Gastroesophageal Reflux Epidemiology and the Rationale for
advertisement

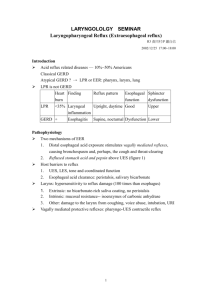
Appendix: Gastroesophageal Reflux Epidemiology and the Rationale for Physician Counseling Changing Impact of Gastroesophageal Reflux in Medical and Otolaryngology Practice A1 There has been a significantly increased interest in the literature regarding gastroesophageal reflux disease (GERD) and laryngopharyngeal reflux (LPR) over the last two decades. This interest seems to be in response to an apparent increasing number of patients with GERD and LPR, although there are no studies in the literature that adequately document the rate of rise. Epidemiology research is often limited by the absence of large-scale databases that track individual subjects over time, so studies on the subject of GERD usually focus on specific populations for a given period of time. The goals of this appendix are to summarize the current understanding of the epidemiology of GERD, and to review the rationale for physician counseling of lifestyle modification to patients with GERD and LPR. As lifestyle modification may play an integral role in the treatment of disease, then it has the potential to affect the overall prevalence of disease. The epidemiology of GERD has been studied using a number of different approaches. Kennedy and Jones (A1) presented a postal survey of 3179 adults in the United Kingdom, in which 28.7% of the population reported heartburn and acid regurgitation symptoms. Less than 25% of subjects with these symptoms presented for medical evaluation and treatment. In a similar study, Louis et al. (A2) reported their interview study involving 2000 adults in Belgium. In this project, 28.4% of the respondents reported symptoms of heartburn at some point of the preceding year, and 56% of these individuals sought medical advice. In the United States, Locke et al. (A3) found 20% of their questionnaire sample to have weekly heartburn and almost 60% with occasional symptoms. A2 Haque et al. (A4) conducted a similar survey with a postal questionnaire. Of the 778 respondents, there was significant overlap between the 30% with reported symptoms attributable to reflux, and the 34.2% with dyspepsia over the preceding year, with an overall “prevalence” of 45.2%. This study further suggests that the symptomatic overlap may in fact be a similarity in pathophysiology of the disease. The “global definition” of dyspepsia suggests that this term is a “variable mix of upper gastrointestinal symptoms” (A5). Endoscopic evaluation of patients with reflux symptoms would be expected to most informative of the state of disease, however this is a relatively unsensitive finding in refluxs disease. Voutilainen et al. (A6) evaluated 1128 consecutive patients referred for endoscopy due to dyspeptic and reflux symptoms. For the purposes of this study GERD was defined as the presence of symptoms for more than six months, accounting for 238 patients. Of these, overall esophagoscopy was normal in 33%, but 85% of patients under 50 years old had a negative exam. This suggests that the disease is often symptomatic with negative objective findings, comparable to dyspepsia. Johanson (A7) reported a summary of epidemiological studies that suggests a prevalence of occasional or monthly heartburn at 21-58%, and daily heartburn at 4-7%. However, the studies referenced were published over a fairly broad range from1982-1997. Perhaps more informative, the incidence of GERD was reported in one study published in 1969 at 0.086%/year (A8), which is starkly smaller than that reported in 1992 at 6%/year (A9). A3 This suggests a significant rise in the incidence of disease over the time period 19691992, although there are substantial limitations in such a meta-analysis. These limitations include comparing studies with different recruitment criteria, and from different study populations or databases. Sonnenberg (A10) analyzed the rate of all physician contacts for esophagitis in 1985 with the use of the National Ambulatory Medical Care Survey (NAMCS) and the National Disease and Therapeutic Index (NDTI). These databases do not report prevalence or incidence of GERD/esophagitis in the general population since the data is limited to physician contacts and some people with disease may not present for treatment. However, there is significant value in these results when considering the impact of GERD/esophagitis on physician practice. The NAMCS figure for total contacts with esophagitis was 797/100,000 population in the United States (0.797%), and the NDTI figure was 1,246/100,000 (1.246%). Incidence may be inferred from the NDTI as less than 20% of physician contacts were first time visits, placing the figure at 0.249/year in 1985. This crude estimation figure is consistent with other reported trends of 0.086%/year in 1969 (A8) and 6%/year in 1992 (A9). One additional way of determining a rising rate of disease is to study the rate of