Urinary Tract Infection: Providing the Best Care
advertisement

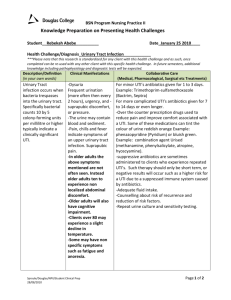
Urinary Tract Infection: Providing the Best Care Introduction Urinary tract infections (UTIs) account for more than 8 million office visits per year and as many as 100,000 hospitalizations. Although UTIs are typically thought to be easy to detect and cure, a number of factors must be taken into account to provide the most appropriate and effective care. Recommendations on the diagnosis and treatment of this common infection vary according to patient's age and sex as well as comorbidity, level of risk of infection with resistant pathogens, previous response to therapy, the use of a urinary catheter, and pregnancy. [1] The choice of antimicrobials has increased, as has the prevalence of resistant pathogens. Those involved in the care of patients who have a UTI are faced with a number of questions: What causes this common clinical condition? How can it be prevented? What is the optimal clinical evaluation? Which antimicrobials should be used empirically, and which should be avoided? Do the antimicrobials long used in the treatment of UTI, such as nitrofurantoin and trimethoprim-sulfamethoxazole (TMP-SMX), still have a role to play in the age of resistant organisms? And when should newer agents such as the fluoroquinolones be used? Recognizing the Clinical Presentation The urinary tract, adjacent to the bacteria-rich lower gastrointestinal tract, produces and stores urine. The periurethral area is typically colonized with gut and other flora, some capable of causing UTI.[2] While the process of urination flushes bacteria from the urethral orifice, periurethral pathogens on occasion enter the urethra and ascend, reaching the bladder and resulting in UTI; this is the most common route for UTI acquisition. On rare occasion, hematogenous UTI can occur when a pathogen is delivered to the urinary tract via the bloodstream from a distant source of infection, such as the lungs in a patient with pneumonia.[3] Urinary tract infections can involve mucosal tissue (cystitis) or soft tissue (pyelonephritis, prostatitis). Anatomically, the infection can be limited to the lower urinary tract (cystitis involving the bladder and urethra) or the upper tract (pyelonephritis). Complicated UTI can occur in either the upper or lower urinary tract but is accompanied by an underlying condition that increases the risk for failing therapy, such as obstruction, urologic dysfunction, or resistant pathogens. Most UTIs occur via an ascending route.[4] UTI is typically diagnosed by clinical presentation and a limited number of physical exam findings. In the otherwise healthy woman, history of the present illness usually reveals a complaint of dysuria, often reported as an internal discomfort, with urinary frequency and urgency but without fever or constitutional symptoms. Although suprapubic tenderness and pain are often considered part of the clinical presentation, they are only found in about 20% of women with an uncomplicated UTI. Back pain, fever, nausea, and vomiting are more often associated with pyelonephritis, and rarely with cystitis; many with pyelonephritis will also report lower UTI symptoms. While vaginal infection and irritation can cause dysuria, most women who have dysuria without vaginal discharge have a UTI, not vaginitis.[5] In urethritis, the inflammation and infection is limited to the urethra only, or urethra and vagina in women; its etiology is usually a sexually transmitted pathogen such as Chlamydia trachomatis, Ureaplasma urealyticum, Neisseria gonorrhoeae, or Trichomonas vaginalis.[6] Found in men and women, complaints include discomfort during voiding, but there are usually no symptoms of postvoid suprapubic pain or urinary frequency. Hemorrhagic cystitis is characterized by large quantities of visible blood in the urine. Its etiology can be bacterial or adenovirus types 1-47 infection or as a result of radiation, cancer chemotherapy, or select immunosuppressive medication. Clinical presentation usually depends on its origin; with all causes, irritative voiding symptoms are typically reported. When infectious in origin, signs and symptoms of infection may also be encountered. Adenovirus is a common cause and is self-limiting in nature. Hemorrhagic cystitis is often confused with glomerulonephritis, but hypertension and abnormal renal function are absent in the former. When radiation-induced, symptoms may develop months after cessation of treatment.[7,8] Acute pyelonephritis is an infection of the renal parenchyma and renal pelvis, caused by an ascending cystitis; most episodes are uncomplicated and not accompanied by risk of treatment failure such as obstruction, urologic dysfunction, or a multidrug-resistant uropathogen.[4] Irritative voiding symptoms similar to cystitis are usually reported, along with fever and flank pain, often with vomiting. Clinical findings usually include an acutely ill appearance, costovertebral tenderness, and pyuria. Table 1 outlines the clinical findings in women with dysuria and pyuria. Table 1. Clinical Findings in Women With Dysuria and Pyuria [3,9] Clinical Findings in Addition to Dysuria Possible and Pyuria Etiology Comment Suprapubic tenderness, pelvic discomfort especially pre- and immediately postvoid, urinary urgency and frequency, small volume voiding, hematuria (micro or macroscopic). Cystitis, lower urinary tract infection Gram-negative bacilli (Escherichia coli, Proteus, Klebsiella, others), select Gram-positive organism (Staphylococcus saprophyticus). Flank pain, fever, CVA tenderness, nausea and vomiting, bacteremia; suprapubic tenderness, urinary urgency and frequency present or absent. Pyelonephritis Pathogenic organisms revealed by urine culture include Gramnegative bacilli (E coli, Proteus, Klebsiella, others). Kidney stones and obstructive uropathy may be contributors. Urethral, vaginal discharge in the absence Urethritis of suprapubic pain or tenderness, urinary frequency, urgency, fever; numerous white blood cells found on microscopic wet mount examination of vaginal discharge Most common as sexually transmitted infection such as Chlamydia trachomatis, Niesseria gonorrhoeae, Trichomonas vaginalis Irritative voiding symptoms, purulent or mucopurulent vaginal or cervical discharge, report of postcoital bleeding, edema and/or erythema of cervix or cervical os, brisk bleeding induced by endocervical swabbing, numerous white blood cells found on microscopic wet mount examination of vaginal discharge Mucopurulent cervicitis N gonorrhoeae, C trachomatis, others. Irritative voiding symptoms, purulent or mucopurulent vaginal or cervical discharge, fever, abdominal pain, edema and/or erythema of cervix or cervical os, brisk bleeding induced by endocervical swabbing, cervical motion tenderness, Pelvic inflammatory disease N gonorrhoeae, C trachomatis, E coli, micro-organisms that normally comprise vaginal flora (anaerobes, Helicobacter influenzae, enteric Gram-negative rods, Streptococcus agalactiae), Mycoplasma and Ureaplasma species, others. possible evidence of tubal-ovarian mass, numerous white blood cells found on microscopic wet mount Selecting Laboratory Tests Laboratory testing has traditionally been used to support the diagnosis of UTI. Urine sampling for diagnostic testing is obtained through midstream voiding. A midstream urine sample can be used for dipstick, microscopic urinalysis, and urine culture. Urine dipstick testing is commonly done in the office setting when UTI is suspected because it is simple and convenient and yields immediate results. Leukocyte esterase, nitrates, protein, and blood are the important features in evaluating for UTI. The presence of leukocyte esterase on a urine dipstick is equivalent to >/= 4 white blood cells per high-power field (WBC/hpf). Nearly all (>/= 96%) patients with UTI have pyuria equivalent to > 10 WBC/hpf.