Fibroscan Business Case
advertisement

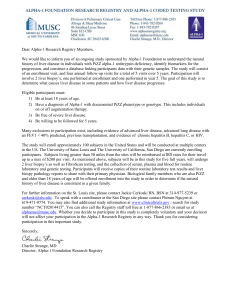
1 Report Title: Business case for the purchase of a new fibroscan machine To be presented by: Executive Summary: Liver disease in the UK is growing at an alarming rate and there is an increasing need for early diagnosis of disease and the assessment of fibrosis to identify those patients with significant liver damage who will benefit from the early implementation of disease management programs which reduce emergency admissions and improve mortality. Average age of death from liver disease in the UK is 59 years; at XXX within alcohol related liver death (2011) the average age was 57 years. Key documents have been published (NICE guidance for increased testing for hepatitis B and hepatitis C, appendix 1, NHS outcomes framework 2012/13, Caring for people with liver disease: Nurse competencies, appendix 2, or are currently in draft, due for publication, (NICE Liver related quality improvement measures and quality standards, NHS specialist commissioning for hepatobiliary and pancreas services, NCEPOD report: Alcohol related liver disease) which have significant implications for the continued increased need and therefore access to the specialist services in the liver unit at XXX and care of patients with liver disease throughout XXX and XXXX London. fibroscanning is now the first recommended assessment for patients with liver disease and a fundamental service providing immediate and risk free assessment of a patients liver fibrosis being used with other investigations. Fibroscanning is a service now being sort by a considerable number of health providers, local General Practitioners. Due to the limited number of machines and trained scan staff with liver knowledge this places XXX as one of the largest providers of this service in the country and the main provider in XXXX London. As the largest provider of liver services in North West London, the business case below sets out the reasoning and need to continue to support and expand the Fibroscan service and the Nursing specialist resources for the improvement of patient care, outcomes, experience and mortality and better management of the direct costs associated with this increasing burden which is currently £0.5 billion per annum to the NHS and rising at 10% a year. XXX experienced a XX.XX% increase in inpatient liver disease related admissions in the year 20112012 which is significantly greater than the year on year forecasted increase of 10% (British Association of Liver Disease). If this is repeated for 2011 – 2012, admissions to the three hospital sites for 2012 will reach XXXX. At of the end of March 2012; XXXX inpatient admissions for a liver ICD-10 code had been recorded in ICH giving a renewed forecast for the trust of XXXX admissions which is an increase of XX.X% on 2011. Key Issues for Discussion: To approve the one off expenditure of £XX,XXX for the purchase of a new fibroscan machine 2 To approve the annual cost of £X,XXX for on-going servicing and maintenance of the machine To assist in providing Fibroscan services, educating and assisting in the earlier recognition and management of Liver disease in the community, ward and outpatient setting. Link to the Trust’s Principal Objectives: 1. 2. 3. 4. Provide the highest quality of healthcare to the communities we serve improving patient safely and satisfaction. Work together for the achievement of outstanding results in all our activities Conduct world-class research and deliver benefits of innovation to our patients and population. Respect our patients and colleagues Business case for the purchase of a Fibroscan machine XXXX 2013 Background Liver disease is a growing epidemic in current healthcare and is now the fifth largest cause of mortality in the UK, with an average age at death of 59 years. Liver disease is the only one of the major diseases on the increase and as such poses a significant risk to future healthcare burden and mortality (Appendix 3). It is forecast to cost the NHS in excess of £1 billion by 2015 (BASL, 2004, 2009). The three largest contributors to this burden are: Viral hepatitis Alcohol Obesity (including non-alcoholic fatty liver disease) Clinical outcomes for liver disease are greatly improved if the condition is detected early and appropriate treatment courses begun. The most effective and convenient way of assessing the condition of a patient’s liver is via a fibroscan, and XXXXXXXXXXXX NHS Trust is currently providing this service out of the XXXXXX XXXXXX at the XXXXXXX site. The assessment of disease stage is a key component of all patient assessments in hepatology. Disease stage which generally equates to the degree of fibrosis (between normal and cirrhosis) can only be measured using investigations such as fibroscan and liver biopsy. International guidelines require staging prior to treatment for both hepatitis B virus infection and hepatitis C virus infection. Both sets of guidelines accept fibroscan as an acceptable assessment of fibrosis stage. A position paper on Fibroscan will be published next year with the approval of all International Liver Societies supporting the use of fibroscan as an assessment tool across a wide range of liver diseases. This business case proposes the purchase of an additional Fibroscan machine in order to increase the number and speed with which patients can have their livers assessed. In the care setting, the only alternative to Fibroscanning is to undertake a liver biopsy which may be painful and conveys a small but significant