Electrolyte Replacement Cardiovascular Surgery Orders
advertisement

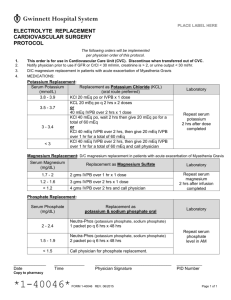
PLACE LABEL HERE ELECTROLYTE REPLACEMENT CARDIOVASCULAR SURGERY ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). 1. This order is for use in Cardiovascular Care Unit (CVC). Discontinue when transferred out of CVC. 2. Notify physician prior to use if GFR < 30 ml/min, creatinine is > 2, or urine output < 30 ml/hr. 3. MEDICATIONS: Potassium Replacement: Serum Potassium 3.8 - 3.9 3.5 - 3.7 3 - 3.4 <3 Replacement as Potassium Chloride (oral route preferred) 20 mEq oral or IVPB x 1 dose 40 mEq oral or 40 meq IVPB over 2 hours x 1 dose 40 mEq oral, wait 2 hours then give 20 mEQ oral for a total of 60 mEq or 40 mEQ IVPB, wait 2 hours then give 20 mEq IVPB for a total of 60 mEq 40 mEQ IVPB, wait 2 hours then give 20 mEq IVPB for a total of 60 mEq and call physician Magnesium Replacement: Serum Magnesium Replacement as Magnesium Sulfate 1.7 - 2 2 gms IVPB over 1 hr x 1 dose 1.2- 1.7 3 gms IVPB over 2 hrs x 1 dose < 1.2 4 gms IVPB over 2 hrs and call physician Phosphate Replacement: Replacement as sodium phosphate IV or potassium & sodium phosphate oral Serum Phosphate (oral route preferred) Neutra-Phos (potassium phosphate, sodium phosphate) 1 packet po q 6 hrs x 48 hrs 2 - 2.4 or Sodium phosphate 15 mM IVPB over 3 hrs x 1 dose Neutra-Phos (potassium phosphate, sodium phosphate) 2 packet po q 6 hrs x 48 hrs 1.5 – 1.9 or Sodium phosphate 20 mM IVPB over 4 hrs x 1 dose < 1.5 Sodium phosphate 30 mM IVPB over 6 hrs x 1 dose ______________ Date ___________________ Time Laboratory Repeat serum potassium 2 hours after dose completed Laboratory Repeat serum magnesium 2 hours after infusion completed Laboratory Repeat serum phosphate level in AM _________________________________ Physician Signature __________ PID Number Send copy to pharmacy *1-40036* FORM 1-40046 REV. 07/2012 Page 1 of 1 PLACE LABEL HERE ELECTROLYTE REPLACEMENT CARDIOVASCULAR SURGERY REFERENCE PAGE (For use with Form 40046) PLACE THIS COPY IN MAR SECTION OF CHART DURING EPISODE OF CARE. Potassium Replacement: Serum Potassium 3.8 - 3.9 3.5 - 3.7 3 - 3.4 <3 Replacement as Potassium Chloride (oral route preferred) 20 mEq oral or IVPB x 1 dose 40 mEq oral or 40 meq IVPB over 2 hours x 1 dose 40 mEq oral, wait 2 hours then give 20 mEQ oral for a total of 60 mEq or 40 mEQ IVPB, wait 2 hours then give 20 mEq IVPB for a total of 60 mEq 40 mEQ IVPB, wait 2 hours then give 20 mEq IVPB for a total of 60 mEq and call physician Magnesium Replacement: Serum Magnesium Replacement as Magnesium Sulfate 1.7 - 2 2 gms IVPB over 1 hr x 1 dose 1.2- 1.7 3 gms IVPB over 2 hrs x 1 dose < 1.2 4 gms IVPB over 2 hrs and call physician Laboratory Repeat serum potassium 2 hours after dose completed Laboratory Repeat serum magnesium 2 hours after infusion completed Phosphate Replacement: Serum Phosphate 2 - 2.4 1.5 – 1.9 < 1.5 Replacement as sodium phosphate IV or potassium & sodium phosphate oral (oral route preferred) Neutra-Phos (potassium phosphate, sodium phosphate) 1 packet po q 6 hrs x 48 hrs or Sodium phosphate 15 mM IVPB over 3 hrs x 1 dose Neutra-Phos (potassium phosphate, sodium phosphate) 2 packet po q 6 hrs x 48 hrs or Sodium phosphate 20 mM IVPB over 4 hrs x 1 dose Sodium phosphate 30 mM IVPB over 6 hrs x 1 dose Laboratory Repeat serum phosphate level in AM Nurse: Write a new order for each dose needed and corresponding lab. Date, time and sign as - “per protocol Dr XX / Your Name, RN” REFERENCE USE ONLY. NOT PART OF MEDICAL RECORD. (For use with Form 40046)