[5] Some uropathogens are capable of reducing dietary nitrates in the urine to nitrite; this is an indirect test for bacteriuria. When coupled with a leukocyte esterase response, the likely offending organism is a Gram-negative pathogen (Escherichia coli, Proteus spp., Klebsiella pneumoniae). The nitrite test may be falsely negative in UTI with a low colony count, or in recently voided or dilute urine. In addition, this test does not detect organisms unable to reduce nitrate to nitrite, such as enterococci, staphylococci, or adenovirus.[10] Small amounts of protein and red blood cells may also be positive on dipstick in cases of UTI. Table 2 highlights common urinalysis dipstick findings in UTI. However, in one study of healthy young adult women with dysuria for less than 1 week without vaginal discharge, signs of pyelonephritis, or predisposing conditions, empiric therapy guided by clinical presentation alone was the most cost-effective strategy; culture and treat-later strategies were significantly more expensive, and use of the dipstick alone was the most expensive approach.[11] Further prospective clinical trials will be helpful in establishing the most cost-effective and clinically effective strategy, including patient-directed therapy. Table 2. Common Urinalysis Dipstick Findings in Urinary Tract Infection [12,13] Finding Significance Comment Color Typically pale yellow to colorless Change in urine color is not synonymous with urinary tract infection (UTI) or disease. Clarity Typically clear Pyuria causes urinary turbidity Odor Mild characteristic odor Rancid or ammonia odor in urea-splitting organism Specific Dilute urine = SG </= 1.008 gravity (SG) Concentrated urine = SG > 1.020 Dilute or concentrated urine may influence the results of urine chemstrip testing. Leukocyte esterase (LE) Positive results indicated presence of neutrophils > 4 WBCs/hpf, an indicator of UTI, reported sensitivity of 75% to 90%. Results not valid in neutropenic patient. Decreased sensitivity with increased urinary glucose concentration, high urinary SG, and presence Test for enzyme present in white blood cell (WBC) of antimicrobial in urine. Nitrites Surrogate marker for bacteriuria. Presence indicates bacterial reduction of dietary nitrates to nitrites by select Gram-negative uropathogens including Escherichia coli, Proteus spp. Normally absent in sterile urine and infection caused by enterococci, staphylococci. Best done on well-concentrated urine such as first AM void. For nitrites to be present, urine should be held in bladder for >/= 1 hour for nitrate-to-nitrite conversion to take place; dietary nitrate intake must be adequate. False negative possible with low colony-count infections. Protein Dipstick testing most sensitive for albumin Common in febrile response or represents presence of protein-containing substance such as white blood cells, bacteria, mucous. In UTI, usually trace to 30 mg/dL (1+), seldom >/= 100 mg/dL. pH Average pH = 5-6 Acid pH = 4.5-5.5 Alkaline pH = 6.5-8 If alkaline urine is found in presence of UTI symptoms and positive leukocyte esterase, likely urea splitting such as Proteus, allowing urea to be split into CO2 and ammonia, causing a rise in the urine's normally acid pH. Red blood cells (RBCs) Low number of RBCs noted. Microscopic hematuria common with urinary Gross hematuria may occur in tract infection but not in urethritis or vaginitis. uncomplicated UTI but may be present in infection complicated by nephrolithiasis Microscopic urinalysis can be used to confirm UTI but requires additional equipment and considerable technical skill if done in the office, or delay in time if performed in a laboratory. When coupled with classic symptoms, a finding of 2-5 WBCs or >/= 15 bacteria per hpf in a centrifuged urine sediment is consistent with UTI.[10] The presence of many epithelial cells usually indicates a contaminated specimen. Urine culture is important when diagnosis is not clear or UTI is recurrent. The presence of more than one organism may indicate a contaminated urine specimen and collection and testing should be repeated. The presence of >/= 105 CFU/mL of bacteria is the traditional diagnostic indicator for UTI. However, in the presence of dysuria and other symptoms for UTI, 102 CFU/mL confirms the diagnosis. Approximately 10% to 20% of women with acute uncomplicated pyelonephritis will have blood cultures positive for the offending pathogen. However, this is not predictive of a poorer outcome or need for protracted length of treatment in the otherwise healthy woman. While typically obtained when a patient pyelonephritis needs to be hospitalized, obtaining blood cultures will likely be of benefit only when there is evidence of complicated infection, multidrug-resistant pathogen or treatment failure.[4] What Factors Determine the Risk of UTI? Certain factors protect against or increase the risk for UTI. Male sex is recognized as a potent protective factor, in part due to the longer urethral length compared with women. In addition, certain women with a closer proximity of the urethral orifice to the anus appear to be at increased UTI risk.[14] In addition, the scrotum provides a physical barrier between the glans and the perianal region, a potential source of uropathogens. Unlike the periurethral area in women, the male periurethral area does not support bacterial growth. Zinc-rich prostatic secretions are antibacterial, further discouraging pathogen growth.[15] In women, the intestinal tract or periurethral area becomes colonized with uropathogens. Once colonization occurs, the organisms may remain in place, whether or not these cause a urinary tract infection. In either sex, efficient bladder emptying helps prevent urine stagnation and minimizes UTI risk. Factors that can alter efficient bladder emptying, such as cystocele, rectocele, and benign prostatic hyperplasia (BPH) increase UTI risk. In addition, robust fucosyltransferase activity discourages bacterial adherence; the presence of relatively few bacterial adhesion receptor sites in the bladder and urethra acts similarly. Women with these receptors who do not have mucosal secretion of the fucosyltransferase enzyme to help block bacterial adherence are more likely to have colonization of E coli and other coliforms from the rectum and less likely to have lactobacilli in the periurethral area, resulting in frequent episodes of cystitis. The uroepithelial receptors can also be found in the upper urinary tract, increasing the risk of pyelonephritis. [6] Women who are nonsecretors of ABH blood group antigens show enhanced adherence of