Pressure Ulcer prevention and management strategy
advertisement

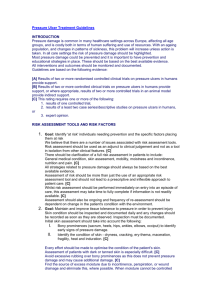
Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults Version 4 Name of responsible (ratifying) committee Nursing & Midwifery Group Date ratified 09.05.2013 Document Manager (job title) Tissue Viability Clinical Nurse Specialist Date issued 11th September 2013 Review date June 2015 Electronic location Corporate Clinical Guideline Related Procedural Documents Key Words (to aid with searching) Pressure ulcers, pressure ulcer prevention, grade of pressure ulcers, Braden, medical equipment, nutrition Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) Page 1 of 18 CONTENTS 1. QUICK REFERENCE GUIDE …………………………………………………………………...3 2. INTRODUCTION ………………………………………………………………………………….4 3. PURPOSE …………………………………………………………………………………………4 4. SCOPE …………………………………………………………………………………………….4 5. DEFINITIONS ……………………………………………………………………………………..4 6. RESPONSIBLITIES..……………………………………………………………………………..5 7. PROCESS …………………………………………………………………………………………6 8. TRAINING REQUIREMENTS ………………………………………………………………….12 9. REFERENCES AND ASSOCIATED DOCUMENTATION ………………………………….13 10. MONITORING COMPLIANCE WITH, AND THE EFFECTIVENSS OF, PROCEDURAL DOCUMENTS ………………………………………………………………………………………18 Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 2 QUICK REFERENCE GUIDE Key principles of pressure ulcer prevention and management include the following: Structured Assessment + Clinical Judgement All patients to undergo daily assessment Skin inspection for patients at risk Use mirror to inspect heels Implement pressure ulcer prevention strategies for at risk patients Address nutritional needs and any moisture/incontinence Prevention equipment including mattress, cushion, glide sheets, heel protectors Repositioning and limited seating + Patient and carer education Skin marking: indicates need to review strategy Re-assessment Evaluate strategy and adjust strategy Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 3 INTRODUCTION Pressure ulcers are an economic burden on the National Health Service (NHS) equating to 4% of the NHS budget (Bennett et al 2004). More importantly, pressure ulcers are detrimental to patients in terms of their physical, psychological and social well being resulting in reduced quality of life and maybe mortality (Fox 2002). The calculated cost of grade 1 pressure ulcer is £1214 rising to £14108 for a grade 4 pressure ulcer (Dealey et al 2012). Portsmouth Hospitals NHS Trust should have an integrated, multidisciplinary approach to the prevention and management of pressure ulcers with a clear strategy supported by senior management (NICE 2005, RCN 2005). Care should be delivered within the context of continuous quality improvement where improvements are identified by regular audit, feedback and review of each Clinical Service Centre Action Plans by the Pressure Ulcer Working Group. Patients should receive an initial pressure ulcer risk assessment within 4 hours of admission and if identified at risk a pressure ulcer prevention strategy must be implemented to reduce or remove risk factors. Daily ongoing risk assessments should be carried out or more frequently if the patient’s condition deteriorates and pressure prevention strategies adjusted accordingly. All pressure ulcers should be categorized or graded using European Pressure Ulcer Advisory Panel (EPUAP) Classification System (2009) and reported via the Trust’s DATIX reporting system. It is the aim of this Trust to eliminate all avoidable pressure ulcers. 1. PURPOSE The aim of the High Impact Action - Your Skin Matters (2009) is to have “No avoidable pressure ulcers in NHS provided care”. It is the purpose of this policy to ensure all staff adopt a zero tolerance of hospital acquired pressure ulcers. All patients admitted to hospital will be assessed within 4 hours of arrival and pressure ulcer prevention strategies will be immediately implemented to prevent pressure damage occurring. Ongoing re-assessments will continue daily throughout the patients’ stay and strategies adjusted accordingly to meet individual needs. 2. SCOPE This policy and guideline is intended to be used by all members of staff using a multidisciplinary team approach in the prevention and management of pressure ulcers 3. DEFINITIONS Pressure ulcers are also known as ‘pressure sores, bed sores and decubitus ulcers’. A pressure ulcer is defined as “localised injury to the skin and/underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear. A number of contributing or confounding factors are also associated with pressure ulcers; the significance of these factors is yet to be elucidated” (EPUAP 2009). Pressure ulcers occur when a bony prominence is in contact with a surface for prolonged periods of time. The most common sites include the buttocks, hips and heels but they can occur over any bony prominence (NICE 2005). Avoidable and Unavoidable Pressure Ulcers The Department of Health (2010) has recognized that, while most pressure ulcers are avoidable, there are those few which may be unavoidable. Their definition of ‘Avoidable’ pressure ulcers is: Avoidable Pressure Ulcer: For a pressure ulcer to be considered avoidable, the care-provider did not: Evaluate the person’s clinical condition and pressure ulcer risk factors Plan and implement interventions that are consistent with the persons needs and goals, and recognized standards of practice Monitor and evaluate the impact of the interventions; or revise the interventions as appropriate Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 4 Unavoidable Pressure Ulcer: For a pressure ulcer to be considered ‘Unavoidable’, the person receiving care developed a pressure ulcer even though the care-provider had: Evaluated the person’s clinical condition and pressure ulcer risk factors Planned and implemented interventions that are consistent with the persons needs and goals and recognized standards of practice Monitored and evaluated the impact of the interventions and revised the approaches as appropriate The individual person refused