chapter 18-the heart
advertisement

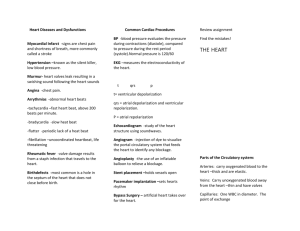
CHAPTER 18-THE HEART I. THE HEART A. The heart serves as the primary pump for the human body. B. The heart pumps blood with its oxygen, nutrients and wastes all over the body. This blood is pumped through miles of blood vessels in the body. II. SIZE, LOCATION AND ORIENTATION OF THE HEART A. The heart is about the size of a fist (weighs less than 1 pound). It is essentially hollow and cone-shaped. B. The heart lies between the lungs in the mediastinum. C. About 2/3rds of the heart is to the left of the midsternal line. The base of the heart is actually located at the top of the heart, the apex of the heart points towards the left hip. III. COVERINGS AROUND THE HEART A. The heart is enclosed and held in place by a double-walled sac known as the pericardium. B. The Pericardium 1. Is composed of 2 layers: a. The Fibrous Pericardium-composed of dense connective tissue. This is a bag that encloses and anchors the heart in place. b. The Serous Pericardium-thin, inner membrane that is composed of 2 layers: 1) Parietal layer-lines the internal surface of the fibrous pericardium. 2) Visceral layer (epicardium)-this layer attaches to the heart muscle (myocardium). 3) Pericardial cavity-space between the parietal and visceral layers. This cavity is filled with serous fluid which prevents friction between the layers as the heart moves. 2. Pericarditis-inflammation of the pericardium. Is caused by bacteria, viruses. a. In this illness, serous fluid production is reduced; therefore, the layers of the pericardium stick together. This restricts heart movements. b. In severe cases, fluid can accumulate around the heart producing a condition known as Cardiac tamponade. A syringe is used to remove the fluid in this case. IV. LAYERS OF THE HEART WALL A. The Epicardium-also known as the visceral layer of the serous pericardium. 1. This is a thin, outer, protective layer around the heart. B. The Myocardium-middle layer. Forms the bulk of the heart wall. 1. This layer is composed of cardiac muscle. 2. This layer also contains a large supply of fibers that provide support and strength to the heart. C. The Endocardium-lines the inside of the heart (including the chambers) and it covers the heart valves. This layer is composed of epithelial and connective tissue. V. HEART CHAMBERS AND IMPORTANT HEART VESSELS A. The heart is composed of 4 chambers: 1. 2 superior atria (which are separated by the interatrial septum). 2. 2 inferior ventricles (which are separated by the interventricular septum). B. 2 grooves on the heart surface indicate the boundaries of the 4 chambers and these grooves contain blood vessels that supply blood to the myocardium. The 2 grooves are: 1. The Atrioventricular Groove (Coronary Sulcus)-encircles the junction of the atria and ventricles. 2. The Interventricular Sulci (anterior and posterior)-separates the ventricles. C. The Atria (singular: atrium) 1. 2 of these: right and left. These are the upper chambers. 2. Auricles-upper appendages of the atria. These increase the volume of the atria. There is one auricle per atrium. 3. Pectinate muscles-small bundles of muscle that line the anterior portion of each atrium. This muscle gives the internal portion of each atrium a rough appearance. 4. Fossa ovalis-depression on the interatrial septum. This marks the spot where the foramen ovale (an opening) existed in the fetal heart. 5. The atria are receiving chambers for blood returning to the heart from the body. They collect blood and then they push the blood into ventricles. 6. Atria are thin-walled since they only push blood into the ventricles. They contribute little to moving blood through the body. 7. Blood returning from the body enters the right atrium through 3 major veins: a. Superior vena cava-returns blood from regions superior to the diaphragm. b. Inferior vena cava-returns blood from regions inferior to the diaphragm. c. Coronary sulcus-collects blood returning from the myocardium itself. 8. 4 Pulmonary Veins carry blood to the heart’s left atrium. These veins carry blood from the lungs back to the heart. This blood is oxygenated blood (this is the only area in the human body where a vein carries oxygenated blood). D. Ventricles-lower heart chambers; these make up most of the mass of the heart. 1. 2 of these: right and left. These are the lower chambers. 2. Trabeculae carneae-ridges of muscle that line the internal walls of the ventricles. 3. Papillary muscles-cone like muscles that project into the ventricular cavity. a. Chord like chordae tendinae extend from the papillary muscles. These attach to and help position the heart valves. 