Prevention and Management of Chronic Diseases
advertisement

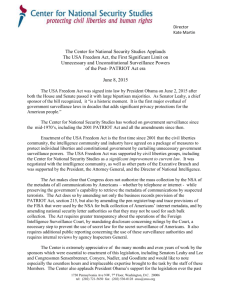
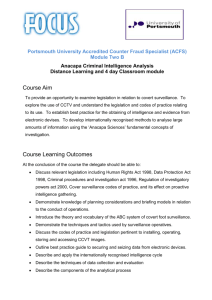
UNIT Prevention and Management of Chronic 2 Diseases Introduction There is continuity in the influences on chronic disease development throughout different stages of life, thus risks occur at all ages. Therefore prevention needs to occur from early on. Before we look at how to prevent these NCDs, there is a need to know about the diseases that contribute to the burden of chronic NCDs. In addition we need to understand the advances that have been made at the individual level in order to prevent chronic NCDs. For people who already have chronic diseases, the focus is mainly on controlling the disease and preventing complications. This section will focus on individual preventive measures that have been used. There are three sessions in this unit. Study Session 1: Pathophysiology of selected chronic NCDs Study Session 2: Methodologies for identifying risk factors for non communicable diseases Study Session 3: Health promotive behaviours and attitudes SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 29 SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 30 Unit 2 - Session 1 Pathophysiology of selected chronic NCDs Introduction In this session, you will be introduced to pathophysiology of selected Chronic Noncommunicable Diseases, which includes cardiovascular diseases, hypertension, diabetes, cancer, and Obstructive Lung Disease/COPD. A brief description of high cholesterol as a risk factor will also be given. The unit will only focus on basic information that will help you understand the bodily changes that occur due to these conditions. A list of references which will we give at the end of the session guide you to additional information to help you extend your knowledge on the subject if you wish to do so. The session consists of the following sections: Contents 1. Learning outcomes of this session 2. Readings 3. Cardiovascular Diseases 4. Hypertension 5. Diabetes Mellitus 6. High Blood Cholesterol 7. COPD 8. Cancer 9. Session summary 10. References Timing of this session In this session there is one reading and five tasks. It should take you at least two hours to finish the session. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 31 1 LEARNING OUTCOMES OF THIS SESSION In the course of this session, you will be addressing the Session Outcomes in the left column; they relate to the Module Outcomes indicated in the right hand column: Session Outcomes 2 Understand the aetiology of the different chronic non communicable diseases, namely cardiovascular diseases, hypertension, diabetes, cancer, and Obstructive Lung Disease/COPD. List the signs and symptoms for the different chronic non communicable diseases namely cardiovascular diseases, hypertension, diabetes, Obstructive Lung Disease/COPD. Understand the risk factors for cardiovascular diseases, hypertension, diabetes, cancer, Obstructive Lung Disease/COPD and cancer. Module Outcomes Understand the basic epidemiological concepts related to chronic diseases Make a reasonable argument why chronic diseases are a concern globally READINGS Barouki, R., Gluckman, P.D., Grandjean, P., Hanson, M. & Heindel, J.J. (2012). Developmental Origins of Non-communicable Disease: Implications for Research and Public Health. Environmental Health, 11:42. [Online]. Available: http://www.ehjournal.net/content/11/1/42 [Downloaded 12.08.12] 3 CARDIOVASCULAR DISEASES Cardiovascular diseases (CVDs) are major public health problems globally. They are a group of diseases that involve the heart and the blood vessels (arteries and veins). If there is an interruption of blood supply due to diseases of the vessels taking blood to the heart, the heart might be seriously damaged due to lack of oxygen and nutrients to fuel its muscular contractions. The medical term for this damage is referred to as a heart attack. If the same type of situation happens in the brain, and lack of oxygen disrupts the normal function of the brain, this is referred to as a stroke. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 32 Heart attacks and strokes are usually acute (meaning that they start suddenly and rapidly get worse), life-threatening events. They are mainly caused by a blockage that prevents blood from flowing to parts of the heart or brain, which are seriously damaged by the lack of oxygen. The blockage of blood flow may be due to fatty deposits (called plaques) on the inner walls of the blood vessels that supply the heart or brain. Strokes can also be caused by bleeding from a blood vessel in the brain or from blood clots blocking an artery. Risk factors for cardiovascular diseases and stroke includes behavioural factors such as: Unhealthy diet including diet high fat and sugar Being overweight or obese, which leads to the build-up of the fatty deposits (plaques) inside blood vessels that eventually block them, causing a heart attack or stroke. Physical inactivity Tobacco use. Drivers for behavioural risk factors include the social, economic and cultural conditions of people’s lives, especially poverty and stress. The effects of unhealthy diet and physical inactivity may show up in individuals as raised blood pressure, raised blood glucose, raised blood fats (lipids), and being overweight or obese – all of which make a heart attack or stroke more likely. 