word - Nevada Compare Care
advertisement

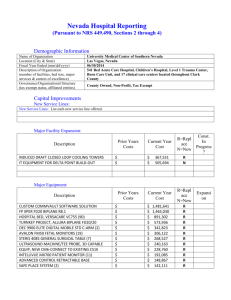
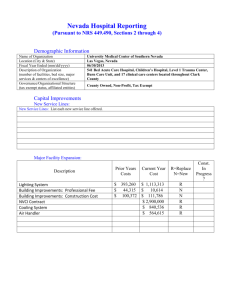
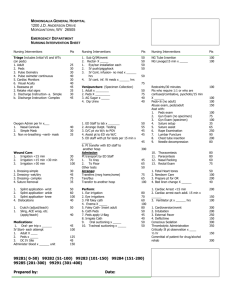
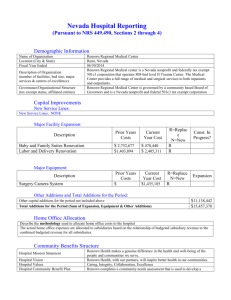
Nevada Hospital Reporting (Pursuant to NRS 449.490, Sections 2 through 4) Demographic Information Name of Organization Location (City & State) Fiscal Year Ended (mm/dd/yyyy) Description of Organization (number of facilities, bed size, major services & centers of excellence) Governance/Organizational Structure (tax exempt status, affiliated entities) Summerlin Hospital Medical Center Las Vegas, NV 12/31/2014 454 bed Acute Care Facility. Major Services: stroke center, chest pain center, emergency services, cardiovascular services, surgery, robotic surgery, sleep center, wound care, hyperbaric, orthopedic & oncology services, electrophysiology program, & extracorporeal shock wave lithotripter, women’s health services, obstetrics, neonatal intermediate care & pediatric ED, pediatric oncology, fetal assessment, occupational health services & physical rehabilitation inpatient & outpatient care. Incorporated – for profit Capital Improvements New Service Lines: New Service Lines: List each new service line offered. Major Facility Expansion: Description OR Expansion Specials Room Other Building Improvements Major Equipment: Prior Years Costs $5,940,142 $ $ $ $ $ $ $ $ $ $ $ Current Year Cost $192,754 $377,000 $418,240 $ $ $ $ $ $ $ $ $ R=Replace N=New N N N Const. In Progress? N N N Prior Years Costs $ $ $ $ $ $ $ $ $ $ $ $ $ Description Specials Room Equipment Other Fixed Equipment Pyxis Cabinet Olympus Endoscope Project Other Major Movable Equipment Current Year Cost $1,301,261 $435,996 $2,480,653 $488,079 $6,648,727 $ $ $ $ $ $ $ $ R=Replace N=New N N N N N Expansion Other Additions and Total Additions for the Period: Other capital additions for the period not included above Total Additions for the Period (Sum of Expansion, Equipment & Other Additions) $3,160,696 $15,503,406 Home Office Allocation Describe the methodology used to allocate home office costs to the hospital The corporate overhead expenses are allocated on a monthly basis to the facility based upon their monthly operating costs as a percentage of the total monthly operating costs. Community Benefits Structure Hospital Mission Statement Hospital Vision Hospital Values The Mission of Summerlin Hospital Medical Center is to achieve long-term growth and success by providing our community with superior quality health care services. Our vision is to be recognized as an organization that patients choose and recommend to families and friends, parents choose for their children, physicians prefer for their patients, purchasers select for their clients, employees are proud to be associated with. Service Excellence, Quality Care, Employee Development, Ethical and Fair Treatment of All, Teamwork, Compassion, and Innovation in Service Delivery. Hospital Community Benefit Plan (groups to target, decision makers, goals) Mission Mapping (these are not required fields) 2 Yes Does your mission map to your strategic planning process? Do you have a dedicated community benefits coordinator? Do you have a charitable foundation? Do you conduct teaching and research? Do you operate a Level I or Level II trauma center? Are you the sole provider in your geographic area of any specific clinical services? (If Yes, list services.) No Yes No No No No Yes General Peds, Peds, IMC, PICU, Peds ER, Peds OP Sedation, & Peds Gastro Community Health Improvements Services Community Health Education Community-Based Clinical Services Health Care Support Services Cab Vouchers Interpreter Services Eligibility Fees Benefit $557,717 $17,500 $1,518 $3,054 17,428 518,217 Health Professions Education Physicians/Medical Students (net of Direct GME payments) Nurses/Nursing