Prenatal maternal anxiety & respiratory infection 1 Effect of Perinatal

Prenatal maternal anxiety & respiratory infection
1
1
2
Effect of Perinatal Anxiety on Bronchiolitis Modified by ROS-Related Genes
3 Eun Lee 1 *, MD, Hyoung Yoon Chang 2 *, MD, MS, MPH, Kyung-Sook Lee 3 , PhD, Dong In
4
Suh
4
, MD, Ho-Sung Yu
5
, MS, Mi-Jin Kang
5
, MS, In Ae Choi
6
, MA, Jinah Park
3
, PhD, Kyung
5 Won Kim
7
, MD, PhD, Youn Ho Shin
8
, MD, PhD, Kang Mo Ahn
9
, MD, PhD, Ja-Young
6
Kwon
10
, MD, PhD, Suk-Joo Choi
11
, MD, PhD, Kyung-Ju Lee
5
, MD, PhD, Hye-Sung Won
12
,
7 MD, PhD, Song I Yang
1
, MD, Young-ho Jung
1
, MD, Hyung Young Kim
13
, MD, Ju-Hee
8 Seo 14 , MD, Ji-Won Kwon 15 , MD, Byoung-Ju Kim 16 , MD, PhD, Hyo-Bin Kim 17 , MD, PhD,
10
11
9
So-Yeon Lee
18
, MD, PhD, Eun-Jin Kim
19
, PhD, Joo-Shil Lee
19
, PhD, Katherine M. Keyes
20
,
PhD, MPH, Yee-Jin Shin
21
, MD, PhD
**
, Soo-Jong Hong
1**
, MD, PhD, and the COCOA study group
12
13
14
*Eun Lee and Hyoung Yoon Chang contributed equally to this work as co-first authors.
** Soo-Jong Hong and Yee-Jin Shin contributed equally to this work as co-corresponding
15 authors.
16
17
18
19
1
Department of Pediatrics, Childhood Asthma Atopy Center, Research Center for
Standardization of Allergic Diseases, Asan Medical Center, University of Ulsan College of
20
21
2
Medicine, Seoul, Korea
Department of Psychiatry, Ajou University College of Medicine, Gyeonggi-do, Korea
22
23
4
3
Department of Rehabilitation, Hanshin University, Gyeonggi-do, Korea
Department of Pediatrics, Seoul National University College of Medicine, Seoul, Korea
5
Asan Institute for Life Sciences, University of Ulsan College of Medicine, Seoul, Korea
24 6
Sewon Infant Child Development Center, Seoul, Korea
Prenatal maternal anxiety & respiratory infection
2
25 7
Department of Pediatrics, Severance Children’s Hospital, College of Medicine, Yonsei
31
32
33
26
27
28
University, Seoul, Korea
8 Department of Pediatrics, CHA Medical Center, CHA University School of Medicine, Seoul,
29
30
Korea
9
Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of
Medicine, Seoul, Korea
10
Department of Obstetrics and Gynecology, Yonsei University College of Medicine, Seoul,
Korea
11
Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan
34
35
University School of Medicine, Seoul, Korea
12
Department of Obstetrics and Gynecology, Asan Medical Center, University of Ulsan
36
37
38
College of Medicine, Seoul, Korea
13 Department of Pediatrics, Pusan National University Yangsan Hospital, Yangsan, Korea
39
40
41
14
Department of Pediatrics, Korea Cancer Center Hospital, Seoul, Korea
15
16
Department of Pediatrics, Seoul National University Bundang Hospital, Seongnam, Korea
Department of Pediatrics, Inje University Haeundae Paik Hospital, Busan, Korea
42
43
17
Department of Pediatrics, Inje University Sanggye Paik Hospital, Seoul, Korea
18
Department of Pediatrics, Hallym University Sacred Heart Hospital, Hallym University
44
45
College of Medicine, Anyang, Korea
19
Allergy TF, Department of Immunology and Pathology, Korea National Institute of Health,
Cheongwon, Korea
46
47
48
20
Department of Epidemiology, Columbia University Mailman School of Public Health, New
York, USA
21
Department of Psychiatry, Gangnam Severance Hospital, Yonsei University College of
49 Medicine, Seoul, Korea
Prenatal maternal anxiety & respiratory infection
3
50
51
52
53
Correspondence to:
Soo-Jong Hong, MD, PhD
Department of Pediatrics, Childhood Asthma Atopy Center, Research Center for
54
55
Standardization of Allergic Diseases, University of Ulsan College of Medicine, 88 Olympicro 43-gil, Songpa-gu, Seoul 138-736, Korea
56
57
58
Tel: +82.2-3010-3379, Fax: +82.2-473-3725
E-mail: sjhong@amc.seoul.kr
59
60
Co-corresponding author
Yee-Jin Shin, MD, PhD
61
62
63
Department of Psychiatry, Gangnam Severance Hospital, Yonsei University College of
Medicine, 250 Seongsandong, Seodaumnu-gu, Seoul, 120-752, Korea
Tel: 82-2-2019-3340, Fax: 82-2-3462-4304
64
65
E-mail: yjshin@yuhs.ac
Prenatal maternal anxiety & respiratory infection
1
66
67
68
69
Abstract
Objectives : Although perinatal anxiety affects the developing immune system and susceptibility to diseases in offspring, studies on gene-environment interactions with respect to exposure to perinatal anxiety are lacking. This study aimed to elucidate the effect and
70
71 interaction between perinatal anxiety and polymorphisms in antioxidant defenses and innate immunity genes on the development of respiratory tract infections (RTIs) during the first year
72
73
74 of life.
Study design: Trait anxiety levels in 440 women were assessed by the State-Trait Anxiety
Inventory (STAI) during late gestation. The occurrence of RTIs including bronchiolitis during
75
76 the first year of life was assessed by parent-reported doctor diagnosis. Polymorphisms in glutathione S -transferase P-1 ( GSTP1 , rs1695) and CD14 (rs2569190) were genotyped using
77
78
79 the TaqMan assay. Copy number variations of GSTT1 were measured by real-time polymerase chain reaction.
Results: Exposure to higher levels of perinatal anxiety increased the risk of lower RTI
80
81
82 bronchiolitis (adjusted odds ratio [aOR] 1.30, 95% confidence intervals [CI] 1.00–1.80).
Perinatal anxiety increased bronchiolitis risk in infants with AG+GG genotype of GSTP1 or
GSTT1 null genotype (aOR 3.36 and 2.79). In the aspect of TC+CC genotype of CD14 ,
83
84 higher levels of perinatal anxiety were associated with the increased risk of upper RTI, lower
RTI, and bronchiolitis (aOR 2.51, 4.60, and 4.31, respectively).