4 HYPERTENSION Hypertension is one of the leading risk factors for mortality worldwide. Hypertension is considered a ‘silent killer’ as many people who have it are not aware that they have the disease. It is therefore important that those who work with communities understand changes that occur in the body due to hypertension, including the signs and symptoms of hypertension, so that they are able to identify early signs in people who have the condition and advise them accordingly. Defining hypertension (high blood pressure) Hypertension or high blood pressure is a condition in which the blood pressure in the arteries is chronically elevated. High blood pressure is known as the ‘silent killer’ because many people may not be aware that they have the condition until they have a stroke. Facts about blood pressure Blood pressure (BP) refers to how hard the blood is pushing on the major blood vessels as it is pumped around the body by the heart. It is measured in millimetres (mm) of mercury (a liquid silver metal, which has the chemical symbol Hg), so blood pressure measurements are expressed as a number followed by mmHg. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 33 Two sounds (beats) can be heard when the heart pumps blood. These are: Systolic: When the heart contracts and pushes blood to the arteries, a beat that is referred to as the systolic pressure can be heard. Diastolic: When the heart relaxes to allow the blood from the body to get back to the heart before it is sent to the lungs through the veins, this causes a second beat referred to as the diastolic pressure. The normal level for blood pressure is below 120/80, where 120 represent the systolic measurement (peak pressure in the arteries) and 80 represents the diastolic measurement (minimum pressure in the arteries). Blood pressure between 120/80 and 139/89 is called prehypertension (to denote increased risk of hypertension), and a blood pressure of 140/90 or above is considered hypertension. How Hypertension develops Under normal circumstances the heart pushes blood through the arteries to the whole body. Blood pressure is the force of blood pushing against the walls of arteries as it flows through them. If for some reasons the blood vessels becomes narrow the blood does not flow smooth through the blood vessels and the heart has to push harder leading to a rise in the blood pressure. If the pressure is too high, the heart has to work harder to pump, and this often leads to organ damage and may results in several illnesses such as heart attack, stroke, heart failure, aneurysm, or renal failure. Risk factors for hypertension The exact causes of hypertension are unknown. There are several factors that are associated with the condition. These are referred to as risk factors and include: High level of fat (cholesterol) in the blood Smoking Obesity or being overweight Diabetes Sedentary lifestyle Lack of physical activity High levels of salt intake (sodium sensitivity) Insufficient calcium, potassium, and magnesium consumption Vitamin D deficiency High levels of alcohol consumption Stress Aging Medicines such as birth control pills Genetics and a family history of hypertension Chronic kidney disease Most of these factors are theoretically preventable by teaching the community to change their behavior to healthier ways. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 34 TASK 1: Symptoms of hypertension Think of the people you have seen or met who have hypertension. What do they often complain of? Compile a list of their complaints. Feedback: A large percent of people do not know that they have high blood pressure, as they do not notice any symptoms until too late. That is why high blood pressure is referred to as a ‘silent killer’. Some people die of stroke and yet they have never been diagnosed with high blood pressure. It is therefore advisable that people go for a check-up annually so they can be diagnosed early and treated before organ damage develops. Extremely high blood pressure may lead to some of the following symptoms: Severe headaches Fatigue or confusion Dizziness Nausea Blurred vision Chest pains