Anticonvulsant Drugs
advertisement

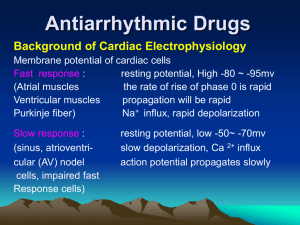
Antiarrhythmic Drugs Introduction of arrhythmia i. Defination When the rhythm of the heart become irregular, or the frequency of the atrial and ventricular beats are different, too fast (tachycardia) or too slow (bradycardia), this is called an arrhythmia. An arrhythmia is an abnormality in the heart's rhythm, or heartbeat frenquency. ii. Classification Bradycardia - a heart rate that is lower than normal(<60/min). * Sinus bradycardia * AV nodal blocks Tachycardia -a heart rate that is higher than normal(>100/min) Sinus tachycardia Atrial tachycardia Atrial flutter Atrial fibrillation Supraventricular tachycardia (SVT) Ventricular premature beats (VPBs) Ventricular tachycardia (VT) Ventricular flutter Ventricular fibrillation 1 iii. Treatment Many arrhythmias do not require any treatment. Some arrhythmias may need treatment because rhythm that are too rapid, too slow can reduce cardiac output. Some types of arrhythmias, such as ventricular tachycardia, are serious and even life-threatening. Arrhythmias can be treated with drugs disscussed in this chapter or with non-pharmacollogical therapies such as pacemaker, cardioversion, catheter ablation, and surgery. Section 1 Basis of Cardiac Electrophysiology Important properties Automaticity: The heart can excite itself without exogenous stimulus. The automaticity results from Spontaneous depolarization in Phase 4 (slope of Phase 0). Conductivity: The impulse can spread among cells. Conductivity is determined by the rate and amplitude of Phase 0 depolarization. APD & ERP: During phases 0, 1, 2, and part of phase 3, the cell is refractory to the initiation of new action potentials. This is termed ERP (effective refractory period). During the ERP, stimulation of the cell does not produce new, propagated action potentials. The ERP acts as a protective mechanism in the heart by preventing multiple, compounded action potentials from occurring. Many anti-arrhythmic drugs prolong the ERP, thereby reducing cellular excitability. APD is action potential duration, and its most important component is ERP. Section 2 Mechanism of arrhythmias Altered impulse formation * Increased autorhythmicity * Afterdepolarizations Early afterdepolarizations (EAD) Delayed afterdepolarizations (DAD) Altered impulse conduction * Reentry Reentry requires three conditions coexisting: presence of a unidirectional block a anatomic or physiologic circuit critical timing. The conduction time must exceed the effective refractory period Section 3 Mechenism of anti-arrythmic effect Mechenism of antiarrythmic effect * Reduce abnormal automaticity (phase 4 slope) * Reduce afterdepolarization • decrease action potential duration • block sodium or calcium channel * Abolish reentry--slow conduction further a.↑conduction:↓unidirectional block b.↓conduction : unidirectional block→ bidirectional block 2 c.↑ERP Section 4 Antiarrythmic Drugs Class I---Na Channel Blocker Class IA moderate potency Class IB low potency Class IC high potency Class II ---β-blocker Class III the drugs prolonging APD Class IV---calcium channel blocker A given drug may have multiple classes of action. For example, amiodarone shares all four classes of action. Drugs are usually discussed according to the predominant class of action. Certain antiarrhythmic agents, eg, adenosine, do not fit readily into this scheme and are described separately. Sodium Channel Blockers 1) ClassⅠA a. Inhibit Na+ influx moderately : ↓the rate and amplitude of Phase 0 depolarization, ↓conduction ↓phase 4 slope, ↓autorhythmicity b. ↓ K+ efflux, prolong the ERP Quinidine(奎尼丁) –its use has decreased considerably in recent years. Pharmacological Effects: Cardiac Effects: ↓autorhythmicity;↓conduction;↑ERP; ↓myocardial contractility. Extracardiac Effects: α-adrenergic blocking and anticholinergic effect Therapeutic Uses: Broad-spectrum Atrial fibrillation; Atrial flutter; supraventricular tachycardia; ventricular tachycardia; Toxicity: Gastrointestinal side effects Chichonic reaction(cinchonism) CVS: Heart failure; hypotension; quinidine syncopy 2) Class IB ↓Na+ influx lightly ↑K+ efflux, shorten the APD>ERP, ERP/APD ↑ Lidocaine (利多卡因) Pharmacological effects: Act on Purkinje fibers and ventricular cells a.