Sulfasalazine tablets for inflammatory arthritis in adults
advertisement

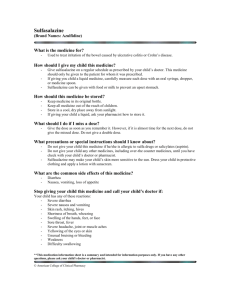
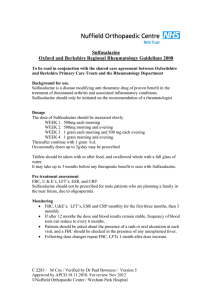
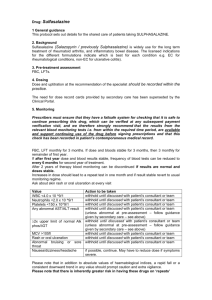
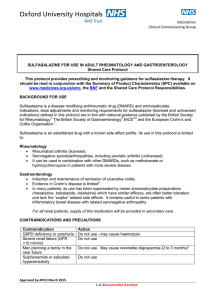
Shared Care Guideline Sulfasalazine tablets For the treatment of: Inflammatory arthritis in adults ( 16 years old) For the latest information on interactions and adverse affects, always consult the latest version of the Summary of Product Characteristics (SmPC), which can be found at: www.medicines.org.uk These guidelines are based on the monitoring criteria of the British Society of Rheumatology, published in the following reference: Chakravarty, K., McDonald, H., Pullar, T. et al. (2008) BSR/BHPR guideline for diseasemodifying anti-rheumatic drug (DMARD) therapy in consultation with the British Association of Dermatologists. Rheumatology 47(6), 924-925. Authors: Dr Kelsey M Jordan (Consultant Rheumatologist, BSUH NHS Trust) Dr Stewart E Glaspole (Pharmacist, BSUH NHS Trust/BHCPCT) SSZ SCG Document status Final/Draft: Final 13 Jan 2009 Date of next review if final: 13 Jan 2010 Page 1 of 8 Drug Name Sulfasalazine 500 mg enteric coated tablets. Indications for use within the protocol Inflammatory arthritis diagnosed by a Rheumatologist, usually supported by indices of inflammation. Duration – most drugs require up to 3 to 4 months trial to assess efficacy (including the time required for dose stabilisation). Therapy is continued providing the drug is working and that any side effects are tolerated by the patient. Relapse is common after withdrawal of therapy. Background Sulfasalazine is used as a disease modifying agent to induce and maintain remission in several types of rheumatic disease. It can reduce inflammation and affect the immune system and is therefore used for a number of other conditions. Pharmacology Sulfasalazine is cleaved by intestinal bacteria to equal amounts of 5-ASA and sulfapyridine. Sulfapyridine is thought to be the more active element in rheumatoid arthritis. Plausable explanations for sulfasalazine’s action center on inhibition of bacterial gut antigens and a general anti-inflammatory effect caused by 5-ASA. Dosage and administration 500 mg/day orally increasing by 500mg weekly to 2.0–3.0 g/day. Occasionally doses above 3.0 g/day are prescribed. Contraindications to use Sulfasalazine is contra-indicated in patients: Hypersensitive to sulphonamides/co-trimoxazole Hypersensitive to aspirin. Cautions Glucose-6-phosphate dehydrogenase deficiency: May cause haemolysis. Seek specialist advice. Renal impairment (moderate - GFR 10-20ml/min): May cause significant crystalluria and must ensure high fluid intake. In case of severe renal failure (GFR <10ml/min) do not use. Slow–acetylators of the drug: May cause drug-induced lupus-like syndrome. It is not necessary to assess acetylator phenotype. May impair folate absorption. SSZ SCG Document status Final/Draft: Final 13 Jan 2009 Date of next review if final: 13 Jan 2010 Page 2 of 8 Monitoring The British Society for Rheumatology (BSR) recommends precise monitoring to be carried out for this drug. The requirements are summarised in the following table. a. Pre-treatment assessment FBC, U&E, LFTs These tests will be carried out by the initiating hospital specialist. b. Ongoing Monitoring FBC and LFTs (including AST/ALT) monthly for the first 3 months and 3 monthly thereafter If, following the first year, dose and blood results have been stable, frequency of blood tests can be reduced to every 6 months for the second year of treatment Thereafter, monitoring of blood for toxicity may be discarded Patients should be asked about the presence of rash or oral ulceration at each visit. Repeat FBC, LFT one month after dose increases. c. Following dose changes Additional monitoring not required but useful ESR and/or