85
86
Conclusions: Perinatal maternal anxiety levels affect the occurrence of bronchiolitis in offspring. The effect of perinatal anxiety on the occurrence of bronchiolitis during infancy
87 was modified by genetic polymorphisms in antioxidant defense and innate immunity genes.
88
89
Keywords: anxiety, bronchiolitis, CD14, perinatal, glutathione S -transferase, polymorphism,
90 respiratory tract infection
91
Prenatal maternal anxiety & respiratory infection
2
Prenatal maternal anxiety & respiratory infection
3
92
93
94
95
Introduction
Environmental factors during early life can influence the development of physiologic and
immune system and modify disease susceptibility later in life [1]. Recent studies revealed that
perinatal maternal stress and anxiety may affect susceptibility to infectious diseases in later
96
97
life [2]. In particular, respiratory tract infection (RTI), the majority of morbidity and mortality
during infancy, poses a worldwide burden that can be prevented by modification of
98
99
100
The mechanisms underlying the associations between exposure to perinatal maternal stress and an increased risk of RTIs have not been fully elucidated. Perinatal maternal stress can
101
102 cause increases in glucocorticoid levels in pregnant women, which can cross the placenta
barrier into the fetus. This might affect fetal programming through immunomodulation [5]
103
104
105 and perinatal anxiety might cause epigenetic changes in offspring with increased vulnerability
to neurodevelopmental diseases in later life [6]. However, no study has directly demonstrated
the possible mechanisms underlying the association between exposure to perinatal maternal
106
107
108 anxiety and development of RTIs in offspring.
The health effects of perinatal anxiety and RTIs share a common pathway of oxidative stress
[7, 8]. Exposure to perinatal anxiety increases the serum levels of glucocorticoid in offspring
109
110
[9], which generate higher levels of ROS. During RTIs, higher levels of ROS are generated in
the epithelium of the respiratory tract. The increased oxidative stress is associated with
111
112
alterations in immune response and affects fetal programming [10, 11].
Glutathione S-transferase (GST) subfamily plays an important role in the protection against
113
114
115 oxidative stress by catalyzing the conjugation of many compounds with reduced glutathione
GSTP1 (rs1695) and GSTT1 affect the ability to deal with the
excessive oxidative stress due to its altered enzyme activity [12]. In subjects with AG+GG
116 genotype of GSTP1 (rs1695), enzymatic activity of GSTP1 is partially reduced, compared to
Prenatal maternal anxiety & respiratory infection
4
117
the subjects with AA genotype [12]. The null genotype of
GSTT1 is associated with an
118
119
120
CD14
(rs2569190) has been known to be associated with enhanced immune response and thereby
121
122
increases the risk of RTIs [14, 15]. This suggests that these genetic variants may affect the
development of RTI and environmental factors may exaggerate the effects of these genetic
123
124
125 variations.
Therefore, we hypothesized that there are possible associations between exposure to perinatal anxiety and genetic variants involved in antioxidant defense and innate immunity and these
126
127 interactions influence RTI risk in offspring especially during early life. First, we examined the association between perinatal anxiety and RTI occurrence during the first year of life.
128
129
130
Second, we explored the effect of gene-environment interactions between exposure to perinatal anxiety and genetic variants of some of GST subfamily genes and CD14
(rs2569190) on the development of RTIs.
131
132
Methods
133
134
135
Participants
We used data from the COhort for Childhood Origin of Asthma and allergic disease
(COCOA), a prospective birth cohort study that aims to investigate the effects of
136
137 environmental and genetic factors during early life on the development of allergic diseases
and children’s health [16-18]. Women in their third trimester of pregnancy were enrolled in
138
139
140 this study from January 2009 to September 2011, when the questionnaire included State trait anxiety inventory (STAI) score. The exclusion criteria included pregnant women with pregnancy associated complications (gestational diabetes and pregnancy-induced
141 hypertension), high risk for early delivery, and delivery earlier than 36 weeks. Neonates were
Prenatal maternal anxiety & respiratory infection
5
142 excluded if they needed oxygen therapy; had congenital anomalies including congenital
143
144 diaphragmatic hernia, congenital heart disease, congenital lung diseases or severe systemic
diseases. Additional information on this ongoing cohort study are described elsewhere [19].
145
Among 734 eligible women, 71 refused to participate, 4 were lost to follow-up, and 28 were
146
147 excluded due to preterm delivery. Among a total of 631 (86%), 440 (69.7%) completed the
STAI questionnaire. Missing data on anxiety was unrelated to key demographic covariates,
148
149
150 except for the season of offspring’s birth (Table I). Information on potential confounders was obtained from a parental-reported questionnaire at the 36th week of pregnancy and medical record at child’s birth. Questionnaires were designed to assess maternal health problems
151
152 including allergic diseases (atopic dermatitis, allergic rhinitis, or asthma); socioeconomic status (income and educational levels); and prenatal environmental factors such as tobacco
153
154 smoking exposure at 36 weeks of gestation of pregnant women. Newborn’s sex and weight, gestational age, season of birth, and health conditions were collected by a questionnaire after
155 birth.
156
157
Written informed consent was obtained from all women and the study was approved by Asan
Medical Center (IRB No. 2008-0616), Samsun Medical Center (IRB No. 2009-02-021),
158
159
Yonsei Univerisity (IRB No. 4-2008-0588), and CHA Medical Center (IRB No. 2010-010).
160
161
162
Anxiety assessment
Data on perinatal maternal anxiety were obtained by self-report at the 36th week of pregnancy. The Korean version of STAI (K-STAI) was used which consists of two subscales;
163
164
165
State Anxiety (anxiety about an event) and Trait Anxiety (anxiety levels as a personal characteristic). Among the two subscales, Trait Anxiety subscale (STAI-T) was used in this study, since it reflects the baseline anxiety levels of the subjects rather than a transient state.
Prenatal maternal anxiety & respiratory infection
6
166
STAI-T is a 20 item questionnaire scored on a four-point Likert-type scale that measures a
167
168
169
general tendency to be anxious [20]. The score ranges from 20 to 80 with a higher score
indicating a more severe anxiety level. K-STAI has been shown to exhibit excellent
170
171
psychometric properties[21] and its internal consistency has been reported as having a
Cronbach’s α coefficient of 0.91 [22]. In this study, the reliability coefficient (Cronbach’s α)
of STAI-T was 0.92.
172
173
174
Assessment of 1 year outcome variables
The infants were examined at 1 year of age with at least one parent present at follow-up visits.
175
176
RTI was assessed by parent-reported doctor diagnosis of RTIs during the first year of life.
RTIs were further categorized as upper (URTIs) and lower (LRTIs) RTIs. URTIs included
177
178
179 common colds, sinusitis, otitis media, and croup; LRTIs included pneumonia, tracheobronchitis, and bronchiolitis.