risk or morbidity and mortality (1/10000). Liver biopsy requires a day case admission causing significant anxiety and inconvenience to the patient. As fibroscan is a fibrosis assessment tool, not a diagnostic one. As the rate of liver disease continues to increase (UK forecast is 10% per year) and within XXXX this was demonstrated with a XX.XX% increase in liver related inpatient admissions for the year 2010 – 2011. The requirement for liver biopsy to diagnose the underlying cause will therefore not diminish and is demonstrated in figure: 1. the need once diagnosed to assess fibrosis and rate of progression will increase substantially year on year 3 Figure 1: XXXXX Unit daycase liver biopsy Liver Biopsy activity 2007 - 2012 400 350 107 98 54 111 300 110 250 94 # 200 287 150 283 266 249 224 100 168 50 0 2007 2008 2009 2010 2011 Dec-17 Year Done DNA Fibroscanning is a 20 minute non-invasive, painless assessment that furthermore does not require an inpatient admission and gives ‘real time’ results. The patients’ liver may be assessed in ambulatory care rather than daycase, and the availability of portable machines increases the flexibility for this service to be provided in the most convenient location for patients such as lager GP practices or within the inpatient ward environment. Early assessment of and diagnosis of liver disease and complex multisystem disease are key outcomes set out in the hepatobiliary NHS specialist commissioning framework being published in 2013 in order to treat earlier and affect mortality rates. As well as improving physician’s knowledge, improved disease management planning, reducing anxiety and delivering on outcome PHQ14: assisting people with long-term conditions to feel independent and in control of their condition it improves patient experience. The fibroscan can ensure that all current access and many outcome targets are met and minimising the number of required bed days for the Trust, at present. Currently there is an inability to assist in meeting targets set such as PHQ15: Unplanned hospitalisation for chronic ambulatory care sensitive conditions (adults) in the 2012/13 operating framework as we are unable to assess the level of liver fibrosis in those with hepatitis B with or without Delta who could be managed in ambulatory care if cirrhosis was detected earlier an management plans in place to reduce non-elective admissions for complications of cirrhosis. Current wait is XX weeks for a fibroscan. An increase in Fibroscanning represents a core part of the Hepatology strategy to increase access for early assessment of liver damage and activity. It is also significant in developing better integrated care pathways with Clinical Commissioning Groups (CCGs) following increased NICE guidance to test for and detect more viral hepatitis. Patient experience Fibroscans improve patient experience, both when in the care setting and also from a much broader life experience perspective. From a quality of life perspective, early identification of liver disease through use of Fibroscanning enables the condition to be assessed and managed much earlier in the process, reducing the likelihood and severity of complications and mortality and greatly improving their management and patient’s quality of life. This is a Key outcome in the NHS specialist commissioning proposals for Hepatobiliary and pancreas services. 4 Proposal It is proposed that XXXX purchase another Fibroscan with immediate effect. However, in May the research machine was transferred to XXXXXX. In order to mitigate against the loss of one machine we successfully increased the number of cases between Jan and May 2012 by 32% to reduce any waiting list before the second machine was lost. However, despite further increases in the Fibroscan activity with increased sessions in the remaining machine the waiting list continues to grow as demand significantly exceeds capacity (42% more scans have been performed in 2012 than in 2011), figure 2. Figure 2: XXXXX Unit fibroscan list year on year Fibroscan activity 2008 - 2012 1400 68 1200 124 1000 279 0 129 0 800 165 # 176 600 130 0 400 200 744 166 0 99 35 526 483 38 205 104 0 Years Attended DNA Biospy paired Planned Links with Hepatology, CPG1 and Trust strategy Expanding provision of Fibroscanning is an integral part of the Hepatology Strategic Plan. As well as bringing short-term benefits to XXXX by increasing activity to the levels agreed in the contract with commissioners, which has been overachieved with the increased extra clinical sessions being made available when trained staff can be released for other clinical duties, improving the waiting time, it will likely yield strategic benefits and despite this has a XX week wait for a scan. These benefits are in two principle ways: An increase in referrals or expansion in market share, owing to a developing community presence; and a reduction in inpatient bed days and Length of Stay relating to liver disease, with earlier detection of severe disease, appropriate management can be implemented reducing non-elective admissions and early mortality as a result. The current age of death for a liver related ICD-10 code is XX years within XXX. The service is now receiving referrals for fibroscan directly from GP’s and has been approached by the XXXX XXXXX Hospital to provide a fibroscan service. None of this can be performed in a timely manner if at all with the current level of equipment or specifically trained staff. The only reduction in the list will take place for the servicing or calibration of