4. The ventricles pump blood to the body; therefore, they are much more muscular than the atria. 5. When the ventricles contract, they push blood out of the heart. a. The right ventricle pumps blood into the pulmonary trunk which routes blood to the lungs where gas exchange occurs. This blood in the pulmonary trunk does not contain oxygen (this is the only artery that carries deoxygenated blood). b. The left ventricle ejects blood into the aorta (largest artery in the body) which carries blood to the body. VI. HEART VALVES A. There are 4 valves in the heart. 1. These ensure that blood flows in one direction through the heart (from atria to ventricles and out of the arteries that attach to the heart). 2. The valves open and close in response to differences in blood pressure on their 2 sides. 3. There are 2 atrioventricular valves and 2 semilunar valves in the heart. B. Atrioventricular (AV) Valves-2 of these; 1 located between each atrium and ventricle. 1. These prevent blood backflow into the atria when the ventricles contract. 2. 2 AV Valves: a. The Tricuspid Valve-consists of 3 flaps or cusps and is located between the right atrium and right ventricle. The flaps are primarily connective tissue. b. The Bicuspid Valve-consists of only 2 flaps and it is located between the left atrium and left ventricle. It is also known as the Mitral Valve. 3. The flaps of the valves are attached to cordlike chordae tendinae that attach to the papillary muscles that line the inside of the ventricles. The chordae tendinae and papillary muscles together control the AV valves. 4. When the heart is relaxed, the AV valves hang down into the ventricular chamber. a. During contraction, pressure rises in the ventricles; thus, forcing the valves to close (the cusps are forced together). The chordae tendinae and papillary muscles anchor the valves in the closed position, which prevents the upward movement of blood. C. Semilunar (SL)Valves-2 of these, located between the ventricles and the major arteries attached to the heart. These prevent blood from back flowing into the ventricles. 1. Each SL valve is composed of 3 half-moon shaped cusps. 2. When the ventricles contract, the blood pushes the SL valves open (against the walls of the arteries). When the ventricles relax, blood in the arteries pushes the valves closed; thus, preventing blood from flowing backwards. 3. The Pulmonary Semilunar Valve and the Aortic Semilunar Valve are the 2 SL Valves. a. Where are these located? D. Valve-Related Disorders 1. Incompetent Valve-the valve does not open and close. Due to this, the heart has to pump the same blood over and over again. This is very inefficient. 2. Valvular Stenosis-valve flaps become stiff and constrict the opening. The heart must work harder in this case. 3. Mitral Valve Prolapse-in about 10% of the population. Most common in young women. In this situation, the flaps become incompetent. There may be a genetic predisposition. Again, this causes great inefficiency in the heart. In most cases, the faulty valves are replaced with synthetic valves or pig heart valves. VII. BLOOD CIRCULATION THROUGH THE HEART A. Circulation Patterns in the Heart: 1. Pulmonary Circulation-carried out by the right side of the heart. In this circulation, blood is pumped to the lungs and back to the left side of the heart. 2. Systemic Circulation-carried out by the left side of the heart. In this circulation pattern, blood is pumped to and from the body. 3. Coronary Circulation-blood flow to and from the heart muscle. B. Events in Blood Circulation Through the Heart 1. Blood enters the right atrium via the superior and inferior vena cava. This is deoxygenated blood. 2. The right atrium contracts. This pushes blood past the tricuspid valve to the right ventricle. Once blood fills the right ventricle, then the tricuspid valve closes to prevent the backflow of blood. 3. The right ventricle contracts to push blood past the pulmonary semilunar valve through the pulmonary trunk(artery) into the lungs. a. In the capillaries of the lungs, the blood gives up carbon dioxide and picks up oxygen. 4. This oxygenated blood returns to the left atrium via the pulmonary veins. a. This ends pulmonary circulation. 5. Next, the left atrium contacts to force blood past the mitral (bicuspid) valve into the left ventricle. Once the left ventricle is filled with blood, the mitral valve closes to prevent the backflow of blood. 6. The left ventricle contracts to force blood past the aortic semilunar valve into the aorta and on to all parts of the body. This is systemic circulation. 