180
181
182
DNA isolation and genotyping
The genomic DNA was extracted from the buffy coat of the cord blood at delivery using the
Gentra® Puregene® Blood kit (Qiagen, Maryland, USA) as recommended by the
183
184 manufacturer. The genotyping of CD14 (rs2569190) and GSTP1 (rs1695) were conducted using a TaqMan assay (ABI, Foster City, CA, USA). Assay identification numbers for CD14
185
186 and GSTP1 were C_16043997_10 and C_3237198_20, respectively. Copy number variations
(CNV) of GSTM1 and GSTT1 were measured by real-time polymerase chain reaction. The
187
188
189 primers and probe for GSTM1 and GSTT1 were synthesized according to Brasch-Andersen C,
et al..[23] Reactions were performed as a triplex, with RNAse P as the reference gene. The
allele frequencies of the polymorphisms in GSTP1 (rs1695), GSTM1 , GSTT1 , and CD14
190 (rs2569190) were in Hardy-Weinberg equilibrium ( P > 0.1).
Prenatal maternal anxiety & respiratory infection
7
191
192
193
194
Statistical analysis
We examined the association between perinatal maternal anxiety levels and RTIs (URTIs,
LRTIs, and bronchiolitis) during the first year of life, using logistic regression. Adjustments
195
196 were made for baseline demographic factors (child’s sex and maternal age) as well as known risk factors of respiratory infections, including maternal educational level, exposure to
197
198
199
tobacco smoking during the first year, presence of maternal and paternal allergic diseases [24,
200
201
The unit of STAI score used in the regression analyses was standard deviation (SD) of samples, which was 8.47. Parameter estimates were multiplied by the SD of the STAI score,
202
203
204 and for 95% confidence intervals (CI), the following equation was used: BETA*(SD of STAI score) ± 1.96*SE*(SD of STAI score). In logistic regression analysis, the estimates were exponentiated to obtain the estimate and 95% CI of the odds ratio.
205
206
207
The combined effects of perinatal anxiety and genetic polymorphisms on RTI risk were investigated by multivariate logistic regression analysis. To analyze the combined effect of the two factors, STAI scores were divided into two categories on the basis of mean levels and
208
209 genetic polymorphisms were classified according to: GSTT1 null or present, GSTM1 null or present, and polymorphisms of GSTP1 (rs1695) and CD14 (rs2569190). All statistical
210
211 analyses were performed using SAS for Windows (version 9.2).
212
213
214
Demographics
Results
Table I summarizes the descriptive statistics across the total sample. Overall, mean maternal
215 age was 32.5 years. Exposure to tobacco smoking during pregnancy was reported by 60.8%
Prenatal maternal anxiety & respiratory infection
8
216 of the women. Of mothers, 28.2% had a history of allergic disease; in spouses, the proportion
217
218
219 was 26.1%. STAI score demonstrated a normal distribution of 41.0 ± 8.47 (mean ± SD).
About half (49.3%) of the offspring were girls, with a mean gestational age of 39.2 weeks.
Births were evenly distributed among four seasons (26.6% in spring, 26.6% in summer,
220
221
21.8% in autumn, and 25.0% in winter). About a third (34.4%) were delivered by caesarean section.
222
223
Association between perinatal maternal anxiety and development of RTIs during the
224
225
226 first year of life
Higher levels of perinatal maternal anxiety were associated with an increased risk of LRTI especially bronchiolitis, but not with total RTI (Table II).
The risk of LRTIs was significantly
227
228
229 increased in infants exposed to higher levels of perinatal anxiety. For a 1 SD increase in STAI score, the odds of LRTIs risk during the first year of life were 1.35 times higher (95% CI
1.01–1.78). The crude association between perinatal anxiety levels and development of
230
231
232 bronchiolitis was weakly significant (OR 1.35, 95% CI 1.00–1.81; aOR 1.30, 95% CI 1.00–
1.80). However, perinatal anxiety did not increase the risk of URTIs (aOR 1.10, 95% CI
0.87–1.39). In addition, higher levels of perinatal maternal anxiety were not significantly
233
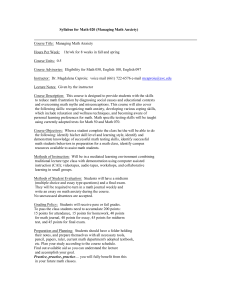
234 associated with the occurrence of each type of RTI except bronchiolitis. Figure represents the predicted probability of bronchiolitis at 1 year of age for each observed value of perinatal
235 anxiety score in the multivariate model.
236
237
238
239
Combined effect between perinatal maternal anxiety levels and GSTP1 (rs1695), GSTT1,
GSTM1 polymorphisms on the development of RTI during the first year of life
Genetic polymorphisms in GSTP1 (rs1695), GSTT1 or GSTM1 did not increase the risk of
Prenatal maternal anxiety & respiratory infection
9
240 any types of RTIs (data not shown). Exposure to higher levels of perinatal anxiety was
241
242
243 associated with an increased risk for LRTIs especially bronchiolitis in infants with AG+GG genotype of GSTP1 (rs1695), compared with infants with both exposure to lower levels of perinatal anxiety and AA genotype (aOR 2.61, 95% CI, 1.09–6.22; aOR 3.36, 95% CI, 1.25–
244
245
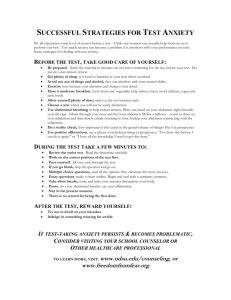
9.03, respectively; Table III). When analyzed by the three genotypes, infants with GG genotype of GSTP1 (rs1695) showed a significantly increased risk for LRTIs especially
246
247
248 bronchiolitis during the first year of life (aOR 22.04, 95% CI, 4.79–101.47; aOR 14.61, 95%
CI, 3.23–66.11, respectively) (Supplementary figure).
In addition, infants with both GSTT1
–null genotype and exposure to higher levels of perinatal
249
250 anxiety were associated with an increased risk for LRTIs especially bronchiolitis, compared with infants with both GSTT1
–present genotype and exposure to lower levels of perinatal
251
252
253 anxiety (aOR 2.47, 95% CI 1.04–5.89; aOR 2.79, 95% CI 1.05–7.43; Table IV). In terms of
GSTM1 , exposure to higher levels of perinatal anxiety increased the risk of LRTIs during the first year of life, regardless of the genotypes (present genotype: aOR, 2.95, 95% CI, 1.06–
254
255
8.17; null genotype: aOR, 2.60, 95% CI, 1.01–6.66; Supplementary table I).