the probe which is now required 4 times per year rather than the 2 previously. This is done on the number of procedures undertaken by the individual probe. Should the one remaining probe be damaged which is a 5 significant risk with the increased number of procedures the service will cease until repair can be undertaken (this requires collection and removal of the probe to Paris). Current position: Current sessions per week X Number of scans performed per week: XX Current referral rate 75-95 per month XXX patients currently on the waiting list Next available appointment for a fibroscan XXXXXXX, Delayed follow up in Consultant outpatient awaiting results Increased scans offered in 2012 up 42% on 2011. Fibroscanning is aligned to the current Ambulatory Care agenda and can lead to a reduction in inpatient stays of <1 day as early detection of disease can improve management and address the increase in non-elective admissions for complications of severe liver damage being seen in XXX. Finally, increasing Fibroscanning contributes to two of the Trust’s strategic objectives for the current year: 1. Provide the Highest Quality of Healthcare to the Communities we Serve 2. Provide World-leading Specialist Care in our Chosen Fields It also has potential to deliver against a third Trust strategic objective, Conduct World-class Research and Deliver the Benefits of Innovation to our Patients and Population, as more patients will be exposed to the possibilities afforded them by participation in clinical trials. Clinical guidelines International Hepatology and HIV-coinfected Guidelines advocate the use of fibroscan as the first line of assessment of liver damage removing the need to liver biopsy where a diagnosis is known and cirrhosis is not evident. Access implications Current waiting times for Fibroscanning are (XX weeks the next available appointment is the XXXXXXX). The national standard for diagnostic procedures is six weeks from referral. Furthermore as the fibroscans are now an essential component in the assessment of patients prior to antiviral therapy the XX week waits frequently compromises the 18 week target between referral and the initiation of treatment. There are currently XXX patients are on the waiting list for a fibroscan and we are accumulating new referrals at a rate of 75 – 95 per month. The referral rate is expected to increase substantially over the next few months as the service is opened up to other hospitals and general practitioners. The purchase of an additional Fibroscan and CNS will enable an additional XX procedures per week (comprising X sessions and XX scans per week) and access for inpatients to fibroscan for earlier diagnosis of advancing fibrosis and improved care planning. It is therefore expected that within three months of purchase waiting list may be reduced to a fortnight. Increase capacity V Replacement Increasing fibroscan capacity with the current system would require immediate reconfiguration and likely addition to the current nursing establishment to maintain current PCT agreed activity in this and other specialist activity and require the training of new staff to perform these roles. The increased demand placed on the current system places it at risk resulting in increased calibration needs which closes the list for one week for each calibration. Additional equipment enables appropriate planning for calibration without the loss of any clinical activity. The most common cause of chronic liver disease is non-alcoholic liver disease (NAFLD) with approximately 20% - 30% of the population with 10% of children aged 10 estimated to have NAFLD this creates a need to be able to assess the damage being done to the liver. The current fibroscan equipment whilst able to identify liver stiffness is not able to provide a quantifiable assessment of liver steatosis and a liver biopsy is still required for many. This advancement is available with the updated fibroscan. 6 The addition of the portable system allows development of the service into the community areas and difficult to reach patient groups providing equity of access to liver assessment which is currently not available. This is prevented by the nature of liver biopsy and the size and sensitivity of the main fibroscan system. Workforce implications Purchase of an additional Fibroscan has some immediate workforce implications, as this maintaining of a second afternoon with 2 trained staff (X clinical sessions) is a level of service that has not previously been provided by the Trust and is not currently built into job plans. An additional Clinical Nurse Specialist in Hepatology (CNS) will need to be recruited with immediate effect and trained if not already as the referral rates continue to increase and the XX% increase of inpatient liver related admissions. This will enable XXX to deliver the predicted rise in community and outreach work to other NHS trusts and address the inpatient care of liver disease patients. It also allows XXX to implement and demonstrates compliance with NICE guidance for HCV and HBV published in December 2012; address the nursing care and education requirements in the inpatient setting of an increasing population of complex patients being admitted to all of XXX main sites in line with the pending specialist commissioning of complicated HCV and cirrhosis requirements. The provision of extra sessions and increased fibroscan capacity is currently severely limited by the workload of the trained scan nurse specialists as they are also trained and provide the venessection