Male Medical Screening - Derwent Medical Centre
advertisement

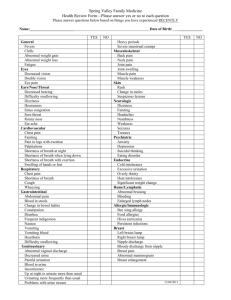
MEDICAL SCREENING Name: Date of Birth: Telephone Number: Email: Please fill this in either adding free text or deleting statements that do not apply to you Please return to Jonathan.Lubin@gp-E83037.nhs.uk Medical Issues and Symptoms: Past Medical History: Family Medical History Current Medication: Smoking: Current smoker Have you ever smoked? How many years smoking Number daily on average Alcohol Intake Units per day (average glass of wine 1U, ½ pint 4% beer 1U, single spirit 1U) Exercise: Frequency of exercise Type of exercise Diet: Allergies: Include drug allergy e.g. penicillin and non drug allergy e.g. animals Other Lifestyle factors: Sleep: Hours per night Quality (do you wake feeling refreshed?) Broken sleep, if so why? SYMPTOMS: Weight: Appetite: GASTROINTESTINAL SYMPTOMS: Symptom: Yes/no Difficulty swallowing/food getting stuck Burning behind sternum/acid in mouth/feeling a lump in throat Dyspepsia or upper abdominal pain after food Bloating or abdominal distension Bowel Frequency Stool consistency Blood in stool Mucous in stool CARDIOVASCULAR SYSTEM Symptoms: Yes/No Chest Pain on Exertion Shortness of Breath on exertion greater than expected Shortness of breath in bed at night Needing many pillows to stop shortness of breath at night in bed Palpitations: Sensation of rapid heart beat Irregular heart beat Extra or missed beats Swelling of Ankles Pain in calves on exertion or walking up hills Do you have any difficulty with maintaining an erection? Details Details RESPIRATORY: Symptoms Cough: Dry Cough: With sputum (include colour) Cough: with blood Wheeze (include time, activities and other causes) Difficulty breathing Shortness of breath Pain breathing Yes/No KIDNEY AND BLADDER Symptoms Yes/No Frequency of passing urine: Daytime Frequency of passing urine: Night Good or poor urine stream? Do you have to wait to pass urine? Does the urine dribble at the end? Is there blood in the urine? NERVOUS SYSTEM Symptoms Faints Fits Headaches Vertigo Loss or reduction in skin sensation Pins and needle, if so where and when Yes/No Details Details Details MUSCULOSKELETAL SYSTEM Symptoms Yes/No Back Pain Radiation of back pain to leg Joint Pain Joint Stiffness Joint Swelling EYES Symptoms Floaters Flashing Lights Eye Pain Eye Irritation EARS/HEARING Symptoms Vertigo Tinnitus Loss of Hearing SKIN Symptom/condition Rashes Moles Other Yes/No Yes/No Details Yes/No Details psoriasis Details Details Medical Examination: Height Weight BMI Anaemia Cyanosis Clubbing Jaundice Lymph Glands: Cervical Lymph Glands: Axillary Lymph Glands: Inguinal CVS: Heart Rate Blood pressure JVP Ankle/leg swelling (oedema) Peripheral pulses Carotid Bruit Femoral Bruit Heart Sounds Varicose Veins ECG RESPIRATORY: Trachea Expansion Percussion note Peak flow Breathe sounds ABDOMEN Soft/hard/firm Masses Tender/Pain Liver Kidneys Spleen Hernias Testis Bowels sounds Rectal examination NERVOUS SYSTEM: Cranial nerves Optic fundi Coordination: Tremor Coordination: Finger to nose Coordination: Dysdiadokinesis Coordination: Rhomberg Coordination: Nystagmus Power: upper limbs Power: Lower limbs Sensation: Light touch Sensation: Pin prick Sensation: Joint position Sensation: Vibration REFLEXES Biceps Triceps Supinator Knee Ankle Plantar LEFT Joints: Cervical spine Thoracolumbar spine Shoulders Hips Knees Functional Assessment Standing on toes Hopping on each foot Kneeling and rising without use of hands Skin: Normal Ears: Examination Audiometry Hospital anxiety and depression test Anxiety /21 Depression /21 RIGHT PATHOLOGY TESTING Urine Glucose Protein Blood Nitrite (urine infection test) Result White cells Blood tests Haemoglobin g/dl Normal Range 13-18g/dl ESR mm/hr <10mm/hr Creatinine umol/l 75-125 umol/l Glucose mmol/l <6.1mmol/l TSH mU/l 0.4-4 mU/l Free T4 Pmol/l Prostate Specific Antigen Free PSA Total mmol/l Cholesterol HDL mmol/l 10-24.5 pmol/l <4ug/L LDL mmol/l 1-5 mmol/l Triglycerides Faecal Occult Blood mmol/l 0.3-2.2 mmol/l <5.7mmol/l 0.9-1.8 mmol/l Ketones SUMMARY AND ACTION PLAN