256
257
258
Combined effect between exposure to perinatal maternal anxiety and CD14 (rs2569190) polymorphism on the development of RTI during the first year of life
Infants with TT genotype of CD14 (rs2569190) demonstrated an increased risk of URTIs and
259
260
LRTIs especially bronchiolitis if they were exposed to higher levels of perinatal anxiety, compared with infants exposed to lower levels of perinatal anxiety (aOR 2.51, 95% CI 1.01–
261
262
6.24; aOR 4.60, 95% CI, 1.29–16.41; aOR 4.31, 95% CI, 1.17–15.79, respectively;
Supplementary table II).
263
264 Discussion
Prenatal maternal anxiety & respiratory infection
10
265
266
267
268
Main findings
In this study, we found a positive association between exposure to higher levels of perinatal anxiety and development of RTIs in offspring during the first year of life. The risk of LRTIs, especially bronchiolitis during early infancy was modified by additive effects between
269
270 exposure to perinatal anxiety and polymorphisms in antioxidant related genes. To the best of our knowledge, this is the first study examining the gene-environment interactions with
271
272
273 respect to perinatal anxiety on the development of LRTIs especially bronchiolitis during early life.
In addition, we found that exposure to higher levels of perinatal anxiety affected the
274
275 development of RTIs especially bronchiolitis during infancy differently, according to the polymorphisms of reactive oxidative stress (ROS) detoxification genes such as GSTP1
276
277
278
(rs1695) and GSTT1 . The combined effect between exposure to perinatal maternal stress and polymorphisms of ROS detoxification genes on the occurrence of LRTI especially bronchiolitis may be partially attributable to the increased generation of ROS with exposure
279
280
281 to higher levels of perinatal maternal anxiety and LRTI especially bronchiolitis. Perinatal anxiety increases glucocorticoid levels in both mother and fetus, which induces superoxide
production [27]. The capacity to effectively detoxify ROS is affected by polymorphisms of
282
283
these genes [28, 29]. The reason for the increased risk of LRTIs, especially bronchiolitis in
infants with AG+GG genotype of GSTP1 (rs1695) or GSTT1
–null genotype in response to
286
287
288
284
285 exposure to higher levels of perinatal anxiety may be explained by partially reduced enzymatic activity in AG+GG genotype of GSTP1 (rs1695) and by the loss of enzymatic activity in GSTT1
–null genotype [28, 29]. Since GST subfamily genes are expressed mainly
in the respiratory tract and oxidative stress is increased during LRTIs including bronchiolitis
[30], genetic variants of the GST subfamily may modify the risk of LRTIs including
289 bronchiolitis.
Prenatal maternal anxiety & respiratory infection
11
290
291
292
293
Possible underlying mechanisms
Psychological stress may affect the imbalance of oxidant and antioxidant states and thereby
influence an individual’s health [31, 32]. In response to stress, serum glucocorticoid levels
294
295
296
297
298
Considering the impact of ROS in fetal programming and variants of ROS-related genes on
the capacity to detoxify ROS [11, 12], the increased susceptibility to RTIs in offspring
exposed to perinatal anxiety might be explained by their decreased ability to mitigate the
299
300
oxidative stress generated during RTIs [36].
An experimental study showed that prenatal maternal stress influences epigenetic re-
301
302
303 programming via altered expression of microRNA involved in the stress response, oxidative
stress, and metabolism [6]. In addition, prenatal anxiety-related immune and oxidative
responses can cause telomere erosion, possibly increasing the risk for infection [37, 38]. On
304
305
306 the basis of these findings, we suggest that perinatal anxiety influences susceptibility to RTIs in offspring during critical periods in combination with genetic variants of ROS-related genes or through epigenetic mechanisms. Additional studies are needed to clarify the underlying
307
308 mechanisms.
Previous studies showed that T allele of CD14159C/T is associated with enhanced
309
310 transcriptional activity and increased soluble CD14 levels, which are markers of monocyte
and macrophage activation [39, 40]. The positive relationship between perinatal anxiety
311
312
313 levels and risk of RTIs in infants with TT genotype of CD14 (rs2569190) might be associated with the essential role of CD14 as an initiator of innate immunity against viral infections in
the respiratory tract [14]. Alterations in cellular and humoral immune responses caused by the
314 interactions between exposure to higher levels of perinatal maternal stress and genetic
Prenatal maternal anxiety & respiratory infection
12
315 variants of CD14
might partially explain these findings [41, 42].
316
317
318
In this study, we proposed that perinatal maternal anxiety differentially affects the risk of
LRTIs, especially bronchiolitis depending on their anatomic location. Increased glucocorticoid levels during fetal periods may affect the development and function of lung
319
320
during early life [43]. In addition, differences in defense mechanisms, depending on the
anatomy, and more severe characteristics in LRTIs than URTIs may account for the increased
321
322
323
risk of LRTIs [44, 45]. In addition, functional differences attributable to the genetic variants
in ROS–related genes may add an increased susceptibility to LRTIs, especially bronchiolitis
324
325
326
327
328
Potential limitations
This study has a few limitations. First, the sample size in this study is relatively small because this study is an ongoing prospective birth cohort study. Although the statistical power was weak to analyze the associations with respect to each type of LRTI except bronchiolitis due
329
330
331 to small sample size, this study implicates the importance of the effect of perinatal maternal anxiety on the occurrence of RTI during early life. Further large scale studies are needed to validate the results of this study.
Second, mechanisms underlying the additive effects between
332
333 perinatal anxiety and variants of antioxidant defense genes on the occurrence of LRTI, especially bronchiolitis were not explored. However, we tried to explain the underlying
334
335 pathophysiology based on the previously reported findings. Also, we analyzed only one single nucleotide polymorphism (SNP) in each gene; however, this selection was based on
336
337
338 previous studies demonstrating an association between SNPs and development of respiratory
Finally, we cannot exclude the effects of postnatal maternal anxiety on the
339 offspring’s health. However, after adjustment for the exposure to the postnatal maternal anxiety during their infants’ 1 st
year of life, exposure to the prenatal maternal stress was
Prenatal maternal anxiety & respiratory infection
13
340 associated with the increased risks of LRTIs. Finally, about 30% of the participants did not
341
342 report their anxiety status and was thus excluded from the analysis.
343
344
345
Conclusion
We suggest that exposure to perinatal maternal anxiety is a significant risk factor for the development of bronchiolitis in the first year of life. Also, this study implicates that variants
346
347
348 in antioxidant defense genes modulate the effect of in utero exposure to perinatal anxiety on infant susceptibility to bronchiolitis during critical periods. In view of the fact that bronchiolitis during early infancy are an economic and medical burden and are associated
349
350 with an increased risk of recurrent wheezing and asthma in later life, efforts to decrease perinatal anxiety may be helpful in preventing bronchiolitis during infancy, especially in
351 genetically susceptible infants.