Students Other Health Professional Education Scholarships/Funding for Professional Education Benefit $186,679 $ $116,771 $69,908 $ Subsidized Health Services Total Uncompensated Cost from Uncompensated Cost Report filed with DHCFP Less: Medicaid Disproportionate Share Payments received for the Period Less: Other Payments Received for these Accounts (County Supplemental Funds, etc.) Net Uncompensated Care Uncompensated SCHIP (Nevada Checkup) Cost Uncompensated Medicare Cost (see instructions) Uncompensated Clinic or Other Cost Other Subsidized Health Services Less: Cost Reported in Another Category Total Subsidized Health Services Benefit $26,623,541 $27,296,080 ($49,151) ($1,020) $27,245,909 ($622,368) $26,623,541 3 Research Clinical Research Community Health Research Other Benefit $ $ $ $ Financial Contributions Cash Donations (Westcare) Grants In-Kind Donations Cost of Fund Raising for Community Programs Benefit $14,817 $14,817 $ $ $ Community Building Activities Physical Improvements and Housing Economic Development Community Support Environmental Improvements Leadership Development and Leadership Training for Community Members Coalition Building Community Health Improvement Advocacy Workforce Development Benefit $ $ $ $ $ $ $ $ $ Community Benefit Operations Dedicated Staff Community Health Needs/Health Assets Assessment Other Resources Benefit $ $ $ $ Other Community Benefits (Briefly explain other community Benefits provided but not captured in sections above) Other Community Benefits Subtotal Benefit $ $ $ $ Total Community Benefit Benefit $27,382,754 4 Other Community Support Property Tax Sales and Use Tax Modified Business Tax Other Tax (Unemployment Tax) Assessment for not meeting minimum care obligation of NRS 439B.340 Total Other Community Support Benefit $6,332,217 $1,843,012 $2,112,017 $860,409 $799,120 $717,659 $ Total Community Benefits & Other Community Support $33,714,971 List and briefly explain educational classes offered Babysitting Workshop, Sibling Class, Breastfeeding Basics, Basic Infant Care, and Infant CPR. List and briefly describe other community benefits provided to the community for which the costs cannot be captured Discounted Services & Reduced Charges Policy & Procedures Charity Care Policy: (attach copies of actual policies if first filing or policy changed) Does the hospital have a policy? (Yes or No) Policy covers up to what % of Federal Poverty Level? Discounts given up to what %? Amount of time to make arrangements (in days or months) Other comments Prompt Pay or Other Discounts: (attach copies of actual policies if first filing or policy changed) Does the hospital have a policy? (Yes or No) Discounts given up to what %? Amount of time to make arrangements? (in days or months) Other comments Policy Effective Date: Yes 200% 100% (see policy) Policy Effective Date: Yes 30%+31 days 5 Collection of Accounts Receivable Policies & Procedures Effective Date of Policy Does hospital have established policy? Does hospital make every reasonable effort to help patient to obtain coverage? (Yes or No) Number of patient contacts before referral to collection agency Is collection policy consistent with the Fair Debt Collection Practices Act? (Yes or No) Methods of communication with patient (e.g. phone, letter, etc.) Number of days prior to referral to collection agency Is the patient notified in writing of referral to collection agency? Is the patient notified in writing prior to a lawsuit being begun? Other comments Yes Yes (see policy) Phone/letter (see policy) Yes Yes Chargemaster Is hospital chargemaster available in accordance with NRS 449.490 (4) requirements? (Yes or No) Is the chargemaster updated at least monthly? (Yes or No) How is the chargemaster made available? (E.g. format, location, etc.) Yes Yes PC in Central Billing Office 6