CRP every three months. Actions to be taken 9 WBC<3.5x10 /l Withhold until discussed with specialist team. 9 Neutrophils<2.0x10 /l Withhold until discussed with specialist team. 9 Platelets<150x10 /l AST, ALT>twice reference range Withhold until discussed with specialist team. upper limit of Withhold until discussed with specialist team. MCV>105 fl Check B12, folate and TSH. If abnormal, treat any underlying abnormality. If normal, discuss with the specialist team. Nausea/dizziness/headache If possible continue, may have to reduce dose or stop if symptoms severe. Discuss with specialist team Abnormal bruising or severe Check FBC immediately and withhold until results available. Discuss with the specialist team, if necessary. sore throat Unexplained acute widespread rash Withhold seek urgent specialist (preferably dermatological) advice. Oral ulceration Withhold until discussed with specialist team. SSZ SCG Document status Final/Draft: Final 13 Jan 2009 Date of next review if final: 13 Jan 2010 Page 3 of 8 Undesirable effects The main adverse effects include: Permanent staining of certain types of extended wear soft contact lenses Generalised skin eruptions Oligospermia, reversible on discontinuance of drug GI disturbance Pregnancy and Lactation If sulfasalazine is to be prescribed during pregnancy, an analysis of risks and benefits to the mother should be undertaken, against the possible small risk related to the unborn child and doses should not exceed 2 g/day. Folic acid: a supplement should be prescribed to those trying to conceive and during pregnancy. Small amounts of the drug may be excreted in breast milk although these are not thought to be a risk to a healthy infant. Interactions Cardiac glycosides—possibly reduces absorption of digoxin Combination therapy with azathioprine may contribute to bone marrow toxicity. Consultant / hospital responsibilities It is the hospital team’s responsibility to: Identify those patients who will benefit from treatment with sulfasalazine Undertake pre-treatment monitoring as detailed above Provide the first month’s prescription for sulfasalazine and provide written information on treatment to the patient and/or carers Provide the patient with monitoring blood forms whilst on treatment with copies of results sent to the GP (unless the GP chooses to take responsibility for both prescribing and monitoring) Undertake responsibility to act on pathology lab results (unless the GP chooses to take responsibility) Review efficacy of treatment at regular intervals and ensure any drug treatment changes are communicated to the GP Provide access to back up and support facilities Report any adverse events to the CSM Evaluate any adverse events reported by the GP. SSZ SCG Document status Final/Draft: Final 13 Jan 2009 Date of next review if final: 13 Jan 2010 Page 4 of 8 GP responsibilities It is the GP’s responsibility to: Return the shared care agreement letter to the consultant to indicate agreement with this guideline. If for any reason the GP is unhappy with the arrangements they should contact the appropriate hospital specialist Prescribe sulfasalazine at the dose recommended by the specialist. Any decision to alter or discontinue treatment should be taken after discussion with the hospital specialist Check for possible drug interactions when newly prescribing or stopping concurrent medication (see interaction section) Report any suspected or actual adverse drug reactions to the hospital specialist and the CSM Patient responsibilities It is the patient’s responsibility to: Report side effects to any member of the health care team Attend for blood testing when required to do so. Information to the patient The outpatient clinic will provide the patient with information about their treatment. Information about the patient to be received by the GP from the consultant Please