Breathing problems Irregular heartbeat Blood in the urine 5 DIABETES Diabetes mellitus (sometimes called ‘sugar diabetes’) is a condition that occurs when the body cannot use glucose (a type of sugar) normally. When a person is in good health the body controls the level of blood glucose and does not allow this to become very high or very low. There is another type of diabetes, called diabetes insipidus, but it is very rare. Diabetes insipidus shares the name ‘diabetes’ because it also results in the production of large quantities of urine, but this has nothing to do with how the body manages glucose. This study session will focus only on diabetes mellitus, and from this point that is what we mean when we mention ‘diabetes’. Types of diabetes There are several types of diabetes, including two main types of diabetes mellitus: Type 1 and Type 2, and gestational diabetes. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 35 Type 1 diabetes is commonly found in children. In this type of diabetes, the body makes little or no insulin. Without enough insulin, glucose cannot enter the tissues and cells, and so the blood glucose level rises damagingly high. People with Type 1 diabetes are dependent on taking insulin every day – either in tablet or injection form. Although there is plenty of glucose in the blood, it cannot enter the tissues and, because of this, it cannot be used as a fuel source. Instead, the body breaks down fats and protein to use as fuel. As a result, the person often loses weight very rapidly due to loss of fluid, an inability to use glucose as a fuel, loss of muscle as protein is broken down, and loss of glucose in the urine. Type 2 diabetes usually occurs in adulthood, but young people are increasingly being found to be having type 2 diabetes, due to increasing exposure to risk factors for chronic noncommunicable diseases. In Type 2 diabetes, the pancreas does not make enough insulin to keep blood glucose levels normal, often because the body does not respond well to insulin. Type 2 diabetes may be present for many years before a diagnosis is made, because some people have few symptoms or take no notice of them, e.g. they may not see their thirst or getting up at night to pass urine as a problem. Having Type 2 diabetes for several years before a diagnosis is made can mean that complications of diabetes, which take years to develop, may already be present at the time of diagnosis. The difference between the two types of diabetes is that in Type 1 diabetes, the pancreas does not make enough insulin while in Type 2 diabetes, the body cannot respond normally to the insulin that is made. In both cases the glucose levels in the blood to rise, leading to symptoms such as increased urination, extreme thirst, and unexplained weight loss. Gestational diabetes is another type of diabetes where high blood glucose develops during pregnancy in a woman who does not have diabetes. Women who have gestational diabetes may later develop Type 2 diabetes and cardiovascular disease. Causes of diabetes The causes of Type 1 diabetes The exact cause of Type 1 diabetes is unknown. Genetics, viruses, and auto-immune problems may play a role. In most people with Type 1 diabetes, the body's own immune system, which normally fights harmful bacteria and viruses, mistakenly destroys the insulinproducing (islet) cells in the pancreas. Exposure to certain viruses may also trigger the disease. Once the islet cells are destroyed, the child will produce little or no insulin. The causes of Type 2 diabetes In Type 2 diabetes, the islet cells are still functioning, but the body becomes resistant to insulin or the pancreas doesn't produce enough insulin. The following are risk factors for developing Type 2 diabetes mellitus: Obesity Abdominal obesity Physical inactivity SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 36 Urbanisation Intra-uterine environment Genetics/heredity Symptoms and signs of diabetes A person who has untreated diabetes is likely to complain of the following symptoms: Feeling thirsty all the time, drinking a lot of water and Passing large amounts of urine, Excess weight loss, and Tiredness. 