Prenatal maternal anxiety & respiratory infection
1
352
353
354
355
Abbreviations:
CB : cord blood
CI : confidence intervals
COCOA : COhort for Childhood Origin of Asthma and allergic disease
356
357
GSTM1: glutathione S -transferase M1
GSTP1 : glutathione S -transferase P1
358
359
360
GSTT1 : glutathione S -transferase T1
LRTIs : lower respiratory tract infections
PCR : polymerase chain reaction
361
362
ROS : reactive oxygen species
RSV : respiratory syncytial virus
363
364
365
RTI : respiratory tract infection
SD : standard deviation
STAI : State-trait anxiety inventory
366
367
368
URTIs : upper respiratory tract infections
POTENTIAL CONFLICT OF INTERESTS TO COMPETING INTERESTS: The
369
370 authors have no conflicts of interest relevant to this article to disclose.
371
372
FINANCIAL DISCLOSURE : The authors have indicated that they have no financial relationships relevant to this article to disclose.
373
374
375
FUNDING: This research was supported by funds (2008-E33030-00, 2009-E33033-00.
2011-E33021-00, 2012-E33012-00) from Research of Korea Centers for Disease Control and
Prevention.
376
Prenatal maternal anxiety & respiratory infection
2
377
378
379
380
Role allocations
Eun Lee and Hyoung Yoon Chang contributed to the analysis and interpretation of data and drafting the manuscript.
381
382
Kyung-Sook Lee, Jinah Park, and In Ae Choi contributed to collection of data on perinatal maternal stress.
383
384
385
Dong In Suh, Kyung Won Kim, Youn Ho Shin, Kang Mo Ahn, Eun-Jin Kim, and Joo-Shil
Lee contributed to the construction of this cohort study and conducted the follow-up.
Ja-Young Kwon, Suk-Joo Choi, Kyung-Ju Lee, and Hye-Sung Won contributed to the
386
387 enrolment of pregnant women in the birth cohort study.
Mi-Jin Kang and Ho-Sung Yu performed the genetic studies and analyzed the data.
391
392
393
388
389
390
Song I Yang, Young-ho Jung, Hyung Young Kim, Ju-Hee Seo, Ji-Won Kwon, Byoung-Ju
Kim, Hyo-Bin Kim, So-Yeon Lee, and Katherine M. Keyes contributed to the thorough review of this manuscript and the acquisition of data.
Soo-Jong Hong and Yee-Jin Shin contributed to the conception of this study, its design, and interpretation of the data as co-corresponding authors.
394
395
ACKNOWLEDGMENTS
The authors thank Jung Yeon Shim, Woo Kyung Kim, Gwang Chen Jang, and Hyeon Jong
396
397
Yang for their valuable support during this study. In addition, the authors are grateful to the research nurses for their continuous collaboration over the years. We thank to Sung-Cheol
398
399
400
Yun for statistics advice.
401
Prenatal maternal anxiety & respiratory infection
3
402 References
413
414
415
5.
416
417
6.
418
419
420
7.
421
422
423
424
425
8.
9.
403
404
405
1.
2.
406
407
408
409
410
3.
411
412
4.
Hanson M, Gluckman P, Nutbeam D, Hearn J: Priority actions for the non-c ommunicable disease crisis . Lancet 2011, 378 :566-567.
Tegethoff M, Greene N, Olsen J, Schaffner E, Meinlschmidt G: Stress during pregnancy and offspring pediatric disease: A National Cohort Study . Enviro nmental health perspectives 2011, 119 :1647-1652.
Tregoning JS, Schwarze J: Respiratory viral infections in infants: causes, cli nical symptoms, virology, and immunology . Clinical microbiology reviews 201
0, 23 :74-98.
Beijers R, Jansen J, Riksen-Walraven M, de Weerth C: Maternal prenatal anx iety and stress predict infant illnesses and health complaints . Pediatrics 201
0, 126 :e401-409.
Merlot E, Couret D, Otten W: Prenatal stress, fetal imprinting and immunit y . Brain, behavior, and immunity 2008, 22 :42-51.
Zucchi FC, Yao Y, Ward ID, Ilnytskyy Y, Olson DM, Benzies K, Kovalchuk I,
Kovalchuk O, Metz GA: Maternal stress induces epigenetic signatures of p sychiatric and neurological diseases in the offspring . PloS one 2013, 8 :e5696
7.
Hosakote YM, Liu T, Castro SM, Garofalo RP, Casola A: Respiratory syncyti al virus induces oxidative stress by modulating antioxidant enzymes . Americ an journal of respiratory cell and molecular biology 2009, 41 :348-357.
Charil A, Laplante DP, Vaillancourt C, King S: Prenatal stress and brain dev elopment . Brain research reviews 2010, 65 :56-79.
Erni K, Shaqiri-Emini L, La Marca R, Zimmermann R, Ehlert U: Psychobiolo
Prenatal maternal anxiety & respiratory infection
4
426 gical effects of prenatal glucocorticoid exposure in 10-year-old-children . Fro
427
428 ntiers in psychiatry 2012, 3 :104.
10. Diz-Chaves Y, Pernia O, Carrero P, Garcia-Segura LM: Prenatal stress causes
429
430
431
alterations in the morphology of microglia and the inflammatory response
of the hippocampus of adult female mice . Journal of neuroinflammation 201
2, 9 :71.
432
433
434
11. Thompson LP, Al-Hasan Y: Impact of oxidative stress in fetal programming .
Journal of pregnancy 2012, 2012 :582748.
12. Hayes JD, Strange RC: Glutathione S-transferase polymorphisms and their b
435
436 iological consequences . Pharmacology 2000, 61 :154-166.
13. Kurt-Jones EA, Popova L, Kwinn L, Haynes LM, Jones LP, Tripp RA, Walsh
437
438
439
EE, Freeman MW, Golenbock DT, Anderson LJ ture immunology 2000, 1 :398-401.
et al : Pattern recognition rec eptors TLR4 and CD14 mediate response to respiratory syncytial virus . Na
440
441
14. Inoue Y, Shimojo N, Suzuki Y, Campos Alberto EJ, Yamaide A, Suzuki S, Ari ma T, Matsuura T, Tomiita M, Aoyagi M et al : CD14 -550 C/T, which is rel
442
443
444 ated to the serum level of soluble CD14, is associated with the developmen t of respiratory syncytial virus bronchiolitis in the Japanese population . Th e Journal of infectious diseases 2007, 195 :1618-1624.
445
446
15. Wiertsema SP, Khoo SK, Baynam G, Veenhoven RH, Laing IA, Zielhuis GA,
Rijkers GT, Goldblatt J, Lesouef PN, Sanders EA: Association of CD14 prom
447
448
449 oter polymorphism with otitis media and pneumococcal vaccine responses
Clinical and vaccine immunology : CVI 2006, 13 :892-897.