uropathogenic E coli to uroepithelial cells compared with women who are secretors; this becomes a major UTI risk factor when coupled with spermicide use or frequent vaginal sexual intercourse. [16] The woman who is exposed to the spermicide nonoxynol-9, either through vaginal use or with a male partner who uses condoms with this spermicide, is at increased risk of UTI. The proposed mechanism of this risk is due to the spermicide's antibacterial effect, reducing lactobacilli, a normal component of the periurethral flora. Lactobacilli produce hydrogen peroxide and lactic acid, providing the periurethral area and vagina with a pH that inhibits bacterial growth and blocks potential sites of attachment, as well as being toxic to uropathogens. [17] Recent studies also propose that spermicides containing the antibacterial detergent benzethonium chloride, often used as a preservative, may contribute to this problem. Although often recommended, voiding at regular intervals, wiping patterns, and postcoital voiding have not been proven to provide uncomplicated UTI protection[14,18]; hot tubs, pantyhose, douching, and obesity have not been demonstrated to increase UTI risk.[14] In postmenopausal women, estrogen deficiency leads to a marked reduction in lactobacilli colonization in the vaginal-perineal areas; topical estrogen use results in reestablishment of the normal protective flora and a reduction of UTI risk.[17] Recent antimicrobial use potentially increases UTI risk by the same mechanism.[14] The replenishment of urogenital microflora with probiotics or exogenous application of protective, "friendly" bacteria, via vaginal douche or capsule or taken orally in capsules, drinks, or yogurt, is gaining popularity for genitourinary tract infections.[19] In children and elders, constipation has been noted to contribute to bladder instability and may encourage UTI.[20] Elders often have a number of risk factors for UTI, including alterations in urinary tract structure such as uterine prolapse, cystocele, rectocele, and BPH, and limited functional status impairing mobility, hygiene, and toileting. [20] UTI in Special Populations Most uncomplicated UTIs occur in women of reproductive age who otherwise do not have chronic health problems or voiding disorders; assessment is often straightforward and treatment is effective. However, certain populations, including elders, pregnant women, and people with clinical conditions such as asymptomatic bacteriuria, bear special mention. Asymptomatic Bacteriuria Asymptomatic bacteriuria, in which urine culture reveals a significant growth of a pathogen (> 10 5 bacteria/mL)[20] but the patient has no symptoms of UTI, can be found at equal rates in pregnant and nonpregnant women during the reproductive years. Incidence increases with age. Asymptomatic bacteriuria is noted in approximately 20% to 25% of community-dwelling women age 65 and older and in around 10% of community-dwelling men age 65 and older. In the nonpregnant woman of reproductive age or the well elder, asymptomatic bacteriuria poises no health threat and should only be treated if bladder instrumentation or surgery is planned. In fact, treatment may result in the development of resistant organisms. A course of an appropriate antimicrobial is indicated if bladder instrumentation is planned.[10,21] The incidence of asymptomatic bacteriuria among elders residing in long-term-care facilities increases to 20% to 50% for those without an indwelling urinary catheter, but virtually all with an indwelling catheter have bacteriuria. Risk factors for bacteriuria in the elderly include altered elimination (fecal impaction and the use of medications that encourage constipation and urinary retention such as anticholinergic drugs), anatomic variations in the urinary tract (cystocele, BPH), hygienic issues (fecal soiling, poor perineal hygiene), neurologic impairment affecting mobility and bladder emptying, and postmenopausal hormonal changes. In the person with an indwelling urinary catheter and evidence of sepsis, bacteriuria should be treated.[18] Cunha proposes the following formulas to assist with the differentiation between UTI and bacteriuria: pyuria alone = inflammation; bacteriuria without pyuria = colonization; pyuria + bacteriuria + nitrites = infection. [22] Symptomatic UTI in the Elderly The healthy elder with an uncomplicated lower UTI, regardless of gender, is likely to have a classic presentation including urinary frequency, urgency, and suprapubic discomfort; new-onset urinary incontinence may also be reported. The frail elder with multiple health problems and complicated UTI may have an atypical or subtle presentation of infection, including change in appetite, delirium, and agitation. An elder with urinary incontinence and UTI may experience an increase in the number of episodes of urine loss.[20,22] UTI and Asymptomatic Bacteriuria During Pregnancy Pregnancy-related anatomic changes in the urinary tract, such as pressure on the bladder from enlarging uterus and increase in the size of the ureters, contribute to urinary reflux. UTI in the pregnant woman is a significant risk factor for low-birthweight infants and prematurity. Asymptomatic bacteriuria occurs in 5% to 9% of both nonpregnant and pregnant women. If left untreated in pregnancy, progression to symptomatic UTI including acute cystitis and pyelonephritis occurs in 15% to 45%, or 4-fold higher than in nonpregnant women. This is due largely to the lower interleukin-6 levels and serum antibody responses to E coli antigens that occur during pregnancy, resulting in less robust immune response. Since asymptomatic bacteriuria, usually caused by aerobic Gram-negative bacilli or Staphylococcus haemolyticus, can lead to UTI, a urine culture should be obtained from all women early in pregnancy, even in the absence of UTI symptoms.[10] Approximately 20% to 40% of women with bacteriuria will develop UTI during the course of the pregnancy; only 1% to 2% of those with a negative urine culture develop UTI. Bacteriuria should be treated with a 3- to 7-day course of antimicrobials, which reduces the risk of symptomatic UTI by 80% to 90%. [10,21] Therapeutic options for the treatment of asymptomatic bacteriuria and symptomatic UTI during pregnancy are guided by pathogen susceptibility, and preferred antimicrobials include those with US Food and Drug Administration (FDA) pregnancy risk category B. Table 3 identifies FDA pregnancy risk and Hale's lactation risk categories for commonly prescribed antimicrobials in UTI. Antimicrobials in pregnancy risk category B include the beta-lactams (amoxicillin, cephalexin, cefpodoxime, cefixime, and amoxicillin/clavulanate) and nitrofurantoin. Nitrofurantoin has the advantage of sparing disruption of normal vaginal flora and consistent efficacy against E coli and Staphylococcus saprophyticus. Nitrofurantoin should be avoided after the 36th week of gestation due to the potential (though unlikely) risk for hemolysis if the fetus is G6PD-deficient and in infections caused by Proteus mirabilis. Beta-lactam use usually fails to eradicate the offending pathogen from the periurethral and perivaginal area, increasing the risk of reinfection. Table 3. FDA Pregnancy Risk and Hale's Lactation Risk