to adhere to prevention strategies in spite of education of the consequences of non-adherence To determine whether pressure ulcers are unavoidable, there must be documentary evidence demonstrating the actions taken to prevent pressure damage during the patient’s episode of care (NHS 2012). For consistency, it is recommended that the EPUAP (2009) (Fig 1) classification system is used to identify pressure damage. Deep Tissue Injury is a purple or maroon localised area of discoloured intact skin and will be classified as grade 3 with the potential to deteriorate to a grade 4 (NHS 2012). Fig 1: EPUAP & NPUAP (2009) Pressure ulcer grading or categories: Definition of Moisture Lesions (Appendix 1) Moisture lesions will be present when there is a history of moisture on the skin due to urinary or faecal incontinence or combination of both. It can also be related to sweating resulting in increased friction between skin folds or from excessive wound exudate in contact with the skin for prolonged periods. The moisture lesions manifests as redness, with or without blistering or erosions often with irregular shaped edges (Guy 2012). There are diffuse areas of partial thickness skin loss that can bleed or ooze serous fluid. Moisture lesions can occur in skin folds, over the buttocks and around the perineum. If the damage is caused by moisture, it should not be recorded as a pressure ulcer. Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 5 Combined moisture and pressure lesions are a result of pressure and moisture where there is necrotic or sloughy tissue present within the area of skin damage. This should be reported as combined moisture and pressure damage. Skin Care At End Of Life: The skin is the largest organ of the body and can fail. End of life is a phase of life when a person living with an existing illness, can deteriorate leading to death. It is acknowledged that during this period, vital organs will gradually cease functioning. The skin will reflect this and show loss of integrity and can result in spontaneous skin damage despite preventative measures (SCALE 2009). 4. DUTIES AND RESPONSIBILITIES All members of the multi-disciplinary team should be involved in the prevention and management of pressure ulcers. As the majority of pressure ulcers are preventable and costly to treat, it requires a high level of awareness within the multi-disciplinary team and each member is accountable for his or her own practice. Chief Executive As the accountable officer, the Chief Executive has a responsibility to ensure that there are robust systems in place in relation to patient safety and pressure ulcer prevention and management. Responsibility with regard to the systems and processes related to pressure ulcer prevention and management must be delegated to appropriate Executive Director. Director of Nursing The Chief Nurse or Director of Nursing, provides Board Level representation, and is responsible for ensuring that safe clinical systems are in place with regard to the prevention and management of pressure ulcers. This is delegated to be overseen by the Pressure Ulcer Working Group and Patient Safety Group. Midwifery & Nursing Group Nursing & Midwifery Group is responsible for approval of this policy and associated guidelines for pressure ulcer prevention and management Pressure Ulcer Working Group The Pressure Ulcer Working Group is responsible for strategic implementation of the pressure ulcer prevention and management strategy Senior Nurse The Senior Nurse is responsible for developing, implementing and evaluation Clinical Service Centre Action Plan for the prevention and management of pressure ulcers. The Senior Nurse, or their deputy, will also support the activities of the Pressure Ulcer Working Group Modern Matron The Modern Matron is responsible for ensuring the implementation and audit of their Clinical Service Centre Action Plan. Ward Manager The ward manager is responsible for implementation of this policy and associated guideline at ward level ensuring that all staff have read and understood the contents. It is also the responsibility of each ward manager to ensure that the correct information on the incidence of pressure ulcers is recorded on DATIX. The ward manager is also responsible for ensuring that staff maintain their competencies for pressure ulcer prevention and management. Registered Nurse It is the responsibility of registered nurses to: Carry out a structured risk assessment within 4 hours of admission Inspect skin if patients identified at risk daily or more frequently if their condition deteriorates Implement, evaluate and document pressure ulcer prevention strategy for those patients identified at risk from pressure damage Continue to daily risk assess patients during their hospital stay including skin inspection for those at risk Address nutritional needs Provide patient and/ carer education Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 6 Report the incidence of pressure ulcers as a clinical incident on DATIX system a Assess any existing pressure ulcers on admission and report on DATIX and re-assess weekly Ensure all grade 3 and 4 pressure ulcers to be photographed Ensure all patients with a pressure ulcer should have a wound care plan Ensure all patients with diabetes or with diabetic foot ulcers are assessed and referred (Appendix Diabetes inpatient assessment proforma) Tissue Viability Team The Tissue Viability Team is responsible for planning, implementing and evaluating a strategic approach within the Trust to reduce the occurrence of avoidable pressure damage through education and guidelines. The Tissue Viability Team is also responsible for ensuring policies, practice guidance and advice is based on best available evidence and to provide accessible and responsive service to wards and departments. Tissue Viability Link Nurse: The Tissue Viability Link will act as a resource with all health care professions in their area to increase the awareness and dissemination of tissue viability information. They will also be available to ward staff