Supplementary Information (doc 638K)
advertisement
")
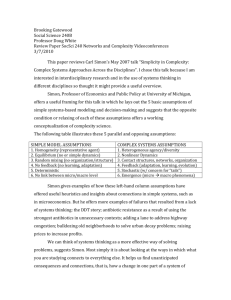
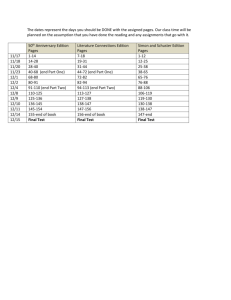
Supplementary Information: Treatment Plan Mobilization of hematopoietic stem cells was performed in 32 patients after the first or the second course of HyperCHidam and in 2 cases after low-dose cytarabine [0.8 gr/m2 every 12 hours for three days]. Mobilized stem cells were not used in case of a suitable donor (n=12), PD (n=6), NRM (n=1), physician decision (n=1). In alloSCT, G-CSF (300 μg/day sc) was administered starting on day + 7 until PMN > 1000/μl for 2 consecutive days. In autoSCT, G-CSF (300 μg/day sc) was administered starting on day + 3 until PMN > 1000/μl for 2 consecutive days. Prophylaxis against herpes simplex, varicella zoster virus and against Pneumocystis Carini was administered (800 mg acyclovir twice a day; 800/160 mg sulphametoxazole/trimethoprim once a day on alternate days). CMV reactivation was monitored with antigen pp65 or with virus DNA detection technique according to the methods used by each concerned Department. In case of laboratory signs of reactivation, pre-emptive treatment was started (oral valgancyclovir or intravenous gancyclovir). Study design and Statistical Methods Clin A sample size calculation: according to the Simon optimal two-stage study design (Simon R. Optimal two-stage designs for phase II clinical trials. Controlled Clinical Trials 1989; 10: 1-10), the study has a type I error rate of 5% if the complete clinical response probability is 20%, and 95% power for concluding that the experimental treatment is promising if the response probability is 40%. Twenty-eight patients were to be accrued in the first stage, with 7 or more responses required to continue on to the second stage of 34 additional patients. In the final analysis, at least 18 responses out of the total 62 patients were to be considered evidence of promising activity. Clin B sample size calculation: according to the Simon optimal two-stage study design (Simon R. Optimal two-stage designs for phase II clinical trials. Controlled Clinical Trials 1989; 10: 1-10), the study has a type I error rate of 5% if the complete clinical response probability is 20% (reflecting the experience with standard treatments), and 90% power for concluding that the experimental treatment is promising if the response probability is 40%. Nineteen patients were to be accrued in the first stage, with 5 or more responses required to continue on to the second stage of 35 additional patients. In the final analysis, at least 16 responses of the total 54 patients were to be considered evidence of promising activity. The CR probability was estimated as proportion of CR over the total number of intention-to-treat patients; the corresponding 95% confidence limits were calculated using the exact method, i.e. taking into account the binomial distribution of proportions. 1 DFS time was calculated as the interval from CR achievement to first disease relapse or death, regardless of the cause, with censoring at the date of last follow-up assessment. PFS time was calculated as the interval from beginning of treatment to disease progression or death, regardless of the cause, with censoring at the date of last follow-up assessment. OS time was calculated as the interval from beginning of treatment to death for all causes, with censoring at the date of last follow-up assessment. In the univariable Kaplan-Meier analyses of PFS and OS involving transplant (auto, allo), time was calculated from the transplant date. In the multivariable Cox model patient’s age was modelled as continuous variable by means of a nonlinear transformation, ie 3-knots restricted cubic splines (RCSs), (Durrleman S, Simon R. Flexible regression models with cubic splines. Stat Med. 1989;8(5):551 – 561). Concordantly, the values used in the tables presenting the Cox model results were not cut-off values but exact values, ie the quartiles of the variable distribution. RCS modelling has the advantage of (i) allowing the age prognostic effect not to be the same in every part of the range; (ii) taking as reference for hazard ratio estimation every value within the range of the variable distribution. The analyses were performed using the software SAS (SAS Institute Inc., Cary, NC) and R (R Development Core Team (2006). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, URL: http://www.rproject.org/, last access Apr 2nd 2013). 2 Figure S1 A) Progression-free survival and B) Overall survival according to the hystotype (excluding patients with enteropathy-associated T-cell lymphomas). 100 PTCLNOS 100 ALK-neg 75 OS(%) PFS(%) 75 50 25 AILD 50 25 p=0.83 p=0.99 0 0 0 20 40 time (months) 60 80 0 20 40 60 80 time (months) 3 Figure S2 A) Progression-free survival by treatment modality calculated from date of transplantation; auto: autoSCT; allo: alloSCT, B) overall survival by treatment modality calculated from date of transplantation; auto: autoSCT; allo: alloSCT; patients not transplanted are not included in the analysis. 1.0 A 0.6 0.4 alloSCT 0.2 Probability 0.8 autoSCT 0.0 p=0.92 0 6 12 18 24 Time (months) B 0.2 0.4 0.6 alloSCT p=0.10 0.0 Probability 0.8 1.0 autoSCT 0 6 12 18 24 Time (months) 4