Categories for Commonly Prescribed Antimicrobials in Urinary Tract Infection Cat B, L1, L2 Cat C, L3 Cat D, L3 Nitrofurantoin Amoxicillin with clavulanate Amoxicillin Cephalosporins Fluoroquinolones TMP-SMX Doxycycline Lactation Risk Category[23] L1 -- Safest, controlled study = Fails to demonstrate risk L2 -- Safer, limited number of woman studied without risk L3 -- Moderately safe, no controlled study or controlled study shows minimal, nonlife-threatening risk L4 -- Hazardous, positive evidence of risk, may be used if maternal life-threatening situation L5 -- Contraindicated, significant, and documented risk FDA Pregnancy Risk Categories[23] Category A Category B Category C Category D Category X Wellcontrolled human study = no fetal risk in first trimester. No evidence of risk in second, third trimesters. Risk to fetus appears remote. Animal studies do not demonstrate fetal risk but no controlled study in humans. OR Animal studies show adverse effect but not demonstrated in human study. No controlled study in humans available. Animals reveal adverse fetal effects. Positive evidence of human fetal risk. Use in pregnant woman occasionally acceptable despite risk. Animal or human studies demonstrate fetal abnormality. Evidence of fetal risk based on human study. No indication in pregnancy. The fluoroquinolones and TMP-SMX are FDA pregnancy risk category C; TMP-SMX is also associated with a higher risk of treatment failure due to resistant pathogens. [6] Women with symptomatic UTI during pregnancy should be treated for 7 days, and asymptomatic bacteruria is usually treated for 3 days. Once UTI is documented, monthly screening urine cultures should be obtained for the duration of the pregnancy. Daily antimicrobial prophylaxis with an appropriate agent should be considered with evidence of 2 days of a symptomatic UTI or persistent, unresolved bacteruria, in spite of effective antimicrobial therapy. Urologic evaluation should also be considered to rule out structural abnormality.[10,21] UTI in Men UTI is often thought to be rare in men, but it is the most common cause of male dysuria. It typically occurs during the first 3 months of life or after age 50 years. Potential obstruction to urine flow may be caused by the foreskin in early life and by the prostate in mid and later life.[24] The male presenting with fever, dysuria, and back pain should be evaluated for acute bacterial prostatitis or pyelonephritis; a urology referral should be considered with any male UTI. Table 4 reviews the clinical findings in men with dysuria and pyuria.[25] Asymptomatic bacteriuria in the older man should not be treated unless bladder instrumentation, surgery, or prostatic massage is planned.[21] Table 4. Clinical Findings in Men with Dysuria and Pyuria [25] Clinical Findings in Addition to Dysuria and Pyuria Possible Etiology Comment Back pain, fever, CVA tenderness, nausea and vomiting, bacteremia Pyelonephritis Consider urinary tract obstructive process such as BPH, stones. Pathogenic organisms revealed by urine culture include Gram-negative bacilli (Escherichia coli, Proteus, Klebsiella, others) Back pain, fever, arthralgia, myalgia, rectal pain obstructive voiding symptoms, tender, boggy prostate Acute prostatitis Urine culture reveals pathogenic organisms (E coli, Proteus, Klebsiella, others) Scrotal swelling and redness, fever, epididymal tenderness Acute epididymitis Pyuria rate = approximately 25%. May be caused by sexually transmitted organism (Chlamydia trachomatis, Neisseria gonorrhoeae) or uropathogen such as E coli in man with recent urinary tract instrumentation Urethral discharge in the Urethritis absence of suprapubic pain, urinary frequency, urgency, fever Most common as sexually-transmitted infection (C trachomatis, N gonorrhoeae) Uropathogens and Antimicrobial Therapy The treatment of UTI usually includes an antimicrobial prescription. Selection of an appropriate agent depends on the anticipated pathogen, which is determined in large part by patient characteristics such as age, sex, pregnancy, the anatomic location of the infection, and comorbid conditions. Antimicrobial characteristics include spectrum of activity, pharmacokinetics (including tissue penetration into the urinary tract), and the adverse effect profile. [3] Table 5 highlights medications for acute uncomplicated cystitis, including dose, and adverse effects. Concern about infection with resistant pathogens can influence the clinician to choose an antimicrobial with broad coverage when one with a narrow spectrum of activity would be more appropriate. The use of any antimicrobial can change the microbiology in the immediate and extended environment.[2,5,25] Table 5. Oral Treatment Regimens for Acute Uncomplicated Cystitis Agent Normal Dosage Adverse Effects and Cautions Ciprofloxacin 250 mg twice a Drowsiness; increases theophylline levels; avoid in day for 3 days pregnancy; avoid divalent and trivalent cations Fosfomycin 3-g single dose Increased incidence of diarrhea and nausea and increased relapse rate Gatifloxacin 200 mg/day for Avoid in pregnancy; avoid divalent and trivalent cations 3 days Levofloxacin 250 mg/day for Avoid in pregnancy; avoid divalent and trivalent cations 3 days Nitrofurantoin 100 mg twice a Idiosyncratic pulmonary fibrosis; avoid in patients with day for 7 days estimated monohydrate/creatinine clearance < 60 mL/minute; macrocrystals; FDA pregnancy risk category B; Avoid use >/= 36 weeks gestation Norfloxacin 400 mg twice a Avoid in pregnancy; avoid divalent and trivalent cations day for 3 days Ofloxacin 200 mg twice a Avoid in pregnancy; avoid divalent and trivalent cations day for 3 days Trimethoprim 100 mg twice a Nausea; risk of treatment failure day for 3 days Trimethoprimsulfamethoxazole 1 doublestrength tablet twice a day for 3 days Nausea; rash; risk of treatment failure Most episodes of community-acquired cystitis in women, the most commonly encountered UTI, are caused by enteric Gram-negative rods from the Enterobacteriaceae group, such as E coli and P mirabilis, as well as the less commonly encountered K pneumoniae. S saprophyticus, a Grampositive organism, and E coli accounted for more than 90% of the uropathogens in one study of 4324 urine isolates obtained from women with cystitis during a 5-year period; nearly all of these isolates were sensitive to ciprofloxacin and nitrofurantoin, while up to 18% were resistant to TMPSMX and at least 28% were resistant to beta-lactams (cephalothin and ampicillin).[26] Given that E coli is by far the most common uropathogen, recent developments in TMP-SMXresistant strains bear mention. Factors influencing the development of multidrug-resistant E coli strains include liberal use of TMP-SMX to treat UTI in adults as well as to provide prophylaxis against Pneumocystis carinii pneumonia in patients with HIV. In children, attendance at day care, age younger than 3 years, and repeated TMP-SMX use for respiratory infections are risk factors for infection with a resistant uropathogen; child-to-child and child-to-parent transmission of this organism may then take place.