculation: [(ABW-IBW) x .25] + IBW Medical Nutrition Therapy: Know what a diet order is (the doctor’s order), the R.D.’s responsibilities with regard to the doctor’s order, and what the diet orders are (from NPO to Regular). Know what foods are allowed, why the diet might me nutritionally inadequate (if it is), when it would be appropriate, and how you would advance the diet (if it were appropriate to advance the diet, that is!). Be able to come up with ideas to help your patient increase his/her intake when appropriate. Be sure to think about what the patient’s problems are, and what you think the best course of action would be. The cheat sheet on the next page WILL be provided for you during your exam. 200% IBW = morbidly obese (or 100# over IBW) >120 % (130%) = obese 110 - 120 = overweight 90 - 109 = normal 80 - 89 = mild 70-79 = moderate < 70% = severe Interpreting % UBW 85-90% mild 75-84% moderate <75% severe OR wt. change (unintentional weight loss) mild moderate severe 1 week 1-2% >2% 1 month 5% >5% 3 months 7.5% >7.5% 6 months 10% 10-15% >15% albumin -5.0 = adequate 2.8= mild def. 2.1- 2.7 = moderate def. <2.1 = severe def. Transferrin Normal: Mild Moderate Severe >200 mg/dl 150-200 mg/dl 100-149 mg/dl <100 mg/dl Prealbumin (TTHY) Normal: 15-40 mg/dl Mild: 10-15 mg/dl Moderate: 5-10 mg/dl Severe: <5 mg/dl WBCs Normal: 5,000-10,000/mm3 Possible critical values: <2500 or >30,000/mm3 Total Lymphocyte Count (TLC) Normal: >1500 mm3 Mild: 1200 - 1500 Moderate: 800-1199 Severe: <800 Hemoglobin 12-16 g/dl females 14-18 g/dl males Hematocrit 12-16 g/dl females 14-18 g/dl males MCV normal: 80-953 Creatinine: 0.6-1.3 mg/dl BUN: 7-25 mg/dl Women: 655+ (9.6 x W) + (1.8 x H) - (4.7 x A)=BEE Men: 66.5 + (13.8 x W) + (5 x H) - (6.8 x A)=BEE AF = Activity Factor Bedrest 1.2 Ambulatory 1.3 IF = Injury Factor Minor Surgery 1.2 Skeletal Trauma 1.35 Major Sepsis 1.6 Severe Burns 2.1 [(ABW - IBW) X0.25] +RBW = adjusted weight Protein Normal Mild Moderate Severe 0.5 - 0.8 g/kg/day 0.8 - 1.0 g/kg/day 1.0 - 1.5 g/kg/day 1.5 - 2.0 g/kg/day