.
16. Kim HB, Ahn KM, Kim KW, Shin YH, Yu J, Seo JH, Kim HY, Kwon JW,
450 Kim BJ, Kwon JY et al : Cord blood cellular proliferative response as a pre
Prenatal maternal anxiety & respiratory infection
5
451
452
453
454
science 2012, 27
17. Shin YH, Choi SJ, Kim KW, Yu J, Ahn KM, Kim HY, Seo JH, Kwon JW, K im BJ, Kim HB
:1320-1326.
et al : Association between maternal characteristics and neo
455
456 dictive factor for atopic dermatitis at 12 months . Journal of Korean medical natal birth weight in a Korean population living in the Seoul metropolitan
area, Korea: a birth cohort study (COCOA) . Journal of Korean medical sc
457
458
459 ience 2013,
18. Shin YH, Yu J, Kim KW, Ahn K, Hong SA, Lee E, Yang SI, Jung YH, Kim
HY, Seo JH
28 :580-585.
et al : Association between cord blood 25-hydroxyvitamin D co
460
461 ncentrations and respiratory tract infections in the first 6 months of age i n a Korean population: a birth cohort study (COCOA) . Korean journal of
462
463
464 pediatrics 2013,
19. Yang HJ, Lee SY, Suh DI, Shin YH, Kim BJ, Seo JH, Chang HY, Kim KW,
Ahn K, Shin YJ
56 :439-445.
et al : The Cohort for Childhood Origin of Asthma and all
465
466
467 ergic diseases (COCOA) study: design, rationale and methods ary medicine 2014, 14 :109.
. BMC pulmon
20. Spielberger CD: Manual for the State-Trait Anxiety Inventory . Palo Alto, C
468
469
A: Consulting Psychologists Press; 1983.
21. Kim JT, Shin DK: A study based on the standardization of the STAI for K
470
471 orea . New Medical Journal 1978, 21 :69-75.
22. Hahn DW, Lee CH, Chon KK: Korean adaptation of Spielberger's STAI (K-
472
473
STAI) . Korean Journal of Health Psychology 1996, 1 :1-14.
23. Brasch-Andersen C, Christiansen L, Tan Q, Haagerup A, Vestbo J, Kruse TA:
474
475
Possible gene dosage effect of glutathione-S-transferases on atopic asthma: using real-time PCR for quantification of GSTM1 and GSTT1 gene copy n
Prenatal maternal anxiety & respiratory infection
6
476 umbers . Human mutation 2004, 24 :208-214.
477
478
479
24. Koch A, Molbak K, Homoe P, Sorensen P, Hjuler T, Olesen ME, Pejl J, Peder sen FK, Olsen OR, Melbye M: Risk factors for acute respiratory tract infec tions in young Greenlandic children . American journal of epidemiology 2003,
480
481
158 :374-384.
25. Jones LL, Hashim A, McKeever T, Cook DG, Britton J, Leonardi-Bee J: Pare
482
483
484 ntal and household smoking and the increased risk of bronchitis, bronchiol itis and other lower respiratory infections in infancy: systematic review an d meta-analysis . Respiratory research 2011, 12 :5.
485
486
26. Koopman LP, Smit HA, Heijnen ML, Wijga A, van Strien RT, Kerkhof M, Ge rritsen J, Brunekreef B, de Jongste JC, Neijens HJ: Respiratory infections in
487
488
489 infants: interaction of parental allergy, child care, and siblings-- The PIAM
A study . Pediatrics 2001, 108 :943-948.
27. Iuchi T, Akaike M, Mitsui T, Ohshima Y, Shintani Y, Azuma H, Matsumoto T
490
491
492
: Glucocorticoid excess induces superoxide production in vascular endotheli al cells and elicits vascular endothelial dysfunction . Circulation research 200
493
494
28. Gilliland FD, Rappaport EB, Berhane K, Islam T, Dubeau L, Gauderman WJ,
McConnell R: Effects of glutathione S-transferase P1, M1, and T1 on acute
495
496
3, 92 :81-87.
respiratory illness in school children ritical care medicine 2002, 166
.
:346-351.
American journal of respiratory and c
497
498
499
29. Rebbeck TR: Molecular epidemiology of the human glutathione S-transferas e genotypes GSTM1 and GSTT1 in cancer susceptibility . Cancer epidemiolo gy, biomarkers & prevention : a publication of the American Association for C
500 ancer Research, cosponsored by the American Society of Preventive Oncology 1
Prenatal maternal anxiety & respiratory infection
7
501
997, 6 :733-743.
502
503
504
30. Habdous M, Siest G, Herbeth B, Vincent-Viry M, Visvikis S: [Glutathione S-t ransferases genetic polymorphisms and human diseases: overview of epidem iological studies] . Annales de biologie clinique 2004, 62 :15-24.
505
506
31. Wright RJ: Moving towards making social toxins mainstream in children's e nvironmental health . Current opinion in pediatrics 2009, 21 :222-229.
507
508
509
32. Zafir A, Banu N: Modulation of in vivo oxidative status by exogenous corti costerone and restraint stress in rats . Stress 2009, 12 :167-177.
33. O'Connor TM, O'Halloran DJ, Shanahan F: The stress response and the hypo
510
511 thalamic-pituitary-adrenal axis: from molecule to melancholia ly journal of the Association of Physicians 2000, 93 :323-333.
. QJM : month
512
513
514
34. Nozik-Grayck E, Dieterle CS, Piantadosi CA, Enghild JJ, Oury TD: Secretion of extracellular superoxide dismutase in neonatal lungs
physiology Lung cellular and molecular physiology 2000,
. American journal of
279 :L977-984.
515
516
35. Kratschmar DV, Calabrese D, Walsh J, Lister A, Birk J, Appenzeller-Herzog C,
Moulin P, Goldring CE, Odermatt A: Suppression of the Nrf2-dependent ant
517
518
519 ioxidant response by glucocorticoids and 11beta-HSD1-mediated glucocortico id activation in hepatic cells . PloS one 2012, 7 :e36774.
36. Korytina GF, Yanbaeva DG, Babenkova LI, Etkina EI, Victorova TV: Genetic
520
521 polymorphisms in the cytochromes P-450 (1A1, 2E1), microsomal epoxide h ydrolase and glutathione S-transferase M1, T1, and P1 genes, and their rel
522
523
524 ationship with chronic bronchitis and relapsing pneumonia in children rnal of molecular medicine 2005, 83 :700-710.
