form
advertisement

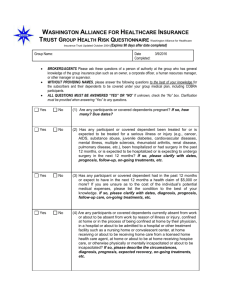
Date: ___________________ Interprofessional Diabetes Foot Ulcer Team 310 Wellington Road, London N6C 4P4 Initial Patient History Form Patient name:______________________________________ Date of birth:_________________ SURGICAL HISTORY MEDICAL PROBLEM LIST Diabetes Type: Type 1 Type 2 Diabetes Duration:___________________________ HbA1c: ____________date: _______________ Diabetes control 7% requires improvement Diabetes Complications: Renal impairment Hypertension Retinopathy History of previous foot ulcers Dyslipidemia Stroke Peripheral Arterial Disease Cardiovascular Disease Obesity Mental/Affective Disorder MEDICATIONS Other medical problems: Obesity Mental/Affective Disorder History of falls. Details: ___________________________________ Other: FAMILY HISTORY: SOCIAL HISTORY Marital Status: Married Common-law Widowed Separated/Divorced Same-sex partner Single Living Situation: Lives alone partner/spouse roommate dependent children adult children parents/in-laws other___________________________ Best source of support re Illness: spouse/partner child parent sibling friend other_______________ Support Person’s Response to Illness: understands their illness understands their need for medication understands their need for treatment encourages their coping efforts provides practical help sometimes tries to take over management understands chronic-nature of illness supports and listens to challenges SOCIAL HABITS: Alcohol: No Yes glasses/wk__________________ Smoker? Never Yes: Amount __ppd x __ yrs QUIT______ Drugs: 9th July 2010 ULCER WOUND HISTORY (duration, recurrence, infection, hospitaln) DATE OF ONSET/DURATION: TREATMENTS: CURRENT TREATMENTS: PAST Response to Treatments (e.g., wearing new footwear occasionally, stopped smoking entirely, using meds regularly) : Barriers to Treatment (e.g., depression, family problems, difficulty remembering to check feet) Weight bearing activity level problematic : No Yes Work:______________________________________________ Exercise:___________________________________________ Social activities:______________________________________ Page 1 of 1