refer to the shared care request letter attached. Two copies of this letter will be sent to the GP for each patient initiated on therapy. Patient information to be received by the consultant from the GP In order for GPs to agree formally to this shared care protocol, it is requested that both the shared care request letters attached be signed and one returned to the hospital specialist requesting shared care. Contacting secondary care If the patient’s Consultant is not available, one of the other Consultants or the Specialist Registrar will be able to help. Please call the Rheumatology department at RSCH on 01273 696955 x4631/3553 or PRH on 01444 441881 x 5432/5984 Out of hours Urgent problems should be referred to the medical team on call, contacted via RSCH switchboard on 01273 696955 or the PRH switchboard on 01444 441881 SSZ SCG Document status Final/Draft: Final 13 Jan 2009 Date of next review if final: 13 Jan 2010 Page 5 of 8 References 1 British National Formulary 54. Pharmaceutical Press, 2007. 2 Salazopyrin summary of Product characteristics http://emc.medicines.org.uk/emc/ assets/c/html/DisplayDoc.asp?DocumentID=3344 (18 October 2007, date last accessed). 3 Sweetman S. Martindale: the complete drug reference. Pharmaceutical Press, 2002. 4 Nørga°rd B, Czeizel AE, Rockenbauer M, Olsen J, Sørensen HT. Populationbased case control study of the safety of sulfasalazine use during pregnancy. Aliment Pharmacol Ther 2001;15:483–6. 5 Ostensen M, Ramsey-Goldman R. Treatment of inflammatory rheumatic disorders in pregnancy: what are the safest treatment options? Drug Saf 1998;19:389–410. 6 Preston S, Needs C. Guidelines on the use of antirheumatic drugs in women during pregnancy and child-bearing age. Ballieres Clin Rheumatol 1990;4:687–98. 7 Herna´ndez-Dı´az S, Werler MM, Walker AM, Mitchell AA. Folic Acid antagonists during pregnancy and the risk of birth defects. New Engl J Med 2002;343:1608–14. 8 Janssen NM, Genta MS. The effects of immunosuppressive and anti-inflammatory medications on fertility, pregnancy, and lactation. Arch Intern Med 2000;160:610–9. SSZ SCG Document status Final/Draft: Final 13 Jan 2009 Date of next review if final: 13 Jan 2010 Page 6 of 8 Confidential shared care request Consultant name Consultant address Date GP Name GP Address Sulfasalazine in inflammatory arthritis in adults ( 16 years old) Patient Name: Patient Hospital number: Patient Address: Patient NHS Number: Dear Dr. Your patient has been commenced on: Sulfasalazine, at a dose of: It would be appropriate for this patient’s therapy to be shared between primary and secondary care. The enclosed Shared Care Guideline provides additional information to support you in this. Please sign both copies of this letter to indicate your agreement and return one copy to my office; the other should be placed in the patient’s notes at your practice. Yours sincerely, Consultant name GP signature Print name SSZ SCG Document status Final/Draft: Final 13 Jan 2009 Date of next review if final: 13 Jan 2010 Page 7 of 8 Date Confidential shared care request Consultant name Consultant address Date GP Name GP Address Sulfasalazine in inflammatory arthritis in adults ( 16 years old) Patient Name: Patient Hospital number: Patient Address: Patient NHS Number: Dear Dr. Your patient has been commenced on: Sulfasalazine, at a dose of: It would be appropriate for this patient’s therapy to be shared between primary and secondary care. The enclosed Shared Care Guideline provides additional information to support you in this. Please sign both copies of this letter to indicate your agreement and return one copy to my office; the other should be placed in the patient’s notes at your practice. Yours sincerely, Consultant name GP signature Print name SSZ SCG Document status Final/Draft: Final 13 Jan 2009 Date of next review if final: 13 Jan 2010 Page 8 of 8 Date