7. Coronary Arteries-carry oxygenated blood to the myocardium. These arteries encircle the heart. a. Deoxygenated blood from the myocardium empties into cardiac veins which converge into a large vein known as the coronary sinus which empties into the right atrium. b. This is coronary circulation. C. Disorders associated with blood flow through the heart 1. Angina pectoris-inadequate blood supply to the myocardium. This leads to pain and tightness in the chest and arm. This is treated with nitrates which dilate blood vessels. Stress and/or increased physical demands on the heart can cause this. 2. Ischemia-reduced oxygen supply to the heart. Is caused by stress. Angina pectoris is an example. 3. Myocardial infarction-heart attack or coronary. a. Infarction-death of tissue due to interrupted blood supply. b. This is often caused by a blockage in one of the coronary arteries. The blockage can be caused by a blood clot, fat etc.. c. Can be treated with streptokinase (thru a catheter) which dissolves clots. d. Surgery may also be an option. VIII. PROPERTIES OF CARDIAC MUSCLE FIBERS A. Cardiac muscle is striated and involuntary. It contracts via the sliding filament mechanism. B. Intercalated discs-only in cardiac muscle fibers. These provide support and strength to contracting muscle fibers. C. Cardiac fibers exhibit autorhythmicity, that is, the fibers contract in a coordinated fashion. D. Cardiac muscle fibers contain numerous mitochondria which are involved in ATP production. These mitochondria require oxygen to function properly. IX. HEART PHYSIOLOGY A. The Cardiac Conduction System-ensures that heart contractions (beats) are well-coordinated. 1. In a normal heart beat: the 2 atria contract (while the 2 ventricles relax), then the 2 ventricles contract (while the 2 atria relax). 2. Autorhythmic Cells make up the cardiac conduction system. These cells are localized in the following areas of the heart: a. Sinoatrial node (SA Node) b. Atrioventricular node (AV Node) c. Atrioventricular Bundle (Bundle of His) d. Right and Left Bundle Branches e. Purkinje Fibers 3. Nerve impulses travel over the heart in the structures listed above. The impulses travel through the structures in the exact order listed above. 4. Events in the Cardiac Conduction System: a. Impulses (electrical signals) produce contractions of heart muscle (also known as the beat). b. The Sinoatrial Node (SA Node)-located in the right atrial wall. This structure produces impulses that begin heart muscle contraction. 1) The SA Node is the pacemaker of the heart. It generates about 75 impulses per minute in a resting individual. 2) The impulses produced here spread to both atria. 3) The SA Node also sets the rhythm for the entire heart. It can speed up or slow down heart beat in response to body activity. c. Next, impulses (and contractions) pass to the Atrioventricular Node (AV Node). 1) The AV Node is located in the lower portion of the interatrial septum. 2) At the AV Node, impulses are briefly delayed. This allows the atria to complete their contraction before the ventricles contract. d. From the AV Node, impulses spread quickly to the Atrioventricular Bundle which is located in the inferior portion of the interatrial septum. 1) The AV Bundle is the only connection between the atria and ventricles. e. Impulses then move into and through the interventricular septum via the Right and Left Bundle Branches. f. Purkinje Fibers carry impulses completely through the interventricular septum and to the apex of the heart. 5. Problems/Disorders Associated with the Cardiac Conduction System a. Arrythmias-irregular heart rhythm. This includes: 1) Tachycardia-abnormally fast heart rate; greater than 100 beats/minute. 2) Bradycardia-slow heart rate; less than 60 beats/minute. 3) Some arrythmias can be treated with artificial pacemakers. b. Fibrillation-rapid, irregular and uncoordinated heart contractions. This interrupts blood flow out of the heart. Is treated with electrical shock. c. Ectopic focus-abnormal pacemaker. In some cases, the AV Node will assume control of the heart. d. Heart block-occurs when impulse conduction in the heart is blocked. This can be caused by damage to the AV Node and the AV Bundle. B. Control of Heart Activity 1. The Medulla oblongata controls and regulates much of the heart’s activity. Specifically, the medulla contains: the cardiovascular center and the cardioaccelerating center. C. The Cardiac Cycle-refers to the events that occur during one complete heart beat. 1. In a normal heart beat, the 2 atria contract while the 2 ventricles relax, then the 2 ventricles contract while the 2 atria relax. At the end of the cycle, all of the chambers relax for a moment, then a new cardiac cycle begins. 