service, staff the liver biopsy day case ward, pre assessment clinic for liver biopsy cases and coordinate and support the specialist cirrhosis and transplant assessment clinic and the clinical research activity. The Senior Nurse ability to provide additional fibroscan sessions is limited by the large clinical research portfolio and study coordinator responsibilities performed in the same area, staff and resource management and internal and external education and other job description work associated demands. Demand There is currently an expediential increase in demand for the fibroscan service and improved care that patients diagnosed with liver disease obtain as this can alter mortality in this area, The awareness of liver disease relate issues and health implications are now acknowledged by the Department of Health and local community health areas. Increased demand for the Fibroscan service is evidenced by the current waiting list of XXX patients despite an increase in scans offered of 42% on last year which has been sustained since May 2012. In addition, the Heptaology team have begun engagement with local CCGs over supporting them to identify patients on their register with liver disease. For example, XXXX and XXXX have expressed an interest in procuring community Fibroscanning services and have requested a business case be submitted. In addition, informal discussions with other local Acute Trusts have highlighted the demand for this service, and willingness to fund it as a more cost effective alternative to biopsies where a diagnosis is known (approximately £xxx/procedure versus £xxx/procedure respectively). There are only XX fibroscan machines in various centres around the UK and so there is huge potential to grow market share. Cost An estimate has been provided from Echosens, the manufacturers of the Fibroscanners, which is only valid if the order is placed and processed before the XXXXXX The cost is broken down as follows: Non-recurrent costs: (agreed in December 2011) Fibroscan Portable Fibroscan XL patient probe (for patients with BMI >30) Paediatric probe TOTAL £ £ £ £ Recurrent costs: 12-month maintenance agreement for probe 12-month maintenance agreement for Fibroscan 12-month maintenance agreement for Portable Fibroscan £ £ £ 7 TOTAL £ Note: First year’s recurrent costs included in purchase price Income The Fibroscan has potential to garner additional income; however, it is recognised that this will either need to go through the ‘counting and coding’ process or will need to be factored into any negotiations with other Trusts (where referrals are from Secondary or Tertiary Care). Such proposals are likely to be accepted, as they represent a saving to the CCGs of £XXX per patient per procedure (compared to biopsies) and reduce the long-term cost of this cohort of patients with chronic conditions. The immediate financial benefits of the Fibroscan are: Ensuring that activity levels agreed for XXXXX, based on performance in XXXXX, will be met Avoid financial penalties for non-delivery of six-week diagnostic pathway The New CNS post in being able to deliver increased community services and Fibroscan clinics will directly generate income for XXX, the position allows patients within the inpatient environment greater access evidence based practice, improved clinical care and access to clinical research opportunities. Associated benefits Essential for developing close working relationships with CCGs Expands patient cohort for whom participation in research trials may be appropriate, delivering the XXXXX XXXXX vision and increasing research income Delivers better integrated care with long-term benefits to the Trust’s non-elective inpatient admissions Aligns with model for Ambulatory Care to reduce admissions with Length of Stay of <1 day Complies with the key outcomes proposed in the NHS specialist commissioning for Hepatobiliary and pancreas services. Provides evidence of compliance with NICE guidance and DH and RCN nurse competencies in the improving of outcomes for patients with liver disease. Places XXX as the largest single provider of Fibroscan services in the NHS Risk The risk of not investing in or purchasing new fibroscanning equipment will Prevent XXX from developing or marinating its majority market share in fibroscanning services Result in XXX needing to purchase this service form another provider to meet the increasing demand for access to liver care XXX will not be able to provide access to liver assessments for the area or funding PCT’s XXX will fail to meet locally and nationally set targets for the care and management of people with liver disease XXX will fail to meet equity and diversity targets set for accessing marginalised populations, many of whom have multiple causes of liver disease and have difficulty in engaging with secondary care areas. Recommendations It is recommended that with immediate effect the purchase of new fibroscanning equipment is arranged and processed through procurement to be able to prevent the extra £11,000 cost to the CPG which will come into effect on the 1/4/13 That engagement with and an assessment is made within the local care commissioning groups for the need/requirement of a community liver/fibroscan service which can identify those patients who can be managed and cared for within the community setting and those who need secondary care management for more complex and sever disease. 8 Appendix 3. Time to act: Rate of liver related deaths under 65 years compared to other causes related to base rates in 1970: BASL (2009)