in the clinical area to give advice and support. Health Care Support Workers Under the supervision of a Registered Nurse, Health Care Support Workers are responsible for implementing the pressure ulcer prevention and management plan, for example: repositioning of patients, reporting changes in skin condition and obtaining relevant equipment. Medical Staff The Consultant has overall responsibility to plan and co-ordinate the patient’s medical treatments and are responsible for maintaining the patient’s optimum, physiological condition especially hydration, nutrition and infection. The Consultant should ensure referral to other healthcare professionals to utilize specialist knowledge in assessing and treating patients. Medial staff should be aware of patients with pressure ulcers ensure that the patients are receiving the optimum care Dietician Although the registered nurse is responsible for carrying out a nutritional screen using the MUST screening tool, further advice may be need from the Dietician Occupational Therapist The occupational therapist will advise on the suitability and correct use of specialist pressure relieving devices, for example cushions, seating and wheelchairs to reduce the risk of pressure ulcer development Physiotherapist The physiotherapist has a role in teaching patients and other professionals to move and reposition patients to minimise trauma to the skin and promote recovery and early mobilization Podiatry Podiatrists have an active role in the care of diabetic foot ulcers, will review patients in the community and provide devices to off load pressure from vulnerable areas of the feet. All patients with diabetic foot ulcers should be referred to Podiatry on discharge 5. PROCESS 6.1a. Patient-centered care Patients and their carers must be made aware of this policy and guideline and provided with an information leaflet. They should be informed of the potential risks of developing pressure ulcers in hospital and participate in the decision-making process when planning, implementing and evaluating their care (NICE 2005) 6.1b. Risk Assessment Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 7 The aim of a risk assessment is to identify the presence of predisposing and precipitating factors that may influence pressure ulcer development. An individual’s potential to develop pressure ulcers is influenced by the following extrinsic and intrinsic factors and must be considered when undertaking a risk assessment (RCN 2005). Extrinsic risk factors involved in tissue damage are pressure and/ or shear and can include other variables such as friction and moisture. These risk factors should be removed/diminished by the utilization of appropriate equipment and/or turning regimes planned according to individuals (NHS 2009). Pressure that causes compression and possible capillary occlusion, can lead to tissue ischaemia. The intensity and duration of pressure varies according to individuals’ tissue tolerance Shearing occurs when the skeleton and deep fascia slide downwards with gravity and the upper fascia remain in the original position. This can result in deep tissue necrosis and occurs when patients slide down or are dragged up a bed/chair Friction occurs when two surfaces move across each other and usually involves superficial layers of skin. Mechanical forces and/or poor moving and handling techniques often cause this Moisture such as urine, faeces or wound exudate alters the resiliency of the epidermis to external forces (Beldon et al 2006). Moisture lesions should be differentiated from pressure ulcers. If a lesion is limited to one spot it is likely to be a pressure ulcer, however diffuse superficial areas are likely to be moisture lesions (TVS 2008). To prevent moisture damage, skin should be kept clean, dry and hydrated. Intrinsic Factors include: Acute illness: this may be due to heart failure, vasomotor failure, vasoconstriction due to pain, low blood pressure and temperature changes, i.e. during and after anaesthesia Chronic illness Unstable diabetes Level of consciousness: reduced awareness and /or ability of the need to move to relieve pressure a prolonged pressure is a key factor in pressure ulcer development (NICE 2001) Reduced mobility/immobility is also a key factor in pressure ulcer development due to prolonged pressure (NICE 2003) Medication: eg steroids mimic the ageing process by thinning the skin Sedatives/hypnotics: can cause excessive sleepiness thus reducing mobility Analgesics: can dampen the normal stimulus to move Inotropes: cause peripheral vasoconstriction and tissue hypoxia Non-steroidal anti-inflammatory (NSAID) such as ibuprofen impair inflammatory responses to pressure injury Sensory impairment: neurological disease can reduce sensation, thus insensitivity to pain or discomfort, this results in reduced or lack of stimulus to move to relieve pressure, i.e. patients with diabetes or spinal injuries (Michael & Gillot 1991) Extremes of age: advancing age has increase risk of cardiovascular and neurological problems, changes to elasticity and resilience of skin Neonates and very young children have an increased risk due to maturing skin; however sites and nature of injury may differ. Neonates are morel likely to develop tissue damage in the occipital region (back of head), ears and heels (Michael & Gillot 1991) Vascular disease: reduces total blood flow, impairs the micro-circulation thus increasing the potential for pressure necrosis (NICE 2001) Malnutrition/dehydration: malnutrition can increase risk of multi-organ failure and serious illness. Dehydration may reduce the elasticity of the tissues, thus increasing tissue deformability under pressure or friction. Both obese and emaciated patients are vulnerable to malnutrition (Michael & Gillot 1991) An initial assessment provides a baseline assessment that identifies individual’s level of risk as well as identifying any existing pressure damage. For each episode of their care, all adult patients will undergo a structured risk assessment including a skin assessment, which will be carried out within 4 hours of admission. The Braden Risk Assessment Tool will be used as an aide memoire (Appendix 2) to identify each individual’s level of risk however it does not replace clinical judgement (NICE 2005). Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 8 On admission a patients who have existing pressure ulcers or must have a wound assessment completed indicating the location and grade of the pressure ulcer, photograph taken and appropriate treatments implemented. Reassessment of existing or hospital acquired pressure ulcer wounds must be carried out weekly (Guy 2012). Structured risk assessments and ongoing reassessments is the responsibility of the Registered Nurse and will be undertaken daily or if the individual’s condition changes. The outcome of the risk assessment will enable the Registered Nurse to identify and adjust the strategies needed to prevent and manage pressure ulcers. The outcome of each assessment must be clearly documented in the medical/nursing records if a patient is identified as not at risk. Reassessment must occur if there is a change in the patient’s condition (NICE 2005. Those patients identified, as “at risk” of pressure damage must have an immediate prevention plan initiated (NHS 2009). Patients who have had previous pressure damage must be considered high risk regardless of their Waterlow or Braden score and a prevention plan initiated to reduce the risk of a re-occurrence as scar tissue does not regain full tensile strength, which may result in tissue damage occurring faster. All structured risk assessments must be documented and made accessible to all members of the multi-disciplinary team as accurate documentation provides a record of patient progress. A prevention plan should include details indicating equipment to be supplied (mattress type, foot protectors etc) repositioning and seating regimes, patient advice, etc. 6.1d Skin Inspection The interpretation of signs and symptoms of a skin assessment forms the basis of pressure ulcer prevention and treatment (RCN 2005). Patients identified at risk of developing pressure ulcers should undergo skin inspection on admission and then daily. If the patient’s condition deteriorates, their skin should be inspected at least once during each shift. If a patient’s condition is stable, they should be re-assessed every day throughout hospitalization and inter-hospital transfers. Anti-embolitic hosiery (eg TED stockings) should be removed daily so that heels can be inspected. Reddened areas on an immobile patient can be observed when repositioning occurs. Patients with darker skin should be examined closely as the presence of non-blanching erythema, which appears as a darker area of skin, perhaps with a bruised appearance may otherwise be missed (NICE 2005). Pressure ulcers can also develop under medical devices such as plaster casts, Bipap masks and foot pumps, orthotic devices, and therefore the skin should be inspected when the devices are removed to ensure there is no pressure damage. If a patient is admitted to a ward with a plaster cast, the Fracture Clinic should be contacted. Results of skin inspections should be clearly documented. It is essential that detailed descriptions of any pressure ulcer be recorded including site, size and grade and supported by photographic evidence if possible. Patients admitted with existing pressure ulcers should have undergo a wound assessment on admission and subsequent assessments should be carried out weekly. A skin tolerance test can give an indication of the amount of time tissue can tolerate sustained pressure without damage. Complete a skin tolerance test by: Pressing a finger lightly onto the area the patient has been turned from The skin should blanch (go white) and then return to its normal colour (blanching erythema). This colour return should take no longer than twice the length of the time the pressure was applied for (i.e. 1-2 seconds) indicating an intact micro-circulation (RCN 2005) Signs that may indicate incipient pressure ulcer formation include: Blisters Discolouration Localized heat Localized oedema Localized induration (EPUAP 2009) Pressure ulcers should be graded or categorized using the European Pressure Ulcer Advisory Panel (EPUAP 2009) classification system. Patients who have existing pressure ulcers or who develop pressure ulcers during their hospital stay must have a wound assessment completed indicating the location and grade of the pressure ulcer and Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 9 appropriate treatments implemented. Reassessment of existing or hospital acquired pressure ulcer wounds must be carried out weekly (RCN 2005). 6.1e Positioning and Repositioning Positioning of patients should ensure that prolonged pressure on bony prominences is minimised, bony prominences are kept from direct contact with one another, friction and shear damage is minimized (RCN 2005). Avoid positioning individuals directly on pressure ulcers or bony prominences (commonly the sites of pressure ulcer development) When patients are nursed on a pressure redistributing/relieving device, repositioning should occur to ensure patient comfort, skin inspection, hygiene needs etc. (NICE 2005). The frequency of repositioning of patients should be based on the results of a skin inspection, patient comfort (6.1c) and individual needs; tissue damage can occur as the intensity of pressure can vary with each individual repositioning reduces the duration of pressure and thus the intensity (NICE 2005, RCN 2005, Bryant 2000). A repositioning schedule should take into consideration other aspects of the patient’s condition, i.e. comfort, support, overall plan of care. Individual needs should be identified and appropriate action taken to ensure that regular change of position occurs (Beldon et al 2006). Patients may not tolerate frequent repositioning due to pain; etc therefore further assessment may be required (NICE 2005). A written/recorded re-positioning schedule should be established for every patient “at risk” and this should include actual position changes. To encourage patient independence, reduce the risk of shear and friction forces, whenever possible patents should be encouraged to redistribute their own weight (RCN 2005). Correct lifting and handling techniques reduce the risk of injury to carers and staff so manual handling devices should always be used to minimize shear and friction damage. All handling equipment should be removed after use as equipment left in situ may result in tissue damage (NICE 2005). 