6 CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) Chronic obstructive pulmonary disease (COPD) is one of the most common lung diseases. Although COPD is a progressive condition, it can be partially reversible through correct treatment, especially if diagnosed early before complications set in. In most cases COPD is preventable. COPD poses a burden to the health care system and to the economy, and affects the quality of life of patients who suffer from the condition. Individuals who suffer with chronic obstructive pulmonary disease (COPD) or those with reduced lung function have a serious risk of developing cardiovascular disease. Chronic obstructive pulmonary disease is a condition in which the lungs have become permanently damaged and the airways are constantly narrowed therefore unable to process oxygen well. The common symptoms of this condition are shortness of breath and coughing. Diseases classified as COPD There are two major diseases that are included in the category of COPD: Chronic bronchitis - a chronic, inflammatory condition of the bronchi characterised by coughing and expectoration (spitting-up) of sputum (mucous coughed-up from the lungs) Emphysema - a respiratory disorder that is characterised by enlargement and eventual destruction of the air sacs (alveoli) in the lungs, through which oxygen passes from the lungs into the bloodstream. Risk factors for COPD Smokers (cigarette) are at a higher for COPD; Exposure to air pollution and industrial dusts and fumes increase; Chronic bronchitis is more common in people over 40 years old; emphysema occurs more often in people 65 years of age and older; COPD-related deaths are about twice as high among people of low socioeconomic status; COPD seems to run in families due hereditary factors, especially in the presence of smoking and air pollution; People with lung infections make all forms of COPD worse. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 37 Other risk factors for COPD are: Exposure to certain gases or fumes in the workplace; Exposure to heavy amounts of second hand smoke and pollution; Frequent use of cooking fire without proper ventilation. Important points to note People with chronic obstructive pulmonary disease are at risk of developing heart disease. As a systemic inflammatory disease, COPD may accelerate the development of CVD. Strenuous work or exercises may increase risk, as exertion increases the depth and rate of respiration, which in turn increases respiratory intake of air particles. High altitude may also affect their condition due to poor air quality which may compound the effects of lower oxygen levels. Patients with COPD are often advised to minimise exposure to fumes and particles, and to take medication before exposure to strenuous activities. They are also advised to use medications regularly and to monitor breathing symptoms to help maintain a normal life. You will notice that many of these conditions/diseases share common risks. However some of the diseases that manifest late in life have their origins in utero. Read the paper by Barouki et al, 2012 and then answer the question in Task 2. READING Barouki, R., Gluckman, P.D., Grandjean, P., Hanson, M. & Heindel, J.J. (2012). Developmental Origins of Non-communicable Disease: Implications for Research and Public Health. Environmental Health, 11:42. [Online]. Available: http://www.ehjournal.net/content/11/1/42 [Downloaded 12.08.12] TASK 2: Factors influencing risk What factors influence the risk for development of disease late in life? 7 CANCER Cancer is a term that refers to a condition in which abnormal cells divide without control and are able to invade other tissues. Cancer cells can spread to other parts of the body through SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 38 the blood and lymph systems. Under normal circumstances, cells in our bodies grow and divide. Some cells die but are continually renewed. With cancer, the cells of the body act abnormally in that they spread elsewhere in the body and grow in areas where that particular type of cell would not normally grow. A lump of new cells growing in an inappropriate location is known as a tumour (the general public often calls it a ‘growth’). The original mass of cells is called the primary tumour to distinguish it from any ‘break-away’ tumours that may form later, if cells from the primary tumour spread to other parts of the body. Types of tumours There are two types of tumours: benign and malignant. Most benign tumours are not life-threatening, though some may grow very large over a long time and eventually interfere with the functioning of a vital organ such as the liver, heart or brain. A malignant tumour on the other hand is cancerous growth. Some cells in a malignant tumour break away from the original primary mass of cells and spread around the body, carried in the blood stream or lymphatic vessels. The malignant cells become lodged in distant locations (e.g. in fine capillaries in organs like the lungs or breast) and begin to generate new secondary tumours. Types of Cancer Most cancers are named for the organ or type of cell in which they start - for example, cancer that begins in liver is called liver cancer; cancer that begins in the colon is called colon cancer. The main categories of cancer include: Lymphoma and myeloma - cancers that begin in the cells of the immune