Sample Request Form and MTA - Birmingham Women`s Hospital
advertisement

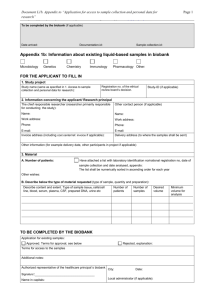
Central England Haemato-oncology Research Biobank Mike Griffiths Director of CEHRB West Midlands Regional Genetics Laboratory Birmingham Women's Hospital Edgbaston, Birmingham, B15 2TG Tel: 0121 627 2710 Fax: 0121 627 2711 email: mike.griffiths@bwhct.nhs.uk Sally Jeffries Manager of CEHRB West Midlands Regional Genetics Laboratory Birmingham Women's Hospital Edgbaston, Birmingham, B15 2TG Tel: 0121 627 2710 Fax: 0121 627 2711 email: sally.jeffries@bwhct.nhs.uk Sample Request Form CONFIDENTIAL Prior to completing an application it is recommended that the researcher e-mails both the director and manager of the bank to ensure that the samples that they would like to request are available, see sample requirement details below. Please complete in block capitals and send a copy each to the Director and the Manager of CEHRB. Applications must be submitted as an electronic document. The committee will consider the impact and feasibility of the proposed study on the use of bank resources. We aim to review all applications within a month of receipt. REQUESTED BY (Full Name, Title): . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . POSITION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . INSTITUTION ADDRESS (FOR SAMPLES): ...................................................................................... ...................................................................................... ...................................................................................... Tel No: . . . . . . . . . . . . . . . . . . . Fax No:. . . . . . . . . . . . . . . . . e-mail:. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . FULL TITLE OF RESEARCH PROJECT: ...................................................................................... ...................................................................................... ATTACH A DISCRIPTION/SUMMARY OF ITS PURPOSE (Sufficient information should be provided to enable the review panel to determine the scientific validity of the study. If your project has been reviewed as part of a grant application, you may supply a copy of the scientific part of that grant application. Please also include whether the project will require the use of animals and give details): ...................................................................................... NAME OF THE CHIEF INVESTIGATOR: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . FUNDING SOUCE: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DURATION OF FUNDING: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Central England Haemato-Oncology Research BioBank (Version 1.2, 25/05/2010) The format and wording of the MTA was produced by the Wales Cancer Bank (Version 2.3, 05/11/07) TO COVER THE COSTS OF BANKING WE MAY CHARGE FOR THE SAMPLES PROVIDED. ARE YOU WILLING TO COVER THE COST OF BANKING TO ANY SAMPLES PROVIDED TO YOU? DETAILS OF COST CAN BE PROVIDED ON REQUEST. ...................................................................................... ...................................................................................... THE LOCATION OF THE RESEARCH: ...................................................................................... ...................................................................................... COLLABORATORS WITHIN AND OUTSIDE THE ABOVE INSTITUTE: ...................................................................................... ...................................................................................... HAS ETHICAL PERMISSION BEEN SORT OR OBTAINED FOR THIS PROJECT? PLEASE GIVE DETAILS, INCLUDE MREC/LREC NUMBER FOR THE STUDY AND PROVIDE A COPY OF THE APPROVAL LETTER : ...................................................................................... ...................................................................................... ................................................................................ NAME TO WHOM THE SAMPLES SHOULD BE ADDRESSED AT THE ABOVE INSTITUTE: ............................................................ TISSUE WILL ONLY BE SUPPLIED WHEN ETHICAL APPROVAL HAS BEEN GIVEN. A COPY OF THE APPROVAL LETTER SHOULD BE SENT TO THE CEHRB MANAGER. RESEARCHERS WILL BE EXPECTED TO COVER THE COST OF TRANSPORTATION OF THE SAMPLES. DETAILED TISSUE REQUIREMENTS: Must include: Sample type required: whole blood/bone marrow, plasma, viable cells, fixed cells, DNA, RNA, cDNA etc. Disease type and stage. Number and amount of each sample required. Anonymised samples are supplied with a minimum data set of gender, age and disease type. Please include details of any other data that you would like on these samples. Central England Haemato-Oncology Research BioBank (Version 1.2, 25/05/2010) The format and wording of the MTA was produced by the Wales Cancer Bank (Version 2.3, 05/11/07) Central England Haemato-oncology Research BioBank AGREEMENT FOR USE OF TISSUE: Project: The recipient/investigator agrees that the tissues provided by the Central England Haemato-Oncology Research BioBank (CEHRB) will be used only for the purposes specified in this application. The recipient agrees not to attempt to obtain information identifying the individuals providing tissues to the CEHRB. The recipient agrees that it shall not sell any portion of the tissues provided by the CEHRB, or products directly extracted from these tissues (e.g. protein, mRNA or DNA). The recipient also agrees that they shall not transfer tissue (or any portion thereof) supplied by the CEHRB to third parties without the prior written permission of the CEHRB. Any subsequent transfer that may be made to other parties, with prior agreement from CEHRB, will require signature of this agreement between the final recipients of the material and the CEHRB. The recipient agrees to return any surplus tissue not used in the research to CEHRB so that the tissue may be made available to other research groups. With written permission from CEHRB any surplus tissue may be stored by the recipient for future research if agreed by CEHRB and the tissue is held in an institute that holds a HTA research license. The recipient understands that while the CEHRB attempts to avoid providing tissues that are contaminated with highly infectious agents such as hepatitis and HIV, all tissues should be handled as if potentially infectious. The individuals who have supplied tissue to the CEHRB have not agreed to have clinical tests performed on this tissue (e.g. for the presence of infective agents such as hepatitis), therefore, the recipient agrees not to perform such tests on the tissues supplied by the CEHRB. The recipient acknowledges that the institution where the tissue will be used follows Human Tissue Authority or appropriate local regulations if outside England, Wales and Northern Ireland, for handling human specimens and will instruct their staff to abide by those rules. The recipient further agrees to assume all responsibility for informing and training personnel in the dangers and procedures for safe handling of human tissues. Tissues are provided as a service to the research community without warranty of merchantability or fitness for a particular purpose or any other warranty, express or implied. The CEHRB accepts no responsibility for any injury (including death) damages or loss that may arise either directly or indirectly from their use. The recipient agrees to acknowledge the contributions of the Central England Haemato-Oncology Research BioBank in all publications resulting from the use of these tissues and provide a copy of the research paper to the CEHRB upon publication. If after 12 months from the release of the tissue the BioBank has not received any communication regarding the project then the researcher will be contacted to provide feedback on the use of the tissue and progress of the study. If no report is received then the Biobank shall prohibit the release of any further tissue samples to the researcher. The institution agrees to assume all risks and responsibility in connection with the receipt, handling, storage and use of issues from the CEHRB. It further agrees to indemnify and hold harmless CEHRB from any claims costs, damages or expenses resulting from the use of the tissues provided by CEHRB. The undersigned warrant that they have authority to execute this agreement on behalf of the recipient institution. BY MY SIGNATURE I AGREE TO THE TERMS SET FORTH IN THE ABOVE AGREEMENT _____________________________ ____________________________________________ Typed Name of Principal Investigator Institution/department _______________________________ Signature of Principal Investigator _______________________________ Date UPON RECEIPT OF THESE SIGNED UNDERSTANDINGS AND THE INFORMATION REQUESTED ABOVE, THE CENTRAL ENGLAND HAEMATO-ONCOLOGY RESEARCH BIOBANK WILL CONSIDER THIS REQUEST. Specific questions about your application should be directed to Sally Jeffries, CEHRB Manager, West Midlands Regional Genetics Laboratory, Birmingham Women’s Hospital NHS Foundation Trust, Edgbaston, Birmingham, B15 2TG. Tel: +44 (0)121 6272710, Fax: +44 (0)121 6272711, Email: sally.jeffries@bwhct.nhs.uk Central England Haemato-Oncology Research BioBank (Version 1.2, 25/05/2010) The format and wording of the MTA was produced by the Wales Cancer Bank (Version 2.3, 05/11/07)