Analysis of longitudinal data
advertisement

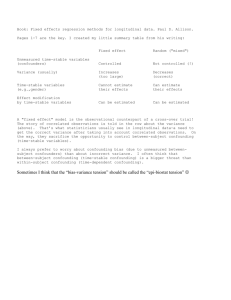
Evaluating the effect of change on change: a different viewpoint Eyal Shahar, MD, MPH Address: Eyal Shahar, MD, MPH Professor Division of Epidemiology and Biostatistics Mel and Enid Zuckerman College of Public Health University of Arizona 1295 N. Martin Ave. Tucson, AZ 85724 Email: Shahar@email.arizona.edu Phone: 520-626-8025 Fax: 520-626-2767 1 Abstract When a causal variable and its presumed effect are measured at two time points in a cohort study, most researchers prefer to fit some type of a change model. Many of them believe that such an analysis is superior to a cross-sectional analysis “because change models estimate the effect of change on change”, which sounds much stronger epistemologically than “estimating a cross-sectional association”. In this article I trace two commonly used regression models of change to their cross-sectional origin and explain that these models do not test anything conceptually different from cross-sectional models. A change model is superior to a cross-sectional model mainly because it corresponds to a self-matched design. Therefore, the main advantage of regressing “change on change” is complete control of time-stable confounders, a key concern in observational studies. Many analysts fail to realize that that important advantage is lost if a random effect model is used. 2 Introduction The most rudimentary example of longitudinal data analysis may be a cohort study where the putative cause and its putative effect are measured twice: at baseline and again some time during follow up. In such cases researchers welcome the opportunity to study “the effect of change on change”, intuitively assuming that longitudinal changes, rather than a cross-sectional association, is a different kind of effect. After all, causal effects are intuitively grasped as “the change in my value of Y, if my value of X were changed”. In this article I suggest that intuition leads us astray. A model of changes between two time points is not testing anything conceptually different from a cross-sectional model, and its key advantage operates in the domain of confounding. Other views are presented as well. To provide a concrete example, rather than use generic notation, I will consider variables from a question of interest to sleep researchers: what is the effect of disordered breathing during sleep (of which sleep apnea is the most severe manifestation) on systolic or diastolic blood pressure (BP)? Although measuring sleep-disordered breathing is a challenge, a commonly used variable is called the respiratory disturbance index (RDI)— the average number of abnormal breathing episodes per hour of sleep. The data structure is simple. In a typical cohort study the RDI and BP are measured twice, several years apart. Time 1 RDI1 BP1 Time 2 RDI2 BP2 3 In the interest of simplified notation, the subscript “i” (indicating the i-th person) is omitted throughout. The first type of a change model To study the effect of the RDI on BP, we may fit two cross-sectional linear regression models, namely, regress BP1 on RDI1 and regress BP2 on RDI2. Most researchers, however, will prefer to fit some type of a change model, the simplest of which is BP2–BP1 = β0 + β (RDI2–RDI1) + ε (Model 1) This change model, however, could be traced to simple subtraction of two cross-sectional models—provided that the effect of the RDI on BP is forced to be identical at both times:[1, page 10] BP2 = μ2 + β RDI2 + γZ + α + ε2 (Model 2) BP1 = μ1 + β RDI1 + γZ + α + ε1 (Model 3) BP2–BP1 = β0 + β (RDI2–RDI1) + ε (Model 1) Where, Z is a vector of confounders whose effect on BP is identical at the two time points. α = all differences between persons that remain constant over time (and are not captured by γZ) β0 = μ2 – μ1 ε = ε2 – ε1 4 Comparing model 1 (the change model) to models 2 and 3, we realize that we haven’t really studied any unique causal idea of change that was missing from the two crosssectional models. The coefficient of the change variable (β)—the so-called effect of change from model 1—is not different from the coefficient of the cross-sectional effect. Notice, again, that we had assumed identical cross-sectional effects of the RDI on BP, which implies no effect modification by time on an additive scale, where “time” is a surrogate for time-dependent variables. So why fit the “change model” instead of fitting two cross-sectional models? As shown above, the key advantage is control of all time-stable confounders (both measured and unmeasured Z variables), which are eliminated by subtracting the crosssectional models.[1, page 10] No cross-sectional model alone offers that important advantage! Interestingly, we may reach the very same conclusion about the control of confounding from the viewpoint of study design, too. The change model is essentially derived from a self-matched cohort design, because we estimate the RDI effect on BP within each person (and then take the average over all people.) Of course, by matching on personal identity, the person-specific estimates of the RDI effect cannot be confounded by any characteristic that has not changed between the two time points, such as gender, ethnicity, and genes. Confounders of the within-subject association (i.e., time-varying 5 confounders) are not eliminated by subtraction. Nonetheless, it may be argued (but cannot be tested) that unknown between-subject confounders usually outnumber, and are perhaps more important, than unknown within-subject confounders. The differences between people at any time are usually more striking than the differences within a person over time. It is perhaps