2. On average, the heart beats 72 times per minute. 3. Key Terms: a. Systole-refers to contraction and emptying of heart chambers. b. Diastole-refers to relaxing and filling of heart chambers. D. Heart Sounds 1. 2 distinct heart sounds: Lubb and Dubb. 2. The sounds are the result of the closing of the heart valves. 3. What produces the heart sounds? a. Lubb-produced by the closing of the atrioventricular valves during ventricular systole. Ventricular pressure is greater than atrial pressure at this point. b. Dubb-2nd heart sound. Occurs at the end of ventricular systole as the semilunar valves close. 4. Heart murmurs-an abnormal heart sound caused by incomplete closing of the valves. a. Stenosis-change in valve shape. E. Electrocardiogram (ECG or EKG)-a measurement of the electrical impulses through the heart. 1. A typical ECG consists of three distinct waves: a. P Wave-1st wave, is very small. This wave is the result of atrial depolarization. 1) The P wave represents atrial contraction. b. QRS Complex-large, results from ventricular depolarization. 1) This represents ventricular contraction. c. T Wave-3rd wave, represents ventricular repolarization. 2. The waves in a normal ECG tend to be very consistent. Any changes indicate heart problems. F. Cardiac Output (CO)-the amount of blood pumped out by each ventricle in one minute. 1. Cardiac output is the product of heart rate (HR) and stroke volume (SV). 2. Stroke Volume-the volume of blood pumped out by a ventricle with each beat. This is related to the force of ventricular contraction. 3. CO= SV X HR a. CO for a normal functioning heart= HR (75 beats/min) X SV (70 ml/beat) =5250 ml or 5.25 L per minute. b. Normal heart volume for an individual is about 5L; thus, the entire blood supply passes through the heart once every minute. 4. Cardiac Reserve-the difference between resting CO and maximal CO. In trained athletes, CO may increase as much as 7X above normal. G. Regulation of Heart Rate 1. Autonomic Nervous System (ANS) a. Nerves from here run to the SA and AV Nodes. b. 2 Divisions of the ANS: 1) Sympathetic Division-under stress or fear, nerves in this division force the release of norepinephrine and epinephrine from the adrenal glands. These two hormones increase SA Node activity; thus, increasing overall heart activity. 2) Parasympathetic Division-reduces heart rate following stress. c. Sensory Neurons play a major role in determining which division is most active in regulating the heart. d. Baroreceptors-in some blood vessels; can respond to blood pressure changes. 1) This forces the brain to adjust SA Node activity as needed. 2. Chemical Regulation-Including: a. Hormones 1) Norepinephrine/epinephrine-from above. 2) Thyroxine-from thyroid gland, regulates overall body metabolism. b. Ions-Including: 1) Calcium Ion-decreased calcium ion levels depresses heart activity (the opposite is also true). 2) Sodium and Potassium Ions-are needed for proper heart functioning. X. HOMEOSTATIC IMBALANCES OF THE HEART A. Tachycardia, Bradycardia-from earlier in notes. B. Congestive heart failure-occurs when the pumping efficiency of the heart is so low that blood circulation is inadequate to meet tissue needs. Can be caused by high BP, atherosclerosis. XI. FETAL DEVELOPMENT OF THE HEART A. The fetal heart has 2 unique structures that disappear prior to birth: 1. Foramen ovale-an opening in the interatrial septum of the fetal heart. Is a hole between the atria. This hole allows blood to bypass the undeveloped lungs. The foramen ovale leaves a remnant known as the fossa ovalis in the adult heart. 2. Ductus arteriosus-opening between the pulmonary trunk and the aorta. Is another lung bypass. This leaves a remnant known as the ligamentum arteriosum on the adult heart. XII. HEART DISORDERS: A. Circulatory Shock-cardiac output is reduced so that body tissues do not receive an adequate blood (oxygen) supply. Symptoms include pale skin, cyanosis. Can lead to organ damage. B. Diagnosing Heart Disorders: 1. Catheterization-catheter is introduced into a blood vessel and worked up to the heart. 2. Echocardiography-use of ultrasound to take pictures of the heart. C. Risk Factors in Heart Disease: 1. High cholesterol 2. High blood pressure 3. Smoking 4. Obesity 5. Lack of exercise 6. Age 7. Genetics 8. Gender 9. Diabetes D. Clinical terms 1. Asystole 2. Cardiac catheterization 3. Commotio cordis 4. Cor pulmonale 5. Endocarditis 6. Heart palpitation 7. Hypertrophic cardiomyopathy 8. Mitral valve prolapse 9. Myocarditis 10. Paroxysmal atrial tachycardia 11. Ventricular tachycardia