Systems Approach to XML based Competency Definition
advertisement

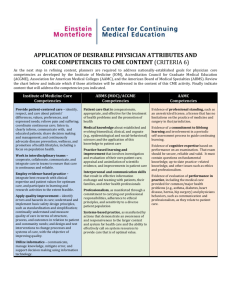
XML-oriented Competency Definition: Systems Approach Vladimir Goodkovsky, PhD University of Virginia vladimir@virgina.edu Introduction Study of existing materials about Competency demonstrates diversity of different views and lack of a single order or system. That is what we are trying to address and hopefully to compensate in this paper: bring the order into the chaos and propose a system for Competency Definition. We feel that systems approach is the best for this purpose. Systems Principles we used Principles Consider any object at least on 3 levels: super-system, system and sub-systems. Differentiate external behavior and internal functioning of the system Split a complex system into simpler subsystems, select one of interest and replace others with their actions on selected subsystem and its reactions. Recommendations Consider Competence on 5 levels: Patient Model Doctors Model Learner Model Instructor Model Medical Education Model Consider Competence as an internal factor of a doctor/learner, which defines his/her external behavior. Consider Competence with its connection to tasks to perform and expected performance. Super-System: (Medical) Education In (Medical) Education there are the following needs: To define learning objectives based upon professional competencies; To collect/design assessments for assessing achievement of the objectives by learners; To collect/design learning activities for achieving desired learning objectives; To evaluate cross consistency and sufficiency, reveal and fill insufficiencies. To sequence available learning activities and assessments for each particular learner to fill the gaps in objectives achievements by the most effective way. To meet these educational needs it is necessary: To understand professional competencies To represent learning objectives based upon professional competencies; To understand relations between available assessments and learning objectives they cover; To understand relations between available learning activities and learning objectives they help to achieve. Medical Educational super-system includes at least 4 systems: 1. Patient 2. Doctor 3. Learner 4. Instructor Below we propose a unified framework for each subsystem, which is necessary for overall definition of Competency from different perspectives. All about competency is presented below in BLUE color. 1. Patient Model in Medical Domain. (Related to VPWG, CWG) Declarative Representation of a (passive) Patient External (stimulus-effect, action-reaction) Representation Stimuli: (exam, test, lab, treatment, drug,…) (controllable mostly) Stimulus1: Stimulus ID Stimulus Description Expected Effects/Symptoms/Findings (measurable) Positive Effects/Symptoms/Findings: Effect/Symptom/Findings 1, … Negative Effects/Symptoms/Findings: (optional) Effect/Symptom/Finding 1, … Sub-Stimuli (optional) … Stimuli Interrelations Internal (health) Representation Int.Systems: Int.System1: Int.System ID Int.System description Int.System States: (not measurable, yet assessable) Normal States: State 1 … Pathological States: State 1 … Sub-Int.Systems (optional) … Int.Systems Interrelations Preferences, Allergies, … “External X Internal” Relations: “Stimuli X Int.SystemStates” Relation: “Stimulus1 X Int.SystemStates” Relation (describes coverage of Int.SystemStates by Stimulus1) “Stimulus1 positive effect X Int.SystemStates” (identifies some normal Int.SystemStates justified by positive effect of Stimulus1) “Stimulus1 negative effect X Int.SystemStates” (identifies some pathological Int.SystemStates blamed by negative effect of Stimulus1) “Stimuli X Int.SystemState1” Relation (identifies some Stimuli, which cover Int.SystemState1) “Stimuli X Preferences/Allergies” Relation (identifies some Stimuli, which are acceptable by the patient) Procedural Representation of a (passive) Patient: Involuntary changes a current state of his/her Int.Systems Accepts Stimuli (exam, test, labs, treatments, operations, drugs,…) Produces Effects (results, symptoms, finding,…) This Model represents a simple (yet extensible in width and depth) root framework for specifying an essential part of Medical Competencies (Knowledge of a Patient) at any level of detail. 2. Doctor Model in Medical Domain (Related to PPWG, CWG) Declarative Representation of a Doctor Activity External (stimulus-effect) Representation Tasks: (controllable somehow) Task1: Task ID What is desired? Desired Situation in Medical domain of activity (e.g. desired state of patient’s Int.Systems) What is available? Current Situation in (Medical) domain of activity (e.g. Patient’s raw Data, recognized symptoms) Resources to use: Reference Materials Time Tools Labs Other Doctors What is expected performance? (measurable somehow) Standard performances: Standard Performance 1, … Typical Fault performances: (optional) Fault 1 … Sub-Tasks (optional) … Tasks Interrelations Internal (mental resource) Representation D.Competencies: (includes the Patient Model) D.Competence1: (a specific part of the Patient Model) Identifier Type: Ability Knowledge Skill Attitude Undefined Description State = Achieved (not measurable, yet assessable) Sub-D.Competencies (optional) … D.Competencies Interrelations Preferences “External X Internal” Relations: “Tasks X D.Competencies” Relation “Task1 X D.Competencies” Relation (describes coverage of some D.Competencies by Task1) “Task1 standard performance X D.Competencies (identifies some D.Competencies justified by standard performance of Task1) “Task1 fault performance X D.Competencies (identifies some D.Competencies blamed by fault performance of Task1) “Tasks X D.Competence1” Relation (identifies some tasks, which activate D.Competence1) “Tasks X Preferences” Relation Procedural Representation of a Doctor Activity Prepares for the Service Reeds History of Present Illness, recognizes symptoms, findings Reeds Past Medical History, recognizes symptoms, findings Reeds Social History, recognizes symptoms, findings Reeds Family History, recognizes symptoms, findings Provides the Service Reviews Int.Systems, recognizes symptoms, findings Performs Physical Examination, recognizes symptoms, findings Assigns Labs and reeds results, recognizes symptoms, findings Assigns Radiology