system. Carcinoma - cancer that begins in the skin or in tissues that line or cover internal organs. Sarcoma - cancer that begins in bone, cartilage, fat, muscle, blood vessels, or other connective or supportive tissue. Leukemia - cancer that starts in blood-forming tissue such as the bone marrow and causes large numbers of abnormal blood cells to be produced and enter the blood. The most common type of cancer in men is prostate cancer, while for women, it is breast cancer. Risk factors for cancers This section will introduce you to the idea of cancer risk factors that can increase our chance of developing a cancer. Knowing what they are can be helpful in educating the members of your community about how they can decrease their cancer risks by changing their behaviour or, if this is not possible, getting an early diagnosis: Old age is a cancer risk because as people get older cells accumulate more damage from avoidable risks (e.g. smoking, alcohol) and unavoidable exposures in the environment; Cigarette smoking and chewing tobacco; Genetic factors can also increase a person’s cancer risk; some families seem to have more than the average number of cancers arising in family members, and this is thought to be due to the existence of certain cancer-promoting genes in their cells; SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 39 8 Environmental risk factors, such as radiation and certain viruses; Exposure to some industrial chemicals (e.g. insecticides); Lack of exercise; Fatty diet leading to obesity ; Excessive alcohol consumption. SUMMARY In this Session the Pathophysiology of selected chronic non-communicable diseases were briefly described just to give you an idea of how these conditions develop. Their manifestation and risk factors were also described to enable you to identify people who have these conditions and advised them to take necessary actions to prevent them. The epidemiology and preventive measures for these conditions will be discussed in the following units. 9 REFERENCES Beevers, G., Lip, G.Y.H., O'Brien, E. (August 2001). The pathophysiology of Hypertension. British Medical Journal, 322: Mahler, R.J. & Adler, M. (1999). Type 2 Diabetes Mellitus: Update on Diagnosis, Pathophysiology and Treatment. The Journal of Clinical Endocrinology & Metabolism; 84(4): xx. Barnes, P.J. (2010). Chronic Obstructive Pulmonary Disease: Effects beyond the Lungs PLoS Medicine, 7(3): e1000220. doi:10.1371/journal.pmed.1000220 SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 40 Unit 2 - Session 2 Methodologies for identifying risk factors for non communicable diseases In this session we will look at the methodologies used to for identify risk factors for non communicable diseases. Several methods have been used to identify risk factors in population. Identification of risk factors is useful to guide the planning of appropriate responses that prevent and control chronic diseases and thus improve the quality of life of the population. Knowledge and skills in surveillance and monitoring are therefore important for the public health practitioner involved in the control of chronic diseases. In this session we will focus on surveillance as of the methodologies used for identifying risk factors Contents 1. Learning outcomes of this session 2. Readings 3. Basic principles and concepts of disease surveillance? 3.1 Definition of surveillance 3.2 Types of Surveillance 3.3 Purpose and benefits of Surveillance 4. Developing a chronic disease surveillance system 4.1 Establishing the need for a surveillance system 4.2 Data Sources and collection 4.3 Data Analysis and interpretation 4.4 Data dissemination 4.5 Ethical and legal considerations 5. Evaluation of surveillance systems 6. Session summary 7. References and further reading Timing of this session In this session there are four readings and seven tasks. It should take you at least two and a half hours to finish the session. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 41 1 LEARNING OUTCOMES OF THIS SESSION At the end of this session, you should be able to: Explain the concepts of disease surveillance, monitoring and evaluation, as used in Epidemiology. Describe epidemiological techniques/approaches relevant for the monitoring of chronic diseases. Develop monitoring and evaluation systems for the surveillance of chronic diseases. 