Administrative Office St. Joseph`s Hospital Site, L301
advertisement

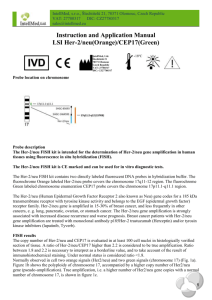
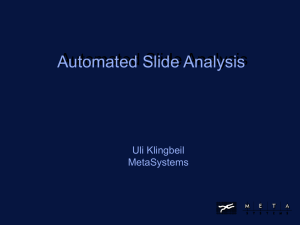
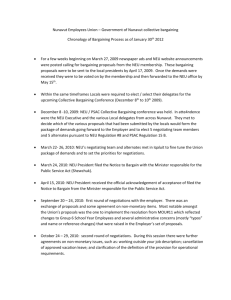
Administrative Office St. Joseph's Hospital Site, L301-10 50 Charlton Avenue East HAMILTON, Ontario, CANADA L8N 4A6 PHONE: (905) 521-6141 FAX: (905) 521-6142 http://www.fhs.mcmaster.ca/hrlmp/ Issue No. 51 QUARTERLY NEWSLETTER June, 2000 HER-2/neu (C-erbB-2) TEST IN BREAST CANCER BACKGROUND: HER-2/neu is a proto-oncogene localized to chromosome 17 that encodes a transmembrane tyrosine kinase human epidermal growth factor receptor protein. Overexpression of HER-2/neu protein or HER-2/neu gene amplification is seen in 10-33% of breast cancers1,2 and at a lower frequency in a number of other solid tumor types. In common with other members of epidermal growth factor family, the HER-2/neu protein has three domains: an extracellular receptor binding site, a lipophilic transmembrane segment, and an intracellular area with tyrosine kinase activity. Ligand binding to the receptor complex on the cell surface leads to activation of intrinsic protein tyrosine kinase activity. This triggers a cascade of events leading to gene activation resulting in mitogenic stimulation. The HER-2/neu receptor, therefore, plays a key role in cellular growth. HER-2/neu AS A PROGNOSTIC AND PREDICTIVE FACTOR IN CANCER: It is generally accepted that there is a significant correlation between a positive HER-2/neu status and an adverse clinical outcome in node positive tumours.3,4 There is still controversy concerning its prognostic significance in node negative patients.5,6 The clinical studies have shown an apparent resistance of tumours with a positive HER-2/neu status to hormone therapy alone7,8 and a strong interaction between HER-2/neu overexpression and chemosensitivity to some chemotherapy regimes.9,10 CANCER THERAPY: HERCEPTIN (Trastuzumab) is a recombinant DNA-derived humanized monoclonal antibody that selectively targets the extracellular domain of HER-2/neu protein. This antiHER-2/neu monoclonal antibody therapy results in alterations of signaling and therefore reduced tumour growth. Apart from this action, Herceptin is also known to potentiate the activity of chemotherapy agent such as paclitaxel. In Ontario, Herceptin is approved for the treatment of patients with metastatic breast cancer whose tumours overexpress HER-2/neu. Herceptin therapy should only be initiated under the supervision of a physician experienced in the treatment of cancer patients. TESTING HER-2/neu STATUS: Immunohistochemistry (IHC), fluorescent in situ hybridization (FISH), and quantitative PCR are powerful assays that are useful for detection of HER-2/neu overexpression and amplification respectively in formalin fixed paraffin embedded tissue samples from primary breast cancers, lymph nodes, or metastases. The following figures show negative and positive HER-2/neu using IHC (DAKO A0485). As per Cancer Care Ontario guidelines, HER-2/neu testing should be undertaken in laboratories supporting regional cancer centers or institutions providing medical oncology practice. These laboratories must have an established immunohistochemistry department with sufficient volume to maintain technical/professional knowledge and skill. The laboratories must confirm indeterminate results using either FISH or quantitative PCR. NEGATIVE POSITIVE REFERENCES: 1. Ali IU, Campbell G, Lidereau R, Callahan R. Lack of evidence for the prognostic significance of cerbB-2 amplification in human breast carcinoma. Oncogene Res 1988;3:139-46. 2. Berger MS, Locker GW, Saurer S, Gullick WJ, Waterfield MD, Groner B, et al. Correlation of cerbB-2 gene amplification and protein expression in human breast carcinoma with nodal status and nuclear grading. Cancer Res 1988;48:1238-43. 3. Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: 4. 5. 6. 7. 8. 9. 10. correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987;235:177-82. Ross JS, Fletcher JA. The HER-2/neu oncogene in breast cancer: prognostic factor, predictive factor, and target for therapy. Stem Cells 1998;16:413-28. Andrulis IL, Bull SB, Blackstein ME, Sutherland D, Mak C, Sidlofsy S, et al. Neu/erbB-2 amplification identifies a poor prognosis group of women with node-negative breast cancer. J Clin Oncol 1998;16:1340-9. Clark G. Should selection of adjuvant chemotherapy for patients with breast cancer be based on erb-2 status? N Natl Cancer Inst 1998;90:1320-21. Bianco AR, DeLaurentis M, Carlomagno C, et al. 20 year update of the Naples gun trial of adjuvant breast cancer therapy: evidence of interaction between c-erbB2 expression and tamoxifen efficacy. Proc Am Soc Clin Oncol 1998;17:97a. Newby JC, Johnston SR, Smith IE, Dowsett M. Expression of epidermal growth factor receptor and c-erbB2. Clin Cancer Res 1997;3:1643-51. Paik S, Bryant J, Park C, Fisher B, Tan-Chiu E, Hyams D, Fisher ER, Lippman ME, Wickerham DL, Wolmark N. erbB-2 and response to doxorubicin in patients with axillary lymph node-positive, hormone receptor-negative breast cancer. J Natl Cancer Inst 1998;90:1361-70. Ravdin PM, Green S, Albain KS, et al. Initial report of the SWOG biological correlation study of cerb2 expression as a predictor of outcome in a trial comparing adjuvant CAFT with tamoxifen (T) alone [abstract]. Proc Am Soc Clin Oncol 1998;17:97a. Dr. L. Elavathil, Pathologist Dr. B. Carter, Pathologist Hamilton Regional Laboratory Medicine Program Henderson General Site, Hamilton Health Sciences Corporation