. Jou
37. Cohen S, Janicki-Deverts D, Turner RB, Casselbrant ML, Li-Korotky HS, Epel
525 ES, Doyle WJ: Association between telomere length and experimentally in
Prenatal maternal anxiety & respiratory infection
8
526 duced upper respiratory viral infection in healthy adults . JAMA : the journ
527
528
529 al of the American Medical Association
38. Shalev I, Entringer S, Wadhwa PD, Wolkowitz OM, Puterman E, Lin J, Epel
ES:
2013, 309 :699-705.
Stress and telomere biology: a lifespan perspective . Psychoneuroendocrin
530
531 ology 2013, 38 :1835-1842.
39. Baldini M, Lohman IC, Halonen M, Erickson RP, Holt PG, Martinez FD: A P
532
533
534 olymorphism* in the 5' flanking region of the CD14 gene is associated wit h circulating soluble CD14 levels and with total serum immunoglobulin E
Am J Respir Cell Mol Biol 1999, 20 :976-983.
.
535
536
40. Kabesch M, Hasemann K, Schickinger V, Tzotcheva I, Bohnert A, Carr D, Bal dini M, Hackstein H, Leupold W, Weiland SK et al : A promoter polymorphis
537
538
539 m in the CD14 gene is associated with elevated levels of soluble CD14 but
not with IgE or atopic diseases . Allergy 2004, 59 :520-525.
41. Pincus-Knackstedt MK, Joachim RA, Blois SM, Douglas AJ, Orsal AS, Klapp
540
541
542
BF, Wahn U, Hamelmann E, Arck PC: Prenatal stress enhances susceptibility
of murine adult offspring toward airway inflammation . Journal of immunol ogy 2006, 177 :8484-8492.
543
544
42. Tuchscherer M, Kanitz E, Otten W, Tuchscherer A: Effects of prenatal stress on cellular and humoral immune responses in neonatal pigs . Veterinary imm
545
546 unology and immunopathology 2002, 86 :195-203.
43. Wright RJ: Perinatal stress and early life programming of lung structure a
547
548
549 nd function . Biological psychology
44. Kajekar R: Environmental factors and developmental outcomes in the lung .
Pharmacology & therapeutics
2010,
2007, 114
84 :46-56.
:129-145.
550 45. Bals R, Hiemstra PS: Innate immunity in the lung: how epithelial cells figh
551
552
553
Prenatal maternal anxiety & respiratory infection
9 t against respiratory pathogens . The European respiratory journal 2004, 23 :3
27-333.
Prenatal maternal anxiety & respiratory infection
10
Table I. Characteristics of study population and subjects not included in the current analysis
Covariates (mother)
Maternal age (years)
BMI (kg/m 2 )
Maternal educational level
Secondary school
College or University
Graduate school
Environmental tobacco exposure
History of any allergic disorder (AD, AR, Asthma)
Covariates (father)
History of any allergic disorder (AD, AR, Asthma)
Covariates (child)
Sex: Girl
Birth weight (g)
Season of birth
Spring
Summer
Autumn
Winter
Mode of delivery: Caesarean section
Gestational age (months)
Presence of siblings
Daycare attendance during the first year of life
Women included in this study n Mean ± SD or n (%)
440
32.5 ± 3.55
20.7 ± 2.67
31 (7.0%)
289 (65.7%)
120 (27.3%)
265 (60.8%)
124 (28.2%)
410
440
115 (26.1%)
217 (49.3%)
3143.9 ± 422.01
117 (26.6%)
117 (26.6%)
96 (21.8%)
110 (25.0%)
134 (34.4%)
39.2 ± 1.08
198 (45.0%)
105 (23.9%)
Exposure 440
STAI score
Physician diagnosed respiratory tract infection during the first year of life
41.0 ± 8.47 (20 – 71)
Upper respiratory tract infection
Lower respiratory tract infection
337 (76.6%)
65 (14.8%)
Bronchiolitis 48 (10.9%)
AD , atopic dermatitis; AR , allergic rhinitis; N/A, not applicable; STAI , state trait anxiety inventory
N/A
Women not include in this study n Mean ± SD or n (%)
193
32.4±3.45
20.7 ± 2.60
21 (7.3%)
209 (73.1%)
56 (19.6%)
160 (54.6%)
76 (30.4%)
193
65 (26.4%)
129 (44.2%)
3198.3 ± 395.43
42 (14.3%)
40 (13.7%)
139 (47.4%)
72 (24.6%)
100 (35.3%)
39.2±1.09
83 (43.0%)
43 (22.3%)
P value
0.736
0.754
0.060
0.131
0.537
0.651
0.173
0.153
<0.001
0.793
0.968
0.705
0.740
Prenatal maternal anxiety & respiratory infection
11
Table II. Odds ratio and 95% confidence intervals for perinatal anxiety predicting respiratory tract infection at age 1 year
Exposure Outcome Unadjusted Adjusted
*
OR
†
95% CI OR 95% CI
Upper RTI 1.04
1.31
‡
STAI (*SD) Lower RTI
Bronchiolitis 1.35
‡
(0.84–1.30)
(1.01–1.71)
1.10
1.35
‡
1.30
§
(0.87–1.39)
(1.01–1.78)
(1.00–1.81) (1.00–1.80)
CI , confidence intervals; OR , odds ratio; RTI , respiratory tract infection; SD , standard deviation; STAI , State trait anxiety inventory
* Adjusted for child’s sex, season of birth, maternal age, education level, exposure to tobacco smoking during the first year of life, history of maternal allergic diseases and history of any paternal allergic diseases (atopic dermatitis, allergic rhinitis, or asthma)
†
Logistic regression models were used to calculate OR and 95% CI.
‡ p -value < 0.05
§ p -value < 0.10
diagnosis diagnosis
(-) (+) diagnosis (-) diagnosis (+)
Prenatal maternal anxiety & respiratory infection
12
STAI
Table III. Interactions between maternal perinatal stress (STAI score) and GSTP1 (rs1695) polymorphism on the development of respiratory tract infection during the first year of life
Upper RTI
*
Lower RTI
†
Bronchiolitis
GSTP1 Upper RTI Upper RTI aOR
‡
Lower RTI Lower RTI aOR
‡
Bronchioli Bronchioliti aOR
‡
(95% CI) (95% CI) tis diagnosis s diagnosis
(+)
95% CI
(-)
138 9 1 low
(≤41) low
(≤41) high
(>41) high
AA
AG+GG
AA
AG+GG
36
17
31
13
111
43
90
53
1
1.10
(0.53-2.27)
1.25
(0.68-2.30)
1.91
133
51
101
52
14
9
20
14
1
1.66
(0.64-4.26)
1.99
(0.92-4.29)
2.61
(>41) (0.86-4.25) aOR , adjusted odds ratio; CI , confidence intervals; GSTP1: glutathione S -transferase P1;
(1.09-6.22)
52
106
54
8
15
12
2.14
(0.74-6.15)
2.07
(0.83-5.16)
3.36
(1.25-9.03)
Prenatal maternal anxiety & respiratory infection
13
RTI , respiratory tract infection; STAI , State trait anxiety inventory
*
Upper RTI includes common colds, sinusitis, otitis media, and croup.