easier to recognize the matching property of the model if the continuous causal variable, RDI, is replaced by a binary (0, 1) variable, say, taking an antihypertensive drug (DRUG). Then, the difference BP2–BP1 for a person who is observed at both DRUG=1 and at DRUG=0 is derived from two BP values that such a person has contributed: once as exposed (DRUG=1) and once as unexposed (DRUG=0). We also see that people who took the drug at both time points, or at neither time point, do not contribute anything to the estimate. Stated differently: the change model in a cohort study may be viewed as the observational counterpart of the randomized crossover trial. In both designs people alternate between at least two exposure values. Finally, notice that the change model has no built-in conditioning. We do not condition the association of RDI2 with BP on RDI1, because both coefficients are forced to have the same absolute value (BP2 – BP1 = β0 + β RDI2 – β RDI1 + ε). From the perspective of causal diagrams,[2] the model simply assumes that RDItBPt (where t=1, 2). 6 The second type of a change model So far we have forced homogeneity of the RDI effect on BP at both times. From a theoretical standpoint, we may often accept that assumption: Why would the effect of the RDI be different at two arbitrary time points, especially when no relevant causal reasoning has dictated the choice of the time points at which these variables were measured? Furthermore, each measured RDI presumably serves as a surrogate for a summary of historical RDI values. Sleep researchers do not assume that the value on a single night determines a contemporaneous blood pressure value. Nonetheless, it is easy to relax the homogeneity assumption and derive a different kind of a “change model”:[1, page 15] BP2 = μ2 + β2 RDI2 + γZ + α + ε2 BP1 = μ1 + β1 RDI1 + γZ + α + ε1 After subtraction: BP2–BP1 = β0 + β2 RDI2 – β1 RDI1 + ε (Model 4) With reorganization of the last equation, we may model BP2 alone as the dependent variable and move BP1 to the right hand side (as part of a person-specific intercept or as an offset variable): BP2 = [BP1 + β0] + β2 RDI2 – β1 RDI1 + ε 7 (Model 5) Again, as we see above the key advantage of this model is control of all time-stable confounders, both measured and unmeasured. But there is more to be said: Since we allowed the effect of RDI2 to differ from that of RDI1, we have also conditioned the associations. This model has four key properties: 1) The association of RDI2 with BP2 is conditional on RDI1 2) The association of RDI1 with BP2 is conditional on RDI2 3) Both conditional associations control all time-stable confounders 4) The coefficient of RDI1 (namely, β1) may be biased! In particular, if RDI1 affects RDI2 A causal diagram perspective of model 5 To understand the fourth property of model 5, we should recall two principles of directed acyclic graphs (causal diagrams):[2, 3] 1) The marginal association between two variables reflects causal paths between them (the effect of interest) and back-door paths (confounding). 2) Conditioning on a common effect of two variables (a collider) creates an association, or contributes to the association, between the colliding variables. Figure 1 shows a possible, realistic, causal diagram according to which RD1 affects RDI2 whereas RDI1, RDI2 and BP2 share a common cause, U (a confounder of the effect of RDI on BP2.) A causal chain from RDI1 to BP2 via BP1 is also depicted. 8 U RDI1 RDI2 BP2 BP1 Figure 1. A theoretical causal diagram for RDI and BP, when measured at two time points. There are two reasons why we should not condition on RDI2 when we try to estimate the effect of RDI1 on BP2: First, part of the effect of RDI1 on BP2 is mediated via RDI2. Conditioning on an intermediary variable on a causal pathway eliminates some of the total effect, which is unwise. Second, since RDI2 is a collider on a path from RDI1 to BP2 (via U), conditioning on RDI2 violates a key rule of directed acyclic graphs for estimating effects,[3] because it opens a non-causal associational path between RDI1 and BP2 (RDI1—UBP2). Therefore, when heterogeneity of the two cross-sectional associations is allowed, we should ignore the coefficient of RDI1. Only the coefficient of RDI2 is informative (assuming no important within-person confounding). So what do we gain from allowing such heterogeneity? Or in other words: what do we gain from conditioning the association of RDI2 with BP2 on RDI1? We may gain the blocking of confounding paths via RDI1, such as the back-door path (thick arrow) that is shown in Figure 2. If a high value of BP1 has triggered the prescription of an antihypertensive medication (MED), 9 which in turn has affected BP2, conditioning the association between RDI2 and BP2 on RDI1 should block this confounding path. When we regress BP2 on RDI2 alone (a crosssectional association at time 2), this confounding path remains open. RDI1 RDI2 BP2 MED BP1 Figure 2. A theoretical causal diagram according to which the cross-sectional association of RDI2 and BP2 contains confounding by RDI1 Other views Textbooks on longitudinal data analysis recognize, of course, the benefit of change models for the controlling of time-stable confounders, but they apparently follow the assumption that “a longitudinal effect” is a different causal idea from “a cross-sectional effect”. For example, the authors of one book [4] seem to suggest conceptual difference between what they call βC (the cross-sectional effect; my β1) and what they call βL (the effect of longitudinal change according to their parameterization; my β2). The following citations illustrate their viewpoint: “…the prime advantage of a longitudinal study is its effectiveness for studying change.”