6.1f Seating Prolonged seating can cause pressure ulcers especially if patients are immobile or are unable to feel discomfort due to injury or disease (TVS 2008). The physical effects of inappropriate sitting times should be considered. Lower limb pooling and in adequate venous pooling contribute to: Reduced renal perfusion Reduced gut perfusion Reduced cerebral perfusion Development of oedema Development of pressure ulcers Chair sitting should be based on a skin assessment (see 4.1) and limited to no longer than 2 hours at any one time for patients identified ‘at risk’. This will minimise pressure over bony prominences and avoid positioning over existing pressure ulcers (NICE 2003). Immobile patients in a chair are at greater risk of developing pressure ulcers than those patients who remain in bed (NHS 2009). Patients who are immobile or have reduced mobility should not be left sitting in chairs for prolonged periods of time and restricted chair sitting should be incorporated in a repositioning regime (RCN 2005). Poor posture can result in an increased incidence of pressure ulcers therefore a patient’s height, posture, weight etc should be taken into consideration before being sat in a chair (NHS 2009). The use of either an alternating cushion or static cushion should be supplied to patients identified ‘at risk’ or higher and to patients with pressure ulcers (TVS 2008). Attention must be paid to the implementation of pressure relieving/reducing cushions as they may increase the height of the chair, which can be detrimental, as chairs too high will not allow the feet to reach the floor. This will result in increased pressure being exerted through the thighs and buttocks as seated patients take the majority of pressure through the buttocks and thighs (Gebhardt & Bliss 1994). If possible, patients must be encouraged to reposition themselves without causing shear and friction. 6.1g Nutrition There is a clear link between poor nutrition and the development of pressure ulcers (Stephen-Haynes 2006) and regular assessment of patient’s dietary intake enables timely interventions. All adult patients admitted to PHT (excluding Maternity) are screened for their nutritional status and assessed regularly for adequate dietary intake Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 10 using the MUST screening tool. Depending on the outcome of the MUST screen, a relevant management plan should be implemented and evaluated weekly. All patients should have their ability to eat and drink noted on nursing assessment. Patients who require assistance in feeding or whose intake is suspect should be highlighted using a red tray. Nutritional support should be given to patients with an identified nutritional deficiency Guy (2012). Snack boxes, mid morning and afternoon snacks are available for patients who have missed meals etc and supplemental drinks are available at ward level for trained staff to issue for those who are struggling to eat a whole meal. Nursing staff should develop First Line Action Plans for those patients who score 2 above in the MUST screen. Those patients not improving on this score can be referred to a dietician. All patients who are at are at risk of pressure ulcers should be referred to the Dietician if nutritionally compromised (NHS 2009). 6.1h Pressure Relieving Devices As a first line of defense against pressure ulcer damage, high quality, pressure reducing mattresses are used in combination with electric profiling beds. The provision of pressure relieving devices requires a 24 hour approach and this applies to all support surfaces (NICE 2003). Patients identified “not at risk” or “at risk” are suitable to be placed on a foam pressure redistributing mattresses. The use of pressure relieving mattresses should reflect the patients ‘risk’ status (appendix for list of equipment available). All patients with pressure ulcers should have access to appropriate pressure relieving support surfaces and strategies e.g. mattresses, cushions and repositioning 24 hours a day. Patients with either grade 1 or 2 pressure ulcers can be nursed on a high specification foam mattress (NICE 2005) and an electric profiling bed. As a minimum, all patients with grade 3 or 4 pressure ulcers will be placed on an alternating pressure relieving mattress (RCN 2005). Where ever possible, preventative measures must be implemented i.e. surgical patients. A patient’s risk increases during and immediately after surgery therefore equipment must be upgraded following prolonged surgery while the patient is immobilized. Patients with complex needs, including Bariatric patients, may require specialised equipment should be referred to the Tissue Viability Team For specialist advice. The request for equipment should be registered with the Medical Equipment Library and documented in the nursing notes. Whenever equipment is not available or there is a delay in obtaining the requested equipment, reasons for the delay and preventative measures taken should be summarized in the nursing notes and escalated to the Bleep Holder. This action will identify difficulties in accessing equipment resources and also ensure preventative measures have been taken to reduce patient’s risk (Beldon et al 2006). A repositioning regime using the 30-degree tilt combined with regular skin inspection must be undertaken. To ensure the stock of pressure relieving mattresses are utilized effectively and efficiently, patients should be reassessed so that equipment can be downgraded if the patient’s condition improves. To make certain that the patient is nursed safely and receives the optimum pressure relief from equipment used, equipment must be kept in full working order at all times. 