Click here to access our guide on breast nipple and skin changes

NIPPLE SYMPTOMS IN PRIMARY CARE
Nipple associated symptoms account for approximately 3-5% of the referrals to breast clinic. Most of these have no underlying breast cancer or in situ cancer (DCIS). A good history and examination of these nipple symptoms can avoid referrals to secondary care. Nipple symptoms that form part of
urgent referral criteria include a) Spontaneous unilateral blood stained/serous nipple discharge b) Recent change in nipple shape either retraction or inversion
c) Unilateral nipple eczema/nipple change that does not respond to topical treatment.
Most patients who present to primary care with nipple symptoms have no associated lump. If a lump is present, then an urgent referral to Breast clinic is required.
Nipple Discharge- Essentially, the patient will fall into either category depending upon the nature of discharge. Investigation of discharge simply with dipstick (Haemostix) testing for blood can be easily performed at the practice and patient can be reassured when the clinical examination is normal and dipstick negative for blood. In most cases discharge settles on its own. Continued, spontaneous and profuse discharge needs referral to breast clinic. Single duct persistent discharge may require surgery with microdochectomy.
Blood stained discharge (above) most likely from a single duct
Serous discharge from the nipple
A simple algorithm as below can help deciding on the most appropriate way of referral with nipple discharge;
Discharge from nipple
Watery/ Milky
Serous/Blood/ yellow green
Confirm blood on dipstick (Haemostix)
Associated with periaerolar inflammation – consider periductal mastitis- encourage stopping smoking and course of antibiotics
Physiological/secondary to stimulation/high prolactin levels due to drugs or rarely prolactinoma
Reassure if normal examination and no lumps and normal serum prolactin
Refer Breast clinic for clinical assessment/cytology/ imaging +/biopsy
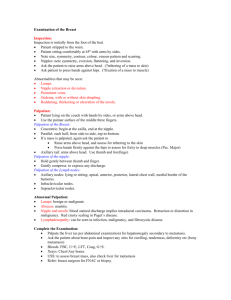
Nipple Distortion
Nipple inversion (Right) and Nipple retraction (left)
Inversion is defined as when the whole nipple is pulled in to produce a slit like appearance and retraction when part of the nipple is drawn in at the site of a single duct. Many women, during their lifetime may notice minor degree of either retraction or inversion of nipple. Bilateral nipple inversion or retraction usually has no underling sinister pathology especially when long standing and may require reassurance and referral for cosmetic correction.
Asymmetrical Symmetrical
Assess whether recent or long standing / Unilateral or bilateral / Retraction or inversion
Unilateral recent inversion or retraction in patients over 35 should require urgent referral to the breast clinic. Likely cause could be benign including duct ectasia or periductal mastitis but underlying malignancy needs excluding as it could be an early sign and patients would require assessment and imaging with mammography and or ultrasound.
Nipple skin changes including Paget’s disease of the nipple
Primary care physicians are rightly concerned about patients presenting with dermatitis or skin changes in and around nipple-areola complex. Ruling out underlying Ductal carcinoma in situ (DCIS) or invasive cancer is of paramount importance but most of these patients referred to breast clinic do not have Paget’s disease or underlying DCIS. Differentiation of dermatitis (contact or else) from
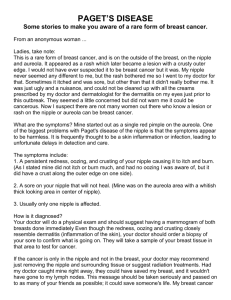
Paget’s disease of the nipple is an important issue. Paget’s disease – affects the nipple (hence
Paget’s disease of the nipple where nipple gets affected by the carcinoma cells (Paget’s cells) coming out from the milk ducts. Therefore any dermatitis/eczema of nipple not responding to topical steroids with or without bleeding from the nipple should be referred urgently to the breast clinic.
Paget’s disease of the nipple (above and below), note that it affects nipple and sparing of aereola
Dermatitis (eczema) above and below affecting mainly the areola and sparing the nipple
A guide to differences between Paget’s disease and dermatitis of the nipple/areola
Paget’s disease Dermatitis
(secondary to underlying DCIS or invasive cancer)
(no underlying DCIS or invasive cancer)
Affects the nipple (hence Paget’s disease
of nipple)
Affects the areola (if severe & chronic can involve nipple as well)
Unlikely to be bilateral- mostly unilateral presentation
In most cases bilateral or evidence of eczema elsewhere in the body
Associated with blood stained discharge Can be associated with bleeding but only on contact
No itching
Doesn’t respond to steroids
Itching can be predominant
Responds effectively to steroids
Periductal mastitis is a benign condition characterised by non cyclical pain (Mastalgia), nipple discharge and periaerolar inflammation with redness that may cause nipple retraction. It affects the major ducts producing inflammatory response. There is highly significant relationship between smoking and periductal mastitis and therefore patients should be encouraged to stop smoking as it would reduce the episodes of inflammation/infection. If untreated it can result in abscess formation
(recurrent) and mammary fistula between ducts and the skin. Where periductal mastitis fails to resolve or is associated with a lump an underlying carcinoma must be excluded and imaging and biopsy will be required and hence referral to the breast clinic is required.
Periductal mastitis with redness, inflammation around nipple areola complex with or without discharge
Learning points
Dermatitis of the nipple that doesn’t settle on topical treatment requires urgent referral to breast clinic
Blood stained discharge & distortion of the nipple needs urgent referral to breast clinic
Bilateral nipple retraction or distortion usually has no underlying sinister pathology
Antibiotics and cessation of smoking will resolve most periductal mastitis and failure to resolve and association with a lump warrants urgent
Paget’s disease with underlying carcinoma in situ (DCIS) affects the nipples with sparing of areola