[4, page 17] 10 “…the major advantage of a longitudinal study is its ability to distinguish the crosssectional and longitudinal relationships between the explanatory variables and the response.”[4, page 23] Like others, these authors acknowledge the benefit of controlling time-stable confounders and recommend conditioning on the baseline causal variable: “…one may simply view Xi1 [my RDI1] as a confounding variable whose absence may bias our estimate of the true longitudinal effect [my β2, the coefficient of RDI2].”[4, page 24] It appears that the effect that is confounded in their mind is “the true longitudinal effect”. As shown here, however, that longitudinal effect is simply the cross-sectional effect at time 2, after controlling for all time stable covariates and the baseline causal variable. The opportunity to partition the total variance into within-person and between-person components has led statisticians to propose another parameterization of longitudinal data.[5] The pertinent expression (for the i-th subject) takes the following form: BPt = βt + βwithin (RDIt – mean RDI) + βbetween (mean RDI) + γZ + α + εt where t=1, 2 Those who proposed that parameterization tell researchers to estimate two kinds of exposure effects in longitudinal studies:[5] “an overall effect of age [here, RDI] on response [here, BP]” as estimated by the coefficient βbetween, and “the effects of deviations 11 from the average age [here, RDI]” as estimated by the coefficient βwithin. Furthermore, they argue that researchers typically fail to distinguish between these two kinds of effects, and that models that incorrectly assume βbetween = βwithin “can lead to very misleading assessments of the association of covariates with response”.[5] Indeed, one of these associations, or both, could be misleading, but “association” is not synonymous with “causation”, and causation is not partitioned into causation by “mean RDI” and causation by “deviation from mean RDI”. If the idea of different causal effects were valid, we should have never compared, for example, the estimated effect of a drug from a parallel group trial (“between-patient effect”) to the estimated effect of that drug from a cross-over trial (“within-patient effect”). Moreover, if the idea were valid, analysts of cross-over trials would have regularly reported “both kinds of effects” (because the “between-patient effect” can also be estimated from that design). Evidently, they don’t. In the absence of time-dependent confounders (i.e., within-subject confounders), the difference between βbetween and βwithin in a non-randomized study may be easily explained by unknown between-subject confounders, although competing explanations are always possible.[6] Moreover, typical multivariable methods to estimate these coefficients, such as a random-effect model and GEE, often sacrifice the controlling of all time-stable confounders for the return of a smaller standard error of β—a classical trade-off between bias and variance.[7] But epidemiologists who realize the last point would rarely be sympathetic to the trade-off. In the absence of within-subject confounding, they don’t 12 usually care about optimal use of a covariance matrix that will minimize the standard error—of a confounded estimator of effect. Finally, in another textbook on applied longitudinal data analysis, the authors dismiss altogether the studying of change between two time points “because two-wave studies…confound true change with measurement error.”[8, page 10] Apparently, the key benefit of two wave studies—controlling of all time-stable confounders—is not deemed that important to these authors. As we see, statisticians speak in many voices about the meaning and interpretation of change models. Conclusion The two models of the effect of change in RDI on change in BP simply estimate coefficients of cross-sectional associations. They offer control of time-stable confounders, which is not offered by any isolated cross-sectional association, and that’s the main reason for preferring these models—whenever we assume that unknown withinsubject confounding is a much smaller threat than unknown between-subject confounding (unfortunately, an untestable assumption). That important advantage is usually lost if a random effect model is used. If heterogeneity of the cross-sectional associations is allowed, then only the coefficient of RDI2 should be reported, and in that case, we are also controlling all confounding paths 13 via RDI1. Most important, and contrary to prevailing thought, a model of changes between two time points does not estimate any special causal idea called “longitudinal effect”. 14 References 1. Allison PD. Fixed effects regression methods for longitudinal data using SAS. Cary: SAS Institute Inc. 2005. 2. Greenland S, Pearl J, Robins JM. Causal diagrams for epidemiologic research. Epidemiology 1999;10:37-81 3. Hernán MA, Hernández-Diaz S, Robins JM. A structural approach to selection bias. Epidemiology 2004:15:615-625. 4. Diggle PJ, Liang K-Y, Zeger SL. Analysis of longitudinal data. New York: Oxford University Press, 1995. 5. Neuhaus JM, Kalbfleisch JD. Between- and within-cluster covariate effects in the analysis of clustered data. Biometrics 1998;54:638-645. 6. Mancl LA, Leroux BG, DeRouen TA. Between-subject and within-subject statistical information in dental research. J Dent Res 2000;79:1778-81. 7. Palta M, Yao T-J. Analysis of longitudinal data with unmeasured confounders. Biometrics 1991;47:1355-69. 15 8. Singer JD, Willett JB. Applied longitudinal data analysis: modeling change and event occurrence. New York: Oxford University Press, 2003. 16