6.1i Prevention of heel pressure ulcers The second most common site for pressure ulcers are the heels. Patients with Diabetes are especially vulnerable. All patients with Diabetes must therefore undergo daily foot inspection regardless of their mobility. Some patients may not be able to lift their heels easily to have them inspected. It is recommended that a hand held mirror is used to inspect the heels. When patients with Diabetes are nursed in bed, Repose boots or pillows placed length ways to alleviate pressure under heels must be used. The knee break on the electric profiling should also be used to alleviate pressure under heels. It may not be possible to inspect patients with bandages to legs and/feet on a daily basis so appropriate medical devices designed to off-load pressure, for example Repose boots, to prevent heel damage should be used. When bandages are changed, the feet should be closely inspected to ensure there is no pressure damage. Anti-embolytic stockings should be removed daily and feet inspected to ensure no pressure damage has occurred. Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 11 6.1j Classification of pressure ulcers and Reporting All pressure damage, Grade 1, 2, 3 and 4 pressure ulcers must be reported as a clinical incident. .All pressure ulcers will be categorized or graded using the EPUAP Classification System (see 4). When pressure ulcers are healing they should not be reverse graded, for example: a grade 4 pressure ulcer does not become a grade 3 as it heals. As ulcers heal, they should be described as healing as the original tissue cannot be replaced (NICE 2005). Patients admitted with pressure ulcers: All pressure ulcers present on admission will be assessed and documented within 4 hours and reported as a clinical incident on DATIX system. A photograph of each grade 3 or 4 pressure ulcer must be taken either by the admitting area, Medical Photography or Tissue Viability Nurse. Patients with category or grade 3 and 4 will be reported to Safeguarding Team and referred to the Tissue Viability Team. Hospital acquired pressure damage: All nurses are responsible for reporting if a patient develops pressure ulcers during their hospital stay. A wound assessment will be carried out and plan of care documented. A photograph of each grade 3 or 4 pressure ulcer must be taken either by the admitting area, Medical Photography or Tissue Viability Nurse. A Serious Incident Requiring Investigation (SIRI) will be undertaken if a patient develops a grade 3 or 4 pressure ulcer. The patient will also be referred to the Safeguarding Team and Tissue Viability Team. Deteriorating pressure ulcers: must be reported on DATIX system. A wound assessment must be carried out and plan of care documented. A Serious Incident Requiring Investigation (SIRI) will be undertaken if the pressure ulcer deteriorates to a grade 3 or 4. A photograph of each grade 3 or 4 pressure ulcer must be taken either by the ward, Medical Photography or Tissue Viability. The patient will also be referred to the Safeguarding Team and Tissue Viability Team and a photograph taken. 6.1k Patient and Carer Education To raise awareness of causes of pressure ulcers and inform patients, their families and/carers on prevention strategies and what they can do to help reduce the risk of pressure damage4 and should be provided with a “Pressure Sore Prevention” leaflet on admission. Wherever possible, patients should be encouraged, following education, to inspect their own skin. There are occasions when individuals may refuse pressure ulcer prevention interventions. This should be clearly documented in the medical/nursing notes and the risks explained of non concordance however it may be possible to adapt the strategies to suit the individual. The individual should be referred to the Tissue Viability Team. Patients should also be provided with the Pressure Ulcer Prevention Advisory leaflet. A patient exercise leaflet is available for patients. This exercise leaflet is not suitable for all patients and should only be given to patients at the discretion of the ward staff. 6.1l Preparation for discharge of patients at risk of pressure damage or with existing pressure damage If patients are discharged and still require pressure relieving/reducing equipment at home, a request must be made via the District Nurses at least one week prior to discharge to ensure continuity of care and ensure equipment is available and in situ prior to discharge 6.1m Training All Registered Nurses and Health Care Support Workers undertaking patient assessment must have received appropriate training in the management and prevention of pressure ulcers and also be aware of the limitations of risk assessments tools, and be able to use their professional judgment. All Registered Nurses and Health Care Support Workers should receive appropriate training and keep updated (NHS QIS 2009) and work through competency levels 1-4 as appropriate. To accurately assess the extent of tissue damage, nursing staff must have a sound knowledge in the grading of pressure ulcers and recognize the differences between pressure damage and moisture lesions. To raise awareness and improve clinical practice in all areas, all Registered Nurses and Health Care Support Workers trained in the prevention and management of pressure ulcers should cascade their knowledge and skills in their clinical areas Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 12 6. TRAINING REQUIREMENTS All staff completing risk assessments should have received appropriate training either through the Trust in-house courses facilitated by the Tissue Viability Team or through a suitable tissue viability course specific to pressure ulcer prevention and management. After initial training, competency needs to be maintained by attending refresher up-dates at least every 3 years 7. REFERENCES AND ASSOCIATED DOCUMENTATION 