↓autorhythmicity;↓the slope of phase 4 and ↑the threshold for excitability. b. Relative increase ERP: ERP/APD↑ Pharmacokinetics: Therapeutic Use Ventricular Tachycardia and Ventricular Fibrillation in + 3 •Myocardial infarction •Digitalis intoxication •Open-heart surgery Phenytoin sodium: It has been used in the acute and chronic ventricular arrhythmias, especially in digitalis intoxication. Mexiletine is a congener of lidocaine that is resistant to first-pass hepatic metabolism and is effective by the oral route. Its electrophysiologic and antiarrhythmic actions are similar to those of lidocaine. 3) Class IC Severely depress Na+ influx, markedly ↓conduction. ↓phase 4 slope. ↓ autorhythmicity Serious adverse reactions are provocation of potentially lethal arrhythmias. Propafenone: Block Na+ and Ca2+ channel, also blockβ-R Used to treat Supraventricular and ventricular tachycardia; Supraventricular and ventricular premature beat, Atrial fibrillation. The most common adverse effects are a metallic taste and constipation; arrhythmia exacerbation can occur. Class Ⅱ β-R Blockers Propranolol 1) β-R blocking action 2) Membrane-stabilizing effect(↓Na+in) Pharmacological effects: a.↓autorhythmicity,↓afterdepolarization stimulated by CA, prevent triggered activity. b.↓ conduction of AV node and P-f ( >100ng/ml) c.↑ERP of AV node,↓reentry d. Improve myocardial ischemic Therapeutic uses Supraventricular arrhythmias; Acute myocardial infarction(AMI) Class Ⅲ Prolonging APD agents + + Blocking K channel , ↓ K efflux , ↓ repolarization, ↑ APD and ERP Amiodarone Pharmacological effects: ↓K+, Na+, Ca2+ ions channel;Blocking α, β receptor 1) ↑APD and ERP, no reverse use-dependence 2) ↓autorhythmicity 3) ↓ conduction of AV node and Purkinje fibers 4) Dilate coronary artery, ↓ myocardial oxygen consumption Pharmacokinetics: F: 35-60%, t1/2 25~60 d, last 4~12w Therapeutic uses: Broad-spectrum antiarrhythmic drug Life-threaten ventricular arrythmias; Artial fibrillation or atrial flutter; superventricular tachycardia Adverse effects: CVS reactions: Sinus bradycardia, Atrial-ventricular block, long QT syndrome (LQTS), hypotension. Pulmonary fibrosis; Abnormal liver function; cornea deposits; skin deposits; Hypo- or 4 hyperthyroidism Sotalol : Nonselective β-R antagonist; Block Ik,↑APD、ERP; F=90%~100%; Broad-spectrum antiarrhythmic drug. Dofetilide: Blocking K+ channel (Ikr) selectivrly, ↓K+ efflux Delay repolarization, APD and ERP↑ Dofetilide is approved for the maintenance of normal sinus rhythm in patients with atrial fibrillation. It is also effective in restoring normal sinus rhythm in patients with atrial fibrillation. Its main adverse effect is Tdp(2%~4%). Class IV: Calcium Channel Blockers Verapamil Pharmacological effects: 1. Reduction the automaticity of S-A node and ischemic myocardium (↓afterdepolarization) 2. Slow AV Node Conduction 3. Prolong AV Node ERP Therapeutic Use: Supraventricular tachycardia arrythmias: * Reentrant supraventricular (first choice) * Atrial fibrilation and flutter ( reduce the ventricular rate) Others Adenosine Act on A-R, activate KACh ,↑K+ efflux, ↓Ca2+ influx, hyperpolarization and ↓ automaticity; Prolong AV Node ERP. Choice for prompt conversion of paroxysmal supraventricular tachycardia. 5