complications from the disease. Panos et al. (A11) documented a rising death rate from non-malignant disease of the esophagus (esophagitis and esophageal perforation) between 1968 and 1991. An association between GERD and esophageal adenocarcinoma has also been noted. Pera et al. (A12) demonstrated increasing incidence of A4 adenocarcinoma of the esophagus, from approximately 0.2/100,000/year in 1974-1979 to 1/100,000/year in 1985-1989. However, these trends may have been impacted by the increased availability and accuracy of non-invasive diagnostic techniques. While GERD seems to be on the rise in developed countries, it does not appear to be as prominent in developing countries (A13, A14). This raises the possibility of lifestyle and diet as an etiology of disease in industrialized nations. GERD is a disease that is significantly lifestyle driven, although there is certainly physiologic and anatomic predisposition. It is therefore straightforward that lifestyle modification should be integral to the care of the reflux patient. Counseling that patients receive on triggers of GERD usually include avoidance of caffeine, alcohol, tobacco, spicy foods, fatty foods and mints. Individual patients may experience exacerbation of their disease with other food products (such as wheat), and they may be more sensitive to food and liquids with a lower pH (such as citrus and tomato-based products). While there is generally a widespread consensus that diet and behavior modification is helpful in the treatment of patients with gastroesophageal reflux, objective studies have been based on small numbers of subjects that do not meet strict statistical significance (A15). Further controversy is sparked by a study involving one-hundred consecutive patients undergoing pH probe monitoring, in which lifestyle alteration did not show significant effect on gastroesophageal reflux (A16). A5 Coffee is a classic example of a beverage that has caffeine (considered to exacerbate predisposition to reflux) as well as triggering increased awareness of heartburn. In one study Pehl et al. (A17) investigated the effects of caffeine and coffee on a reflux population using 3-hour pH probe monitoring. Following the ingestion of caffeinated coffee the median time of pH < 4 was 18%, compared to 3% for subjects receiving decaffeinated coffee. In a prior study, Wendl et al. (A18) demonstrated that caffeinated coffee induced significant reflux, however, subjects did not develop notable reflux in response to caffeinated tea or caffeinated water. Alcohol is known to affect lower esophageal sphincter pressure and esophageal motility (A19), so one would expect that reducing alcohol intake would affect severity and frequency of GERD. There is also considerable evidence to support tobacco cessation as a lifestyle modification for reflux since smoking reduces lower esophageal sphincter pressure and prolongs acid exposure due to decreased salivation (A20). However, there are conflicting reports regarding actual changes seen on pH-probe monitoring in subjects while smoking (A21, A22, A23). While intake of fatty foods may exacerbate GERD by slowing digestion, the effect of fat on postprandial gastroesophageal reflux is still controvertial. Colombo et al. (A24) used 6-hour pH monitoring in thirteen healthy volunteers to monitor changes after high fat, balanced fat and balanced low calorie meals. In their study, the balanced low calorie meal resulted in fewer episodes of reflux and less time under pH 4 than the balanced calorie or high fat meals, suggesting that the caloric load of meals is more critical than fat content A6 in affecting gastroesophageal reflux. These data supports empiric observation of the effects of low calorie diet on GERD patients (A25). However, Pehl et al. (A26) were not able to demonstrate any significantly different effects of low calorie meals compared to high calorie meals on reflux time and lower esophageal sphincter tone. In another study by this group, Pehl et al. (A27) were not able to demonstrate a significant difference in pH or lower esophageal sphincter pressure in a group of twelve volunteers after eating low versus high fat meals. This suggests that the volume of the meal may have more of an effect on reflux than the calorie content. Lifestyle modification alone may only dampen symptoms of the disease, although patient reduction of these triggers is well known to control flare-ups of symptoms. However, lifestyle changes are presently considered to be adjuncts to medical management of GERD with pharmacotherapy (A28). It is still not clear whether lifestyle modification alone has the potential to substantially affect overall epidemiologic trends in GERD and LPR. A7 References A1. Kennedy T, Jones R, “The prevalence of gastro-oesophageal reflux symptoms in a UK population and the consultation behaviour of patients with these symptoms,” Aliment Pharmacol Ther 2000; 14: 1589-1594. A2. Louis E, DeLooze D, Deprez