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. BENNETT G, DEALEY C, POSNETT J (2004) The cost of pressure ulcers in the UK Age ageing 33: 230-5 BRYANT R (2000) Acute and Chronic Wounds Nursing Management 2nd Edition Moseby, London BELDON P, COOPER P, WILSON M (2006), Pressure Ulcers Wound Care Essentials Vol 1 pp67-81 DEALEY C, POSSNETT J & WALKER A (2012) Cost of Pressure Ulcers in the United Kingdom Journal of Wound Care Vol 21 No 6 pp261-266 DEFLOOR T, SCHOONHOVEN L, FLETCHER J, et al (2005) Statement of the European Pressure Ulcer Advisory Panel — Pressure Ulcer Classification Differentiation Between Pressure Ulcers and Moisture Lesions. J Wound Ostomy Continence Nursing 32(5): 302–06 DEPARTEMENT OF HEALTH (2010) EUROPEAN PRESSURE ULCER ADVISORY PANEL ((EPUAP) 2009) Pressure Ulcer Prevention: Quick Reference Guide http://www.epuap.org EXPERT PANEL (2009) Skin Changes At Life’s End (SCALE): Final Consensus Document FOX C (2002), Living with a pressure ulcer: a descriptive study of patients’ experiences, British Journal of Community Nursing 7(6; Supplement) S10-S22 GEBHARDT K & BLISS M (1994) Preventing Pressure Sores in Orthopaedic Patients: Is Prolonged Chair Nursing Detrimental? Journal of Tissue Viability Vol 4 No 2 pp51-54 GUY H (2012) The difference between moisture lesions and pressure ulcers Wound Care Essentials Vol 1 pp3644 MICHAEL C & GILLOT H (1991) Macrovascular mechanisms in stasis and ischaemia In Pressure Sores, Clinical and Scientific Approach Bader DL Macmillan London NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE (2005) Pressure Ulcers: The Management of Pressure Ulcers in Primary and Secondary Care: A Clinical Guideline CG029 NICE London NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE (NICE (2003)) Pressure Ulcer Prevention Clinical Guidelines 7 NICE London NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE (2001) Pressure ulcer risk assessment and prevention NICE NHS INNOVATION And IMPROVEMENT (2009) High Impact Actions – Your Skin Matters NHS SOUTH OF ENGLAND (2012) The South of England Quality Improvement Framework for the Prevention and Management of Pressure Ulcers NHS QIS (2009) Best Practice Statement: Pressure Ulcer Prevention NHS Quality Improvement Scotland Edinburgh NIX D , HAUGEN V (2010) Prevention and management of incontinence-associated dermatitis Drugs Aging 27 (6): 491-96 NURSING & MIDWIFERY COUNCIL (2009) Record Keeping Guidance for Nurses & Midwives NMC London ROYAL COLLEGE OF NURSING & NATIONAL INSTITUTE for HEALTH & CLINICAL EXCELLENCE 2005 The Management of Pressure Ulcers in Primary & Secondary Care London NICE STEPHEN-HAYNES J (2006) Implementing the NICE pressure ulcer guidelines, British Journal of Community Nursing in association with Wound Care Society: Wound Care September, S16 - S18 TISSUE VIABILITY SOCIETY (2008) Seating and Pressure Ulcers: Clinical Practice Guideline http://www.tvs.org.uk An Organisation-Wide Policy for the Development and Management of Procedural Documents: NHSLA, May 2007. www.nhsla.com/Publications/ 8. EQUALITY IMPACT STATEMENT Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 13 Portsmouth Hospitals NHS Trust is committed to ensuring that, as far as is reasonably practicable, the way we provide services to the public and the way we treat our staff reflects their individual needs and does not discriminate against individuals or groups on any grounds. This policy has been assessed accordingly All policies must include this standard equality impact statement. However, when sending for ratification and publication, this must be accompanied by the full equality screening assessment tool. The assessment tool can be found on the Trust Intranet -> Policies -> Policy Documentation Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: Version 4 Issue Date: 11/09/2013 (Review date June2015 (unless requirements change) 14 Appendix 1 Moisture Lesions* Pressure Ulcer Incontinence Associated Dermatitis (IAD) Cause Pressure and/or shear must be present Moisture must be present (for example, look for shining, wet skin, caused by urinary incontinence or diarrhoea) Location A wound over a bony prominence is likely to be a pressure ulcer Equipment related – under a device/tube Skin fold (combination) IAD may occur over a bony prominence. However, pressure and shear should be excluded as causes, and moisture should be present Perineum, buttocks, inner thighs, groins Skin folds Shape If the lesion is limited to one spot, it is likely to be a pressure ulcer Circular wound Regular shape Diffuse, different superficial spots are more likely to be IAD Kissing ulcer Anal cleft - linear Depth Partial thickness and full thickness skin loss Superficial (partial thickness skin loss) Necrosis A black necrotic scab on a bony prominence is a pressure ulcer grade 3 or 4. If there is no limited muscular mass underlying the necrosis, the lesion is a pressure ulcer grade 4 No necrosis Edges Distinct edges Diffuse or irregular edges Colour If redness in non blanchable, this is most likely a pressure ulcer grade 1 Blanchable or non blanchable erythema Pink or white surrounding skin due to maceration *Adapted from Defloor et al (2005), Nix & Haugen (2010) Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: (Review date June2015 (unless requirements change) Version 4 Issue Date: 11/09/2013 15 Appendix 2 Braden Risk Assessment Chart Undertake and document risk assessment within 4 hours of admission and then daily. Individuals with a total score of 15-18 are at risk score of 13-14 are at moderate risk score of 10-12 are at high risk score of 9 or below are at very high risk. Patient’s name: ………………………………………………. Sensory Perception – Ability to respond meaningfully to pressure related discomfort 1. Completely Limited Unresponsive (does not moan, flinch or grasp) to painful stimuli, due to diminished level of consciousness or sedation or limited ability to feel pain over most of the body surface. Moisture – Degree to which skin is exposed to moisture 1. Constantly Moist Skin is kept moist almost constantly by perspiration, urine etc. Dampness is detected every time patient / client is moved or turned. 