[27,28] TMP-SMX has also been widely used in animal feed, likely contributing to TMP-SMX resistance among E coli strains in animals, although the role of the animal reservoir as a contributor to the origin or spread of uropathogenic E coli has not been demonstrated. Travel to an area with a high prevalence of TMP-SMX resistance may result in what Stamm [28] called "traveler's urinary tract infection" with a multidrug-resistant E coli strain. Multidrug resistance may be transferred on a single plasmid, often yielding resistance to TMP-SMX, ampicillin, cephalothin, and tetracycline; seldom does this multidrug resistance extend to nitrofurantoin. Infectious Disease Society of America (IDSA) Guidelines for Treatment of Uncomplicated UTI advise a 3-day course of TMP-SMX for acute cystitis treatment in regions where E coli TMP-SMX resistance is less than 20%.[27] Alternative therapies in the presence of sulfa allergy or where E coli TMP-SMX resistance rates exceed 20% include a fluoroquinolone or nitrofurantoin. Fluoroquinolones are contraindicated in children aged 18 years and under due to possible disruption of developing cartilage. The Medscape UTI Zone Resource Center[29] provides information on uropathogen susceptibility data for various regions of the United States. Choosing one of these agents will assure infection resolution; nitrofurantoin has a focused spectrum of activity and can spare gut flora exposure to a wider-spectrum antimicrobial and possibly reduce the risk for development of resistant pathogens.[25,28] When prescribing nitrofurantoin for the treatment of cystitis, the IDSA recommends a 7-day course.[27] Although E coli remains the most common uropathogen in the community and long-term-caredwelling elder, P mirabilis and K pneumoniae account for approximately one third of all infections in this age group. Length of antimicrobial in the elder with uncomplicated UTI should be 7-10 days in women and 10-14 days in men; short-course therapy is not recommended. First-line therapy includes TMP-SMX or fluoroquinolones; nitrofurantoin should not be used in the elderly, as its safe use requires a minimum creatinine clearance of 40 mL/min.[30] In the elder with impaired renal function, TMP-SMX and fluoroquinolone doses need adjustment as well. Is an Office Visit Needed? In the adult woman, the clinical presentation of cystitis nearly always includes dysuria, frequency, and/or urgency; laboratory diagnostics typically add little to the assessment process. As a result, the rationale for insisting on an office visit prior to treatment needs to be questioned. The Institute for Clinical Systems Improvement advises that in the adult woman with dysuria, frequency, and/or urgency without symptoms or risks of genitourinary disease such as sexually transmitted diseases and complicating factors, short-course antimicrobial therapy with patient education may be given without an office or provider visit.[31] Complicating factors include protracted duration of symptoms; signs and symptoms of pyelonephritis; concomitant health problems including diabetes mellitus, renal disease, or recurrent UTI; or the presence of any factor that dictates the need for an office visit and provider assessment. The University of Michigan Health Systems offers similar guidelines,[32] as does a well-designed study presented at the 2001 Interscience Conference on Antimicrobial Agents and Chemotherapy.[33] Posttreatment Follow-up Routine posttreatment cultures in uncomplicated cystitis and pyelonephritis are not warranted; follow-up cultures in complicated infection should be obtained as appropriate during the evaluation and treatment of the complicating factors. Urologic imaging (renal ultrasound or computed tomographic scan) should be considered if pyelonephritis symptoms initially resolve but recur within 2 weeks of the end of antimicrobial therapy and urine culture yields the original pathogen with sensitivity profile. Retreatment with a 2-week regimen using another agent should be considered.[4] Recurrent Infection: Relapse Vs Reinfection Approximately 20% of patients with UTI will develop a second infection with 6 months. A recurrent infection that occurs within 2 weeks of completing antimicrobial treatment and is caused by the original uropathogen is a relapse of infection. Reinfection occurs after 2 weeks of antimicrobial therapy has been completed and may be caused by the same or a different organism. [10] For women with repeated UTIs, patient-initiated therapy should be considered. In this, the patient has an appropriate antimicrobial available and initiates therapy at first UTI symptom. Recent study on this practice failed to demonstrate an increase in the rate of resistant pathogens. [33] For patient-initiated therapy to be safe and successful, the patient needs to have a clear understanding of length of UTI therapy, signs and symptoms of treatment failure, and when to seek provider assistance.[34] UTI prophylaxis may be indicated for women who experience 2 or more symptomatic UTIs within 6 months or 3 or more UTIs over 12 months, or for those with fewer infections but with severe discomfort. Both continuous prophylaxis, in which an antimicrobial is taken daily for 6 months or more, and postcoital prophylaxis, in which an antimicrobial is taken with each act of coitus, have been demonstrated to be effective in the management of recurrent uncomplicated cystitis. Prior to initiating UTI prophylaxis, resolution of the previous UTI should be confirmed by a negative urine culture 1-2 weeks posttreatment. The method prescribed is dependent upon the frequency and pattern of recurrences and patient preference.[35] Choice of an antimicrobial agent for recurrent UTI should be based on susceptibility patterns of the strains causing the patient's previous UTIs and patient history of drug allergies or intolerance. Long-term TMP-SMX or nitrofurantoin therapy has been used successfully for many years. When compared with TMP-SMX, nitrofurantoin has the advantage of lower rates of resistance of the more common UTI pathogens. The use of a fluoroquinolone for UTI prophylaxis has gained some popularity; concern about emerging resistance is an issue. UTI prophylaxis in the postmenopausal woman should also include the use of a topical estrogen to encourage lactobacilli recolonization.[14] Cranberry juice intake has been touted as a helpful measure to reduce the rate of recurrent infections. Initially believed to cause high levels of benzoic acid that resulted in urinary acidification and bacteriostatic action, further study failed to support this hypothesis. Rather, cranberry-derived substances including glycoproteins, fructose, and condensed tannins (proanthocyanidins) prevent bacterial adherence, especially E coli, to urinary epithelial cells. Infection risk is then minimized as pathogens are flushed from the urinary tract. This property has also been noted with blueberry juice. A minimum of 300-400 mg twice daily in tablet form or 8-16 oz of a >/= 30% cranberry juice blend is needed to yield therapeutic effective. Cranberry juice intake also appears to weaken attachment of E coli to inert surfaces and controls biofilm formation on urinary catheters.[36-38] However, a systematic review of studies indicated a high withdrawal rate and conflicting results. Long-term adherence to cranberry products and expected benefit may be overestimated.