P et al, “Heartburn in Belgium: Prevalence, impact on daily life, and utilization of medical resources,” Euro J Gastroenterol Hepatol 2002; 14: 279-284. A3. Locke GR III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ III, “Prevalence and clinical spectrum of gastroesophageal reflux: A population-based study in Olmsted County, Minnesota,” Gastroenterol 1997; 112: 1448-1456. A4. Haque M, Wyeth JW, Stace NH, Talley NJ, Green R, “Prevalence, severity and associated features of gastro-oesophageal reflux and dyspepsia: a populationbased study,” New Zeland Med J 2000; 113: 178-81. A5. Malfertheiner P, “Current concepts in dyspepsia: A world perspective,” Eur J Gastroenterol Hepatol 1999; 11(suppl 1): S25-S29. A6. Voutilainen M, Sipponen P, Mecklin J-P, Juhola M, Farkkila M, “Gastroesophageal reflux disease: Prevalence, clinical, endoscopic and A8 histopathological findings in 1,128 consecutive patients referred for endoscopy due to dyspeptic and reflux symptoms,” Digestion 2000; 61: 6-13. A7. Johanson JF, “Epidemiology of esophageal and supraesophageal reflux injuries,” Am J Med 2000; 108 (4A): 99S-103S. A8. Brunnen PL, Kannody AM, Needham CD, “Severe peptic esophagitis,” Gut 1969; 10: 831-7. A9. Talley NJ, Zinsmeister AR, Schleck CD, Melton HILJ, “Dyspepsia and dyspepsia subgroups: A population based study,” Gastroenterology 1992; 102: 1259-1268. A10. Sonnenberg A. Esophageal diseases. In: Everhart JE, ed. Digestive Diseases in the United States: Epidemiology and Impact. US Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Disease. NIH publication no. 94-1447. Washington, DC: US Government Printing Office, 1994: 300-355. A11. Panos MZ, Walt RP, Stevenson C, Langman MJS, “Rising death rate from nonmalignant disease of the oesophagus (NMOD) in England and Wales,” Gut 1995; 36: 488-491. A9 A12. Pera M, Cameron AJ, Trastek VF, Carpenter HA, Zinsmeister AR, “Incresing incidence of adenocarcinoma of the esophagus and esophagogastric junction,” Gastroenterology 1993; 104: 510-513. A13. Osatakul S, Sriplung H. Puetpaiboon A, Junjana CO, Chamnongpakdi S, “Prevalence and natural course ofgastroesophageal reflux symptoms: a 1-year cohort study in Thai infants,” J Ped Gastroenterol Nutrition 2002; 34: 63-7. A14. Segal I, “The gastro-oesophageal reflux disease complex in sub-Saharan Africa,” Euro J Cancer Prevention 2001; 10: 209-212. A15. Meining A, Classen M, “The role of diet and lifestyle measures in the pathogenesis and treatment of gastroesophageal reflux disease,” Am J Gastroenterol 2000; 95: 2692-7. A16. Lim PL, Gibbons MJ, Crawford EJ, Watson RG, Johnston BT, “The effect of lifestyle changes on results of 24-h ambulatory oesophageal pH monitoring,” Eur J Gastroenterol Hepatol 2000; 12: 655-6. A17. Pehl C, Pfeiffer A, Wendl B, Kaess H, “The effect decaffeination of coffee on gastro-oesophageal reflux in patients with reflux disease,” Alimentary Pharmacology & Therapeutics 1997; 11: 483-6. A10 A18. Wendl B, Pfeiffer A, Pehl C, Schmidt T, Kaess H, “Effect of decaffeination of coffee or tea on gastro-oesophageal reflux,” Alimentary Pharmacology & Therapeutics 1994; 8: 283-7. A19. Bujanda L, “The effects of alcohol consumption upon the gastrointestinal tract,” Am J Gastroenterol 2000; 95: 3374-82. A20. Pandolfino JE, Kahrilas PJ, “Smoking and gastro-oesophageal reflux disease,” Eur J Gastroenterol Hepatol 2000; 12: 837-42. A21. Smit CF, Cooper MP, van Leeuwen JA, Schoots IG, Stanojcic LD, “Effect of cigarette smoking on gastropharyngeal and gastroesophageal reflux,” Ann Otol Rhinol Laryngol 2001; 110: 190-3. A22. Kadakia SC, Kikendall JW, Maydonovitch C, Johnson LF, “Effect of cigarette smoking on gastroesophageal reflux measurend by 24-h ambulatory esophageal pH monitoring,” Am J Gastroenterol 1995; 90: 1785-90. A23. Pehl C, Pfeiffer A, Wendl B, Nagy I, Kaess H, “Effect of smoking on the results of esophageal pH measurement in clinical routine,” J Clin Gastroenterol 1997; 25: 503-6. A11 A24. Colombo P, Mangano M, Bianchi PA, Penagini R, “Effect of calories and fat on postprandial gastro-oesophageal reflux,” Scan J Gastroenterol 2002; 37: 3-5. A25. Yancy WS Jr, Provenzale D, Westman EC, “Improvement of gastroesophageal reflux disease after initiation of a low-carbohydrate diet: five brief case reports,” Alternative Therapies in Health & Medicine 2001; 7: 116-120. A26. Pehl C, Pfeiffer A, Waizenhoefer A, Wendl B, Schepp W, “Effect of caloric density of a meal on lower oesophageal sphincter motility and gastro-oesophageal reflux in healthy subjects,” Alimentary Pharmacology & Therapeutics 2001; 15: 233-9. A27. Pehl C, Waizenhoefer A, Wendl B, Schmidt T, Schepp W, Pfeiffer A, “Effect of low and high fat meals on lower esophageal sphincter motility and gastroesophageal reflux in healthy subjects,” Am J Gastroenterol 1999; 94: 11926. A28. Katz PO, “Optimizing medical therapy for gastroesophageal reflux disease: state of the art,” Reviews in Gastroenterological Disorders 2003; 3: 59-69. A12