1. Bedfast Confined to bed. Activity – Degree of physical activity Mobility – Ability to change and control body position 1. Completely Immobile Does not make even slight changes in body or extremity position without assistance. Nutrition – MUST score Friction and Shear 1. Very High MUST score >2 1. Problem Requires moderate to maximum assistance in moving. DOB:…………….. Hospital No……………………. Date 2. Very Limited Responds only to painful stimuli. Cannot communicate discomfort except by moaning or restlessness. OR has a sensory impairment that limits the ability to feel pain or discomfort over half of body. 2. Very Moist Skin is often, but not always, moist. Linen must be changed at least once a shift. 3. Slightly Limited Responds to verbal commands, but cannot always communicate discomfort or need to be turned. OR has some sensory impairment that limits ability to feel pain or discomfort in 1 or 2 extremities. 3. Occasionally Moist Skin is occasionally moist, requiring an extra linen change approximately once a day. 4. No Impairment Responds to verbal commands. Has no sensory deficit that would limit ability to feel or voice pain or discomfort. Score 1,2 or 3 Ensure repositioning regime in use and chart. Use pressure relieving mattress, Repose Boots, glide sheets, skin assessments when turned, remove stockings inspect heels daily. 4. Rarely Moist Skin is usually dry. Linen only requires changing at routine intervals. Score 1 or 2 Use a soap substitute for washing, pat dry, apply barrier cream/ film, offer regular toileting, use continence aids, and consider flexi seal for liquid diarrhoea. 2. Chairfast Ability to walk severely limited or non-existent. Cannot bear own weight and / or must be assisted into chair or wheelchair. 2. Very Limited Makes occasional slight changes in body or extremity position but unable to make frequent or significant changes independently. 2. High MUST score =2 2. Potential Problem Moves feebly or requires minimum assistance during a move, skin probably slides to some extent against sheets, chair restraints, or other devices. Maintains relatively good position in chair or bed most of the time but occasionally slides down. 3. Walks Occasionally Walks occasionally during day, but for very short distances, with or without assistance. Spends majority of each shift in bed or chair. 3. Slightly Limited Makes frequent though slight changes in body or extremity position independently. 4. Walks Frequently Walks outside the room at least twice a day and inside the room every two hours during waking hours. Score 1 or2 Ensure patient changes position regularly, use individualised repositioning chart ie 2 hr. turns. Pressure relieving mattress, glide sheets, Repose boots Score 2 or 3 Limit sitting to 1 to 2 hours use dynamic chair cushion 3. Medium MUST score =1 3. No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move. Maintains good position in bed or chair at all times. 4. Low MUST score =0 4. No Limitations Makes major and frequent changes in position without assistance. Score 1,2 or 3 Follow MUST action plan Score 1 or 2 Use profile bed frame, use knee brace to reduce sliding or raise foot of bed 10’ , teach patient to adjust bed, use glide sheets to reposition, reduce sitting time if patient slumps in chair, refer to physiotherapist. Total score Signature Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: (Review date June2015 (unless requirements change) Version 4 Issue Date: 11/09/2013 16 Appendix 3 Pressure Ulcer Prevention Guidance on Pressure Relieving Equipment Allocation of Pressure Relieving Equipment Implement and document pressure ulcer prevention strategy Undertake daily risk assessment or more frequently if change in condition Use Clinical Judgement At High to Very High Risk At Moderate Risk- High Risk At Risk – Moderate Risk Pressure Reducing Foam Mattress Fully mobile No pressure damage Patients with unstable spinal or pelvic injuries Author: Tissue Viability Team April 2013 Pressure Reducing Foam Mattress +/-Repose Mattress* Reduced mobility Underweight Diabetic /+ vascular disease Grade 1 or 2 pressure ulcer (superficial skin loss) Patients with previous pressure damage Seating: 2 hours per session Consider using pressure relieving cushion Repositioning: 2 hourly *Do not use: if patient weight above 19 stone or if patient has plaster cast, external fixator metal work or metal frame in bed Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: (Review date June2015 (unless requirements change) Pressure Relieving Mattress Patients with: Existing grade 3 & 4 pressure ulcers Who have had long lie following fall At risk that weigh 130Kg or more or who are too wide for Repose Immobile patients due to illness or paralysis Multiple underlying health problems Being nursed at home on an air mattress Seating with pressure ulcer: seek Tissue Viability Advice Seating: with no pressure damage: up to 2 hours Use pressure relieving cushions Repositioning: 2 hourly or more frequently depending on individual patient need Version 4 Issue Date: 11/09/2013 17 9. MONITORING COMPLIANCE WITH PROCEDURAL DOCUMENTS This document will be monitored to ensure it is effective and to assurance compliance. Minimum requirement to be monitored Lead Tool Action Plan All relevant Clinical Service Centres will develop and implement Action Plans Senior Nurse Audit of nursing documentation Modern Matron/Ward Manager Patient Records All grade 2, 3 and 4 pressure ulcers are reported as clinical incident Ward Manger DATIX Frequency of Report of Compliance Quarterly Reporting arrangements Policy audit report to: Weekly Monthly Pressure Ulcer Prevention and Management Policy and Associated Guideline for Adults: (Review date June2015 (unless requirements change) Modern Matrons Pressure Ulcer Working Group Policy audit report to: Senior Nurses Pressure Ulcer Working Group Policy audit report to: Lead(s) for acting on Recommendations Risk Department Pressure ulcer Working Group Version 4 Issue Date: 11/09/2013 18