[39] Recommendations for Practice The assessment and treatment of the patient with a UTI is often straightforward, but in certain populations, such as pregnant women and the elderly, diagnosis and therapy can pose complex challenges for the primary care provider. Uncomplicated cystitis needs to be differentiated from pyelonephritis, urethritis, mucopurulent cervicitis, and pelvic inflammatory disease by evaluating clinical findings elicited from the physical examination and appropriate diagnostic tests. While presentation of uncomplicated cystitis in the adult woman does not always require laboratory evaluation for confirmation of diagnosis, the urine dipstick, microscopic urinalysis, and urine culture tests may play a role in other cases. Keeping in mind the most likely uropathogens and patient factors such as age, gender, comorbidity, resistant pathogen risk, previous response to therapy, urinary catheter use, and pregnancy can help guide the clinician to the most costeffective therapy. References 1. O'Donnell J, Gelone S, Abrutyne E. Selecting drug regimens for urinary tract infection: current recommendations. Infect Med. 2002;19:14-22. Available at: http://www.medscape.com/viewarticle/423482. Accessed March 11, 2002. 2. O'Brien T. Resistance problems of urinary tract infections with gram-negative bacilli. In: Cuhna B, ed. Urinary tract infections: current issues in diagnosis and treatment. Antibiotics for Clinicians. 1998;2(suppl 2):23-28. 3. Desai S. Dysuria (women). In: Desai S. Clinician's Guide to Diagnosis. Hudson, Ohio: Lexi-Comp, Inc; 2001:189-206. 4. Hooton T, Stamm W. Acute pyelonephritis: symptoms, diagnosis and treatment. Available at: www.uptodate.com. Accessed February 19, 2002. 5. Cunha B. Introduction: Urinary tract infections. In: Cunha B, ed. Urinary tract infections: Current issues in diagnosis and treatment. Antibiotics for Clinicians. 1998;2(suppl 2):3-4. 6. Kurowski K. The woman with dysuria. American Family Physician; May 1, 1998. Available at: http://www.aafp.org/afp/980501ap/kurowski.html. Accessed April 10, 2002. 7. Kunin CL. Urinary tract infections and pyelonephritis. In: Goldman L, Bennett JC, eds. Cecil Textbook of Medicine. 21st ed. Philadelphia: W.B. Saunders; 1999;613- 616. 8. Sparling PF. Introduction to sexually transmitted disease and common syndromes. In: Goldman L, Bennett JC, eds. Cecil Textbook of Medicine. 21st ed. Philadelphia: W.B. Saunders; 1999;1738-1742. 9. Centers for Disease Control and Prevention. Sexually transmitted disease treatment guidelines 2002. MMWR Morb Mortal Wkly Rep. 2002;51(No. RR-6):36-52. 10. Orenstein R, Wong ES. Urinary tract infections in adults. American Family Physician; March 1, 1999. Available at: www.aafp.org/afp/990301ap/1225.html Accessed April 10, 2002. 11. Barry HC, Ebell MH, Hickner J. Evaluation of suspected urinary tract infection in ambulatory women: A cost-utility analysis of office-based strategies. J Fam Pract. 1997;44:49-60. Abstract 12. Rejavel S, Treanor J. Adenovirus diseases. In: Goldman L, Bennett JC. Cecil Textbook of Medicine. 21st edition. Philadelphia, Pa: WB Saunders; 1999:1801-1803. 13. Desai S, Isa-Pratt S. Urinalysis. In: Desai S, Isa-Pratt S. Clinician's Guide to Laboratory Medicine. Hudson, Ohio: Lexi-Comp, Inc; 2000:517-531. 14. Stamm T, Hooton W. Recurrent urinary tract infection. Available at: www.uptodate.com. Accessed March 19, 2002. 15. Bruce G, Galloway N. Diagnostic and therapeutic considerations in catheter associated bacteruria in hospital/ chronic care facility. In: Cuhna B, ed. Urinary tract infections: current issues in diagnosis and treatment. Antibiotics for Clinicians. 1998;2(suppl 2):1116. 16. Gupta K, Stamm WE. Pathogenesis and management of recurrent urinary tract infections in women. World J Urol. 1999;17:415. 17. Warren J, Clinical presentation of urinary tract infections in the office setting. In: Cuhna B, ed. Urinary tract infections: current issues in diagnosis and treatment. Antibiotics for Clinicians. 1998;2(suppl 2):1 5-10. 18. Kunin C. Urinary tract infections and pyelonephritis. In: Goldman L, Bennett JC, eds. Cecil Textbook of Medicine. 21st ed. Philadelphia: W.B. Saunders; 1999;613-617. 19. Reid G, Bruce AW. Could probiotics be an option for treating and preventing urogenital infections? Medscape Women's Health. 2001;6(5). Available at: http://www.medscape.com/viewarticle/408951. Accessed April 10, 2002. 20. Urinary tract infections. In: Beuben D, Herr K, Pacala J, Potter J, Semla T, Small G, eds. Geriatrics at Your Fingertips. New York: American Geriatrics Society; 2000:70-73. 21. Gilbert D, Moellering R, Sande M. Sanford Guide to Antimicrobial Therapy. 32nd ed. Hyde Park, Vermont: Antimicrobial Therapy, Inc; 2002. 22. Cunha B. Therapeutic approach to treating urinary tract infections. In: Cuhna B, ed. Urinary tract infections: current issues in diagnosis and treatment. Antibiotics for Clinicians. 1998;2(suppl 2):35-40. 23. Hale T. Medications and Mothers' Milk. 10th ed. Amarillio, Texas: Pharmasoft Medical Publishing; 2002. 24. Howe DS. Urinary tract infection, male. Available at: http://www.emedicine.com/emerg/topic625.htm (free registration required). Accessed June 4, 2002. 25. Desai S. Dysuria (men). In: Desai S. Clinician's guide to diagnosis. Hudson, Ohio: LexiComp, Inc; 2001:78-81. 26. Gupta K, Scholes D, Stamm W. Increasing prevalence of antimicrobial resistance among uropathogens causing acute uncomplicated cystitis in women. JAMA. 1999;281:736-738. Abstract 27. Warren J, Abrutyne E, Hebel R, Johnson J, Schaeffer A, Stamm W. Guidelines for antimicrobial treatment of uncomplicated acute bacterial cystitis and pyelonephritis in women. Clin Infect Dis. 1999;29:745-758. Abstract 28. Stamm W. An epidemic of urinary tract infections? N Engl J Med. 2001;345:1055. 29. Medscape Resource Center -- UTI-Zone. Available at: http://www.medscape.com/pages/editorial/resourcecenters/public/uti/rc-uti.ov. Accessed June 5, 2002. 30. Shua-Haim JR, Ross JS. Urinary-tract infections in the elderly: a practical approach. Clin Geriatr. 2000. Available at: http://www.mmhc.com/engine.pl?station=mmhc&template=cgfull.html&id=1076. Accessed April 10, 2002. 31. Health Care Guideline: Uncomplicated urinary tract infection in women. Institute for Clinical Systems Improvement. May 2001. Available at: http://www.icsi.org/knowledge/detail.asp?catID=29&itemID=200. Accessed March 29, 2002. 32. Gradwohl C, Foude K, Harrison V, Munger K, Zoschnick L. University of Michigan Health System Guidelines for Clinical Care: Urinary tract infection. Available at: http://cme.med.umich.edu/pdf/guideline/UTI.pdf. Accessed March 29, 2002. 33. Gupta T, Hooton TM, Roberts PL, Stamm WE. Antimicrobial resistance in uropathogens from patients utilizing self-initiated therapy for recurrent UTI. Program and abstracts of the 41st Interscience Conference on Antimicrobial Agents and Chemotherapy; December 16-19, 2001; Chicago, Illinois. Abstract 1352. 34. Barry HC, Hickner J, Ebell MH, Ettenhofer T. A randomized controlled trial of telephone management of suspected urinary tract infections in women. J Fam Pract. 2001;50:589594. Abstract 35. Stamm W, Hooton T. Overview of acute cystitis. Available at: www.uptodate.com. Accessed March 10, 2002. 