and reeds results, recognizes symptoms, findings Assigns Procedures Makes diagnosing decision Plans Therapy Follows up 3. Learner Model in Educational Domain. (Related to MWG, PCLWG, CWG) Declarative Representation of a Learner Activity External (stimulus-effect) Representation Tasks: (controllable somehow) Task1: Task ID What is desired? Desired Situation in domain of activity What is available? Current Situation in domain of activity Resources to use: Learning Materials Self-test items Time Tools, The Virtual Patient Simulated Patients, Standardized Pateint, Other Learners, Doctors, Instructors What is expected performance? (measurable somehow) Standard performances: Standard Performance 1, … Typical Fault performances: (optional) Fault 1 … Sub-Tasks (optional) … Tasks Interrelations Internal (mental resource) Representation L.Competencies: () (L.Competencies may be defined on the basis of D.Competencies and include a subjective Patient Model) L.Competence1: (e.g., a specific part of subjective Patient Model) Identifier Type: Ability Knowledge Skill Attitude Open Description Mastery States: (not measurable, yet assessable somehow) Ground Zero Supplied Achieved Sub-L.Competencies (optional) … L.Competencies Interrelations Preferences “External X Internal” Relations: “Tasks X L.Competencies” Relation “Task1 X L.Competencies” Relation (describes coverage of some L.Competencies by Task1) “Task1 standard performance X L.Competencies (identifies some L.Competencies justified by standard performance of Task1) “Task1 fault performance X L.Competencies (identifies some L.Competencies blamed by fault performance of Task1) “Tasks X L.Competence1” Relation (identifies some tasks, which activate L.Competence1) “Tasks X Preferences” Relation Procedural Representation of a Learner Activity Learns to prepare for a Service: Learns to reed History of Present Illness, recognize symptoms, findings Learns to reed Past Medical History, recognize symptoms, findings Learns to reed Social History, recognize symptoms, findings Learns to reed Family History, recognize symptoms, findings Learns to provide a Service: Learns to review Int.Systems, recognize symptoms, findings Learns to perform Physical Examination, recognize symptoms, findings Learns to assign Labs and reed results, recognize symptoms, findings Learns to assign Radiology and reed results, recognize symptoms, findings Learns to assigns Procedures Learns to make diagnosing decisions Learns to plan Therapy Learns to follow up 4. Instructor Model in Educational Domain (Related to LO, PCLWG) Declarative Representation of a Instructor Activity External (stimulus-effect) Representation Tasks: (controllable somehow) Task1: Task ID What is desired? Learning Objectives = some D.Competencies What is available? Current Achievements = L.Competencies Resources to use: Learning Materials Assessments, Test Items Time Tools Patients, Doctors, Learners, Instructors What is expected performance? (measurable somehow) Standard performances: Standard Performance 1, Sequence of Learning Materials and test Items … Typical Fault performances: (optional) Fault 1: Wrong Sequence of Learning Materials and test Items … Sub-Tasks (optional) … Tasks Interrelations Internal (mental) Representation T.Competencies: (not measurable, yet assessable somehow) T.Competence1: Identifier Type: Ability Knowledge Skill Attitude Open Description State = Achieved Sub-T.Competencies (optional) … T.Competencies Interrelations Preferences “External X Internal” Relations: “Tasks X T.Competencies” Relation “Task1 X T.Competencies” Relation (describes coverage of some T.Competencies by Task1) “Task1 standard performance X T.Competencies (identifies some T.Competencies justified by standard performance of Task1) “Task1 fault performance X T.Competencies (identifies some T.Competencies blamed by fault performance of Task1) “Tasks X T.Competence1” Relation (identifies some tasks, which activate T.Competence1) “Tasks X Preferences” Relation Procedural Representation of a Instructor Activity Prepares for teaching Studies his/her learner and builds the learner model Collects available learning materials Collects available testing items Accepts/formulates learning objectives Defines a learning strategy Connects all of it together Checks consistency and sufficiency Realizes teaching Selects a mode: presenting or testing Selects next learning material or test item depending of the mode selected. Recognizes learner’s performance Updates learner Model Checks achievement of learning objectives Justification: Provided Models represent a systems context for cross-definition of Competencies. In such a context, competencies may be defined as 1. something that includes the Patient Model; 2. the internal representation of Doctor’s ability to perform external (medical) tasks. 3. the internal representation of Learner’s ability to perform external (educational) tasks. This definition can be easily detailed by extending the model. For example, competencies can be defined as good and not so good. Standard performance of the tasks can justify good competencies. Fault performances can blame not so good competencies. 4. Possible base line and learning objectives of the instructor. Competencies can be decomposed into any number of sub-competencies, each of which can be decomposed into sub-sub-competencies and so on. Competencies may have relations. For example: prerequisite relations, analogy, … But what is the most important for education; the models establish relations required for performing educational tasks by instructor (human or machine). Particularly: It defines learning objectives based upon Competencies; It establishes relations between available tasks (such as assessments) and learning objectives they cover; It establishes relations between available tasks (such as learning activities) and learning objectives they help to achieve. It means that these models are able to support solution of main educational tasks. They are extendable in width (you can add new sibling elements) and in depth (you can add new child elements). The tasks and competencies are also recursively extendable in depth, which means that you can add sub-tasks to any task and sub-competencies to any competence. The models are ready for XML notation. Vocabulary adjustment may be required.