2 READINGS Nsubuga, P., White, M.E., Thacker, S.B. et al. (2006). Public Health Surveillance: a Tool for Targeting and Monitoring Interventions. In D.T.Jamison et al. (Eds.) Disease Control Priorities in Developing Countries (2nd Ed). DCPP. Ch. 53: 997-1015 Brownson, R.C. & Bright, M.S. (2004). Chronic Disease Control in Public Health Practice: Looking Back and Moving Forward. Public Health Reports, 119: 230-238. Piriyawat, P., Smajsova, M., Smith, M.A., Pallegar, S., Al-Wabir, A. et al. (2002). Comparison of Active and Passive Surveillance for Cerebrovascular Disease. The Brain Attack Surveillance in Corpus Christi (BASIC) Project. American Journal of Epidemiology.156: 1062-1069 McNabb, S.J.N., Chungong, S., Ryan, M., Wuhib, T., Nsubuga, P. et al. (2002). Conceptual Framework of Public Health Surveillance and Action and its Application in Health Sector Reform. BioMed Central Public Health 2002, 2: 1-9 [Online]. Available: www.biomedcentral.com/147-2458/2/2 [Downloaded 9.7.07]. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 42 3 BASIC PRINCIPLES AND CONCEPTS OF DISEASE SURVEILLANCE 3.1 Definitions of surveillance TASK 1: Defining ‘surveillance’ 1. Try to provide your own definition for the term ‘surveillance’. A dictionary definition of the term is as follows: ‘watch or guard over a person, especially a suspected person, a prisoner or the like’. 2. The above definition refers to ‘police-type’ surveillance. Can we apply the same to Public Health? 3. How would you define disease surveillance? Identify key elements in the definition of surveillance as used in epidemiology. FEEDBACK Surveillance is defined as “the ongoing, systematic collection, collation, analysis and interpretation of outcome-specific data essential to the planning, implementation and evaluation of public health practice, closely integrated with the timely dissemination of these data to those who need to know.” Note the italicised elements of the definition above. Surveillance should: - be continuous and involve the systematic scrutiny of health data/information - have as its essence, the collection of data for action - entail rapid reporting and analysis of health related data as well as a rapid action to correct the problem READING McNabb, S.J.N., Chungong, S., Ryan, M., Wuhib, T., Nsubuga, P. et al. (2002). Conceptual Framework of Public Health Surveillance and Action and its Application in Health Sector Reform. BioMed Central Public Health 2002, 2: 1-9 [Online]. Available: www.biomedcentral.com/147-2458/2/2 [Downloaded 9.7.07]. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 43 TASK 2: Consider an alternative definition Last (1990) defined surveillance as the ‘systematic, regular ascertainment of incidence using methods distinguished by their practicality, uniformity, and frequently their rapidity rather than by their accuracy’. Based on your reading so far, and with reference to this definition: 1. Describe the trends in the application of surveillance in Public Health 2. Outline the core activities of public health surveillance. 3.2 Types of disease surveillance READINGS Nsubuga, P., White, M.E., Thacker, S.B. et al. (2006). Public Health Surveillance: a Tool for Targeting and Monitoring Interventions. In D.T.Jamison et al. (Eds.) Disease Control Priorities in Developing Countries (2nd Ed). DCPP. Ch. 53: 997-1015 Piriyawat, P., Smajsova, M., Smith, M.A., Pallegar, S., Al-Wabir, A. et al. (2002). Comparison of Active and Passive Surveillance for Cerebrovascular Disease. The Brain Attack Surveillance in Corpus Christi (BASIC) Project. American Journal of Epidemiology.156: 1062-1069 Two broad types of surveillance are described in the readings: Passive surveillance (‘Cold pursuit’): Here, one relies on external sources to gather health information. For example data used to monitor the occurrence of a disease is generated as a result of the use of health services by persons who seek medical attention. The notification of diseases and sentinel surveillance are examples. Often such passive surveillance undercounts the number of health problems because reporting is voluntary. It is usually prescribed by legislation for universal implementation. Active surveillance (‘Hot pursuit’): In this case, one actively seeks out health-related information. For example, the providers of health services conduct a survey in apparently well persons to identify those with sub-clinical disease or those who harbour the agents of the disease but have not by themselves approached the health service for medical attention. Periodic blood smears for malaria, screening for blood glucose, hypertension and ANC seroprevalence surveys of HIV are examples. Nsubuga et al (2006) further describe other forms of surveillance, inter alia; syndromic surveillance; integrated surveillance; behavioural risk factor surveillance; categorical surveillance; the health information and management systems and the routine health information system. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 44 TASK 3: Classifying surveillance methods 1. Identify any 5 disease surveillance systems that exist (or have existed) in your area. Briefly describe these, classifying them as active or passive surveillance, and explain your classification. 