36. Avorn J, Monane M, Gurwitz JH, Glynn RJ, Choodnovskiy I, Lipsitz LA. Reduction of bacteriuria and pyuria after ingestion of cranberry juice. JAMA. 1994;271:751-754. Abstract 37. Zafriri D, Ofek I, Adar R, Pocino M, Sharon N. Inhibitory activity of cranberry juice on adherence of type 1 and type P fimbriated Escherichia coli to eucaryotic cells. Antimicrob Agents Chemother. 1989;33:92-98. Abstract 38. Ofek I, Goldhar J, Zafriri D, Lis H, Adar R, Sharon N. Anti-Escherichia coli adhesin activity of cranberry and blueberry juices. N Engl J Med. 1991;324:1599-1599. 39. Jepson RG, Mihaljevic L, Craig J. Cranberries for preventing urinary tract infections. In: The Cochrane Library, Issue 3, 2000. Office Management of UTI: Practical Cases Author: Desiree Lie, MD, MSED Case #1: Diagnosis and Testing for Possible UTI Presenting Scenario A 23-year-old healthy female college student, gravida 0, para 0, presents to your office with a 2day history of "on and off" dysuria, urgency, and frequency and a single episode of gross hematuria. There is no fever or back pain. She has self-medicated with cranberry juice and pyridium 200 mg, which was left over from a previous urinary tract infection (UTI). Her urine is consequently dark-colored. She has had 2 prior UTIs in the past year, which were successfully treated each time with trimethoprim-sulfamethoxazole (TMP-SMX) 160 mg/800 mg twice a day for 3 days. The last UTI was 4 months ago and there is no history of pyelonephritis. She is heterosexual, has been sexually active since 18 years of age, currently uses an oral contraceptive, and has not missed any pills. She is currently in a monogamous sexual relationship that has lasted 6 months. She believes that her partner is also monogamous. She has had a total of 4 lifetime sexual partners and does not admit to any history of sexually transmitted disease (STD). Her last menstrual period was 3 weeks ago, at the expected time. Physical examination shows that she is afebrile with no suprapubic tenderness or costovertebral angle tenderness. What Is the Differential Diagnosis? This patient has a primary symptom of dysuria. Given her history of recurrent UTIs and her response to TMP-SMX, it is likely that she was infected with Escherichia coli in the past. E coli is the most prevalent pathogen in this scenario, and she is at risk of reinfection due to previous antibiotic therapy and sexual activity.[1,2] Therefore, the first possibility for diagnosis would be uncomplicated lower tract UTI, which is characterized by a symptomatic patient with bacterial colony count of more than 102 colonies/mL. Given this patient's young age and sexual history, urethritis and cervicitis due to sexually transmitted infection should be ruled out. A finding of mucopurulent vaginal discharge would raise suspicion for this. Additional history findings to support this diagnosis would be longer length of symptoms (> 7 days) and lack of hematuria. In situations when a sexually transmitted infection is suspected, a pelvic exam would be the next step. Urethral and cervical chlamydia testing using the ligase chain reaction test (90% sensitivity and 98% specificity) or amplified DNA test (higher sensitivity) as well as gonococcal testing using these methods or culture can be performed. In cases where pelvic exam is not practical, chlamydia and gonorrhea testing may be done on spot urine samples via DNA amplification methods. It is also prudent to rule out pregnancy if contraception is unreliable. What Are the Appropriate Next Steps to Take? With a straightforward clinical presentation, immediate treatment with the appropriate antibiotic may be justified. However, in a patient with recurrent UTIs, diagnostic testing is warranted. Culture and sensitivity are particularly important with recurrent UTIs to exclude infection with a new organism (such as Proteus mirabilis or Klebsiella pneumoniae) or the emergence of E coli resistance to TMP-SMX. For this patient, urine sampling with dipstick, microscopic urinalysis, and culture and sensitivity should be considered as the next step. For the diagnosis of UTI, the dipstick has a sensitivity of 95%, a specificity of 75%, a positive predictive value of 30% to 40%, and a negative predictive value of 99%.[3] A negative dipstick is therefore usually sufficient to exclude true infection, and a positive test should be followed by bacterial culture and sensitivity. Urinalysis was positive for pyuria at 3 leukocytes/hpf, and negative for bacteria. Urine culture was sent. The clinician opted not to do pelvic exam on this patient, but educated her to report mucopurulent discharge or other symptoms of sexually transmitted diseases and encouraged her to follow up for yearly Pap smear and STD screening. What Are the Appropriate Steps for Immediate Office Management and Follow-up? The information obtained so far suggests a lower tract UTI. Since urine culture results are pending, and findings point to an uncomplicated lower UTI, immediate management should include an antimicrobial with activity against E coli and Staphylococcus saprophyticus, the 2 most common UTI pathogens in women during the reproductive years. Choices include TMP-SMX, used by the patient in the past, inexpensive but with the risk of possible E coli resistance; nitrofurantoin, relatively inexpensive with little E coli or S saprophyticus resistance (and with the added benefit of sparing normal vaginal flora and little risk of subsequent Candida vaginitis), or a fluoroquinolone, most expensive but with activity against most strains of E coli, Proteus mirabilis, and S saprophyticus, but with growing concerns about excessive use and subsequent resistance. The following are the dosing options for this patient: TMP-SMX: 160 mg TMX/800 mg SMX twice daily, for 3 days. (Consider resistance potential.) Nitrofurantoin 50-100 mg 4 times each day for 7 days, or nitrofurantoin as macrocrystals and monohydrate 100 mg twice a day for 7 days. Levofloxacin 250 mg once a day for 3 days. Ciprofloxacin 250 mg twice a day for 3 days. Although voiding at regular intervals with efficient bladder emptying, wiping patterns, and postcoital voiding have not been proven to provide UTI protection, including these recommendations for young women with recurrent UTIs associated with sexual activity may at least raise awareness that intercourse is related to UTIs. The clinician may also recommend steps to prevent fecal contamination of the vaginal and urethral area (eg, avoid rear-entry coital positions), adequate vaginal lubrication, avoidance of the intravaginal insertion of foreign objects including diaphragms, and early detection and treatment. Prophylaxis (such as antibiotics after intercourse) may be considered after all of these measures have failed to prevent recurrent UTIs. Case #2: Asymptomatic Bacteriuria in Pregnancy Presenting Scenario During her fourth routine prenatal visit at 20 weeks' gestation as determined by reliable dates and early ultrasound, a 32-year-old healthy gravida 1, para 0 woman is found to have asymptomatic bacteriuria, with > 105 CFU/mL in a clean-catch MSU specimen. The pregnancy is otherwise uncomplicated and she does not have any complaints. Further Findings in This Patient Urine culture was positive for 105 CFU/mL of E coli. The patient was