†
Lower RTI includes pneumonia, tracheobronchitis, and bronchiolitis
‡ Adjusted for child’s sex, season of birth, maternal age, education level, prenatal exposure to tobacco smoking, history of any maternal allergic diseases and history of any paternal allergic diseases (atopic dermatitis, allergic rhinitis, or asthma)
diagnosis (-), diagnosis (+), n n diagnosis (-), diagnosis (+), n n
Prenatal maternal anxiety & respiratory infection
14
STAI
Table IV. Interactions between maternal perinatal stress (STAI score) and copy number variation of GSTT1 on the development of respiratory tract infection during the first year of life
Upper RTI
*
Lower RTI
†
Bronchiolitis
GSTT1 Upper RTI Upper RTI aOR
‡
Lower RTI Lower RTI aOR
‡
Bronchiolitis Bronchiolitis aOR
‡
(95% CI) (95% CI) diagnosis (-), diagnosis (+), n n
(95% CI) low
(≤41)
CNV≥1 low
(≤41)
CNV=0 high
(>41)
CNV≥1 high
(>41)
CNV=0
16
37
22
22
76
76
65
77
1
0.43
(0.21-0.88)
0.66
(0.30-1.45)
1.02
(0.46-2.26)
82
102
75
77
10
11
12
22
1
0.86
(0.33-2.21)
1.29
(0.50-3.33)
2.47
(1.04-5.89)
85
104
79
80 aOR , adjusted odds ratio; CI , confidence intervals; CNV , copy number variation; GSTT1, glutathione S -transferase T1;
RTI , respiratory tract infection; STAI , State trait anxiety inventory
7
9
8
19
1
0.97
(0.33-2.83)
1.13
(0.37-3.34)
2.79
(1.05-7.43)
Prenatal maternal anxiety & respiratory infection
15
*
Upper RTI includes common colds, sinusitis, otitis media, and croup.
†
Lower RTI includes pneumonia, tracheobronchitis, and bronchiolitis
‡ Adjusted for child’s sex, season of birth, maternal age, education level, prenatal exposure to tobacco smoking, history of any maternal allergic diseases and history of any paternal allergic diseases (atopic dermatitis, allergic rhinitis, or asthma)
Prenatal maternal anxiety & respiratory infection
16
Figure Legends
Figure.
Relationship between perinatal maternal anxiety levels and predicted probability of bronchiolitis at 1 year of age.
Prenatal maternal anxiety & respiratory infection
17
Supplementary figure.
Effect of GSTP1 (rs1695) polymorphisms on respiratory tract infection according to perinatal maternal anxiety levels. (A) The risk of upper RTIs during the first year of life. (B) The risk of lower RTIs during the first year of life. (C) The risk of bronchiolitis during the first year of life.
STAI, state trait anxiety inventory
Prenatal maternal anxiety & respiratory infection
18
Supplementary table I . Interactions between maternal perinatal stress (STAI score) and copy number variations of GSTM1 on the development of respiratory tract infection during the first year of life
Upper RTI *
STAI
Upper RTI Upper RTI
GSTM1 diagnosis (-) diagnosis (+) low (≤41)
CNV≥1 21 77 low (≤41) CNV=0 32 76 aOR
‡
(95% CI)
1
0.68
(0.35-1.34) high (>41) high (>41)
CNV≥1
CNV=0
24
20
55
87
0.81
(0.38-1.73)
1.43
(0.68-3.01)
Lower RTI†
Lower RTI Lower RTI diagnosis (-) diagnosis (+)
91 7
93
65
87
15
14
20 aOR
‡
(95% CI)
1
1.75
(0.66-4.66)
2.95
(1.06-8.17)
2.60
(1.01-6.66)
Bronchiolitis
Bronchiolitis Bronchiolitis diagnosis (-) diagnosis (+)
92 6
97
69
90 aOR , adjusted odds ratio; CI , confidence intervals; CNV , copy number variation; GSTM1, glutathione S -transferase M1;
11
10
17
RTI , respiratory tract infection; STAI , State trait anxiety inventory aOR
‡
(95% CI)
1
1.35
(0.46-3.97)
2.02
(0.65-6.25)
2.35
(0.86-6.47)
*Upper RTI includes common colds, sinusitis, otitis media, and croup.
†
Lower RTI includes pneumonia, tracheobronchitis, and bronchiolitis
† Lower RTI includes pneumonia, tracheobronchitis, and bronchiolitis
Prenatal maternal anxiety & respiratory infection
19
‡
Adjusted for child’s sex, season of birth, maternal age, education level, prenatal exposure to tobacco smoking, history of any maternal allergic diseases and history of any paternal allergic diseases (atopic dermatitis, allergic rhinitis, or asthma)
STAI CD14 diagnosis
(-), n
Diagnosis
(+), n diagnosis
(-), n diagnosis
(+), n
Prenatal maternal anxiety & respiratory infection
20
Supplementary table II.
Interactions between STAI score and CD14 (rs2569190) polymorphism on the development of respiratory tract infection during the first year of life
Upper RTI
*
Lower RTI
†
Bronchiolitis
Upper RTI Upper RTI aOR
‡
Lower RTI Lower RTI aOR
‡
Bronchiolitis Bronchiolitis aOR
‡
(95% CI) (95% CI) diagnosis
(-), n diagnosis (+), n
(95% CI) low
(≤41)
TT low
(≤41)
TC+CC high
(>41)
TT
21
31
13
43
110
44
1
1.89
(0.93-3.83)
2.51
60
123
46
4
18
11
1
2.22
(0.69-7.14)
4.60
60
128
47 high
(>41)
TC+CC 31 96
(1.01-6.24)
1.90
(0.91-3.94)
105 22
(1.29-16.41)
3.01
(0.94-9.70)
110 aOR , adjusted odds ratio; CI , confidence intervals; RTI , respiratory tract infection; STAI , State trait anxiety inventory
*
Upper RTI includes common colds, sinusitis, otitis media, and croup.
4
13
10
17
1
1.58
(0.47-5.31)
4.31
(1.17-15.79)
2.11
(0.63-7.04)
Prenatal maternal anxiety & respiratory infection
21
†
Lower RTI includes pneumonia, tracheobronchitis, and bronchiolitis
‡ Adjusted for child’s sex, season of birth, maternal age, education level, prenatal exposure to tobacco smoking, history of any maternal allergic diseases and history of any paternal allergic diseases (atopic dermatitis, allergic rhinitis, or asthma)