2. According to Piriyawat et al (2002), how does active surveillance of cerebrovascular accident compare with passive surveillance? 3. What, in your opinion, are the implications for a district health manager interested in setting-up a surveillance system of this condition? 3.3 Purpose and benefits of surveillance Why should we be concerned about disease monitoring? “Good monitoring does not necessarily ensure the making of good decisions but it reduces the risk of making bad ones” Languimer, 1963. Refer back to the Nsubuga et al (2006) reading for more information on this topic. After reading the text, is there anything you can add to the following list of the purposes/uses of surveillance? ● ● ● ● ● ● ● ● ● ● ● ● ● ● To give an accurate assessment of the health status of a given population; To estimate the magnitude of a health problem; To give a quantitative base to define objectives for action; To establish long-term trends in disease occurrence; To detect epidemics; To give measures used to define specific priorities in resource allocation; To set research priorities; To help identify high risk groups or areas; In portraying the natural history of a disease; Useful to test the hypothesis on the effectiveness of specified interventions in controlling a particular disease; Provide information that enables providers of health care to target communities most in need of interventions; Provide information necessary for monitoring the characteristics, extent of spread and immunologic effects of an infectious agent; Form the basis for rational planning of public health intervention; Useful to monitor specific priorities. In short, surveillance provides a scientific, factual basis for appropriate policy decisions in public health practice and in rational allocation of resources. It is the essential management tool for good public health practice. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 45 4 DEVELOPING A CHRONIC DISEASE SURVEILLANCE SYSTEM 4.1 Establishing the need for a surveillance system TASK 4: Identify ways of setting up a system Refer to the Nsubuga et al. (2006) reading. Describe the elements in establishing and maintaining a surveillance system. FEEDBACK You should now be familiar with Thacker and Stroup (1998) flow-charts on elements in establishing and maintaining a surveillance system. Other conditions necessary to establish a surveillance system: Statutory empowerment or support by appropriate health authority Clearly defined goals of the surveillance system Clearly defined responsibilities and assignment of tasks to specific persons and authorities Determine the inputs, processes and outcomes of the surveillance system Select clear, simple and practical case definition Establish the environment that will ensure support by all those involved in the surveillance system Critically review the presented case study of the development of the Philippine national epidemic surveillance system contained in your reading. How, according to the authors, were the challenges of “multiple-vertical systems” overcome in the development of this system? 4.2 Data sources READING Brownson, R.C. & Bright, M.S. (2004). Chronic Disease Control in Public Health Practice: Looking Back and Moving Forward. Public Health Reports, 119: 230-238. TASK 5: Evaluating sources of data 1. Identify the advantages and disadvantages of each of the sources of data described in your reading. 2. Are these sources available in your locality? If not available, could they be established, and if so how? SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 46 FEEDBACK Consider the following table adopted from the Health Canada (2003). SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 47 4.3 Data analysis and interpretation READING Brownson, R.C. & Bright, M.S. (2004). Chronic Disease Control in Public Health Practice: Looking Back and Moving Forward. Public Health Reports, 119: 230-238. The reading describes the analysis of surveillance data in terms of the epidemiological variables of person, place and time. You may want to review basic concepts of descriptive epidemiology at this stage. Some other important things to note are: - Analyses should be done as close to the primary reporting level as possible - Training in data analysis is important (analytic methods, data presentation) 4.4 Data dissemination The essence of the surveillance system is to guide interventions. Recall that our definition of surveillance posits that information needs to be disseminated to the appropriate quarters, and this should be done timeously. In your reading, there is discussion of a framework of 5 steps for communicating surveillance information. These are: - Establish the message Set an objective Define the audience Select the channel Evaluate the impact The last step, (evaluating the impact), although often expensive, time-consuming and difficult to interpret, is core to surveillance efforts and will be discussed further later in this session. 