given cefixime 250 mg by mouth once/day for 3 days, and completed therapy. Nitrofurantoin 100 mg twice a day for 7 days is also an alternative. A test of cure was obtained 1 week after completion of therapy and repeated monthly until completion of pregnancy. Repeat urinalysis showed no bacteria, the patient remained asymptomatic and the pregnancy was otherwise uncomplicated. If repeat culture suggests persistent asymptomatic bacteriuria, the patient should be treated with suppressive therapy such as nitrofurantoin 50 or 100 mg at bedtime or cephalexin 250 or 500 mg at bedtime, until delivery. Case #3: UTI in the Elderly Postmenopausal Female Presenting Scenario You receive a call from a convalescent home that a 68-year-old normally healthy and ambulatory female patient has recently become lethargic, less active, and anorexic over the past week. She is afebrile and has no organ-system specific symptoms. She complains only of nonspecific lower abdominal pain unrelated to food or bowel movements. Her mental status has not changed and is reportedly normal. She has not been sexually active since losing her husband 10 years ago. Her blood pressure is noted to be lower than usual, at 110/50 mm Hg; her usual blood pressure is 130/70 mm Hg. She had a UTI 2 months ago, which was confirmed by urine culture. She was responsive to ciprofloxacin 250 mg twice a day for 7 days after failing initial therapy with TMPSMX 160 mg/800 mg twice a day for 7 days. She is allergic to penicillin. She is on no regular medications other than vitamins, and takes acetaminophen as needed for mild arthritis. Her most recent annual physical examination was performed 3 months ago and was normal. Pelvic examination and Pap smear revealed atrophic vaginitis only, but was otherwise normal. Cholesterol, thyroid-stimulating hormone, and hemoglobin were all normal. A clean-catch MSU specimen was sent yesterday for urinalysis and was positive for nitrates, leukocyte esterase, and bacteria. A specimen has been sent for culture and sensitivity. What Factors Should Be Considered in the Evaluation of This Patient? UTIs are a leading cause of Gram-negative bacteremia, which is associated with significant morbidity and mortality in the elderly. They account for approximately 1 million hospitalizations annually in the United States and are one of the most frequently presenting diagnoses to emergency rooms and ambulatory settings.[4] The incidence of bacteriuria increases from less than 5% in adult women to over 20% in females older than aged 65 years. In the elderly, UTI symptoms can be atypical, and include confusion, lethargy, cough, weakness, dyspnea, abdominal pain, change in mental status, and anorexia. Patients at increased risk of UTI include those who are frail, immobile, recently hospitalized, incontinent, catheterized, recently receiving genitourinary manipulation, estrogen-deficient females, and those with a history of UTI or bacteriuria. Organisms causing uncomplicated and complicated UTI in order of decreasing frequency include E coli, S saprophyticus, Klebsiella pneumoniae, P mirabilis, Enterococcus faecalis, and Pseudomonas aeruginosa. Complicated UTIs include those infections caused by multiple drug-resistant organisms. This patient's history puts her at risk for a complicated UTI, and she should be examined to exclude pyelonephritis and bacteremia. Further Findings in This Patient Physical examination of the patient confirms the initial telephone assessment and, in addition, shows clinical dehydration, nonspecific lower abdominal tenderness, some confusion (not oriented in time and place), fecal impaction, and signs of estrogen deficiency in the introitus and vagina. What Is the Next Appropriate Step in Management? Although she is afebrile, this patient could still have pyelonephritis and bacteremia. Given her past history of TMP-SMX resistance, she has a complicated UTI. Blood culture, complete blood count with differential, IV hydration, and even hospital evaluation and admission are justified. What Antibiotic Treatment Options Are Recommended? Her urine culture is positive for P mirabilis, white blood count is normal, and blood cultures are negative. Duration of therapy should be at least 7 to 10 days.[5] Antibiotic options, given her past TMP-SMX resistance, include: Ciprofloxacin 250 mg twice daily Levofloxacin 250 mg once daily Nitrofurantoin 100 mg twice daily Norfloxacin 400 mg twice daily Ofloxacin 200 mg twice daily Dosing frequency and side effect profile are additional considerations in selection. See Table 5 in the main paper for an analysis of these variables. What Strategies Should Be Considered to Prevent Future UTIs in This Patient? Given her risk factors for recurrent UTI, the following measures may be helpful: Local estrogen in the form of topical estrogen cream. Recent evidence suggests that an estrogen-releasing vaginal ring can effectively reduce recurrence of UTI in elderly postmenopausal women.[6] Adequate oral hydration and voiding pattern. Prevention and treatment of constipation. Possible monthly urine sampling for bacteriuria. Exclusion of comorbid medical conditions such as diabetes and occult colon cancer, as warranted by history and examination. Practice Points In the presence of pyuria with dysuria and other UTI symptoms, a bacterial culture standard of 102 CFU/mL, rather than the traditional 105 CFU/mL, is adequate for confirmation of UTI diagnosis. An adult woman with classic presentation of lower UTI of short duration without significant recurrence, risk factors for sexually transmitted infections, or signs of obstruction may be treated with a short course of antibiotic (usually 3 days) without confirmation by diagnostic testing. Prescribing for UTI should be guided by local resistance patterns. TMP-SMX is not the first drug of choice in areas where resistance prevalence is greater than 20%. Asymptomatic bacteriuria should be aggressively sought and treated in pregnancy to prevent adverse maternal and fetal outcomes. The elderly, frail patient is at greater risk of morbidity and mortality from UTI vs the healthy young patient, and is more likely to present with atypical symptoms. Patient education and preventive care is an essential part of UTI management. References 1. Warren JW. Clinical presentation of urinary tract infections in the office setting. Antibiotics Clinicians. 1998;2(supplement 2):5-10. 2. Ikaheimo R, Siitonen A, Heiskanen T, et al, Recurrence of urinary tract infection in a primary care setting: analysis of a one-year follow-up study of 179 women. Clin Infect Dis. 1996;22:91. 3. Pappas PG. Laboratory in the diagnosis and management of urinary tract infection. Med Clin North Am. 1991;75:313. 4. Oreinstein R, Wong ES. Urinary tract infections in adults. Am Fam Physician. 1999;59:1225-1234. Abstract 5. O'Donnell JA, Gelone SP, Abrutyn E. Selecting drug regimens for urinary tract infections: current recommendations. Available at: http://www.medscape.com/viewarticle/423482. Accessed June 5, 2002. 6. Eriksen B. A randomized, open, parallel-group study on the preventive effect of an estradiol-releasing vaginal ring (Estring) on recurrent urinary tract infections in postmenopausal women. Am J Obstet Gynecol. 1999;180:1072-1079. Abstract