CHELSEA & WESTMINSTER HEALTHCARE – CARDIOLOGY
advertisement

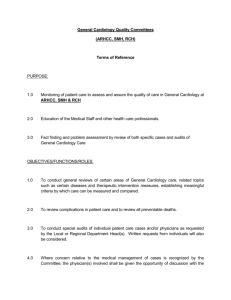
Open access Echocardiology and Heart Failure Cardiology Department Patient Details Name Date of Birth Sex Address Male General Practitioner Detail (or stamp) Name Surgery Address Female Postcode Telephone NHS Number Telephone Fax DATE OF REFERRAL Service Requested Echocardiogram New onset heart failure Priority of referral (please tick one High priority (to be seen A.S.A.P) Low Priority (within 4-6 weeks) Clinical Symptoms/Signs Pulmonary crepitations Raised JVP Other (please specify) Unexplained breathlessness Unexplained oedema Heart murmur Relevant Patient History (Year? ) Smoker Number of units of alcohol per week: Other relevant condition (please specify) MI Hypertension Atrial fibrillation Heart surgery Murmurs Diabetic Family history of heart disease Medication (please tick) ACE Inhibitor Diuretics Other Name Current Past Never Date Results of previous Tests and Investigations Has the patient had an ECG? Yes No If Yes, were the results: Normal? Has the patient had a chest x-ray? Yes If YES, were the results Normal? Abnormal? No Abnormal? Any other relevant information: Please complete this form and return it to: Cardiology Department (next to Outpatient Area 4), First Floor, Chelsea and Westminster Hospital, 369 Fulham Road, SW1O 9NH Telephone: 020 8746 8032 Fax: 020 8746 8038 TO BE COMPLETED BY CARDIOLOGY DEPARTMENT: DATE OF APPOINTMENT: DID PATENT ATTEND? YES NO On arrival of this form, your patient will receive an appointment by telephone or by post (Note: this is not a walk-in service)