4.5 Ethical and legal considerations TASK 6: Think about legal considerations Based on your readings and what you have learned so far, what ethical and/or legal considerations do you feel should be taken into account in implementing surveillance systems? FEEDBACK You may have identified the following; can you expand on these? SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 48 Protection from misuse Confidentiality Anonymous reporting 5 EVALUATION OF SURVEILLANCE SYSTEMS Why is it important to evaluate our surveillance system? What should we be evaluating in the surveillance system? Evaluating the surveillance system provides several benefits: Evaluate the public health importance of the condition being monitored Evaluate the cost and usefulness of a surveillance system Evaluate the process in the surveillance system Evaluate the sensitivity and specificity of tests TASK 7: Evaluating and using surveillance data Part A. Routine statistical data gathered at Tygerberg Hospital shows higher fatality rates in male patients admitted for Cerebro-vascular accident over the past 2 years compared with rates from a similar period a decade ago. How should any judgment about the significance of these observations be made? How can such an observation be investigated further? Part B. Following further investigation, it is determined that there is increasing incidence of CVA in all health districts of the Western Cape. Mass screening is to be initiated but there is concern about the cost. Describe how you would establish a surveillance system for CVA in the province. What monitoring measures would you put in place for your surveillance system? Look at the conceptual model on the following page, designed by a chronic disease intervention group. It is useful in understanding that the end-result of surveillance is to influence intervention. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 49 A conceptual framework: ‘High-level surveillance model’ of the Chronic Disease Subgroup, Health Canada. INPUTS Information Management Data Collectio n Health Surveillance OUTPUTS Basic Research Integration Public, Professional & Stakeholder Input Actions Knowledg e synthesis and Decisionmaking Analysis - Programs Intervention s - Policy Surveillance Products O U T C O M E S Disseminati on Management Coordination Legislation & Regulation Applied research & epidemiologic al studies Social & economic considerations Other consideratio ns This surveillance model describes a cyclical process where information, derived from data and supplemented by other information, leads to greater knowledge and decision- making capabilities. This prompts actions that will have an impact on disease incidence, risk behaviours and other determinants and (ultimately) produce better health. There are six core functions of surveillance: data collection, data integration, data analysis, interpretation, development of surveillance products, and dissemination. These are supported by the appropriate infrastructure and functions of management, coordination, information management and in some instances, legislation and regulation. Also see McNabb et al (2002) for their conceptual framework of public health surveillance and action. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 50 6 SESSION SUMMARY In this session, we have described the basic principles and concepts of disease surveillance and monitoring, and applied these to the prevention and control of chronic diseases. We further explored the elements of establishing a chronic disease surveillance system, inter alia establishing the need for the system, data sources and collection, data analysis and interpretation, data dissemination, ethical and legal considerations as well as methods of evaluating surveillance systems. The session concludes by emphasizing the importance of linking these data to chronic disease prevention and control efforts in a ‘high-level surveillance’ system. 7 REFERENCES AND FURTHER READING Health Canada. (July 2003). Chronic Disease Surveillance in Canada - a Background Paper. Available (online): http://publications.gc.ca/collections/Collection/H39-6662003E.pdf? Thacker, S.B. & Stroup, D.F. (1998). Public Health Surveillance. In R.C. Brownson & D.B. Petiti (eds). Applied Epidemiology: Theory and Practice. New York: Oxford University Press. SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 51 SOPH, UWC, Master of Public Health: Epidemiology and Control of Non-communicable Diseases – Unit 2 52