THE UNIVERSITY OF CHICAGO Department of PEDIATRICS
advertisement

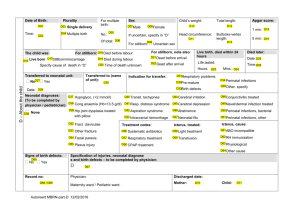
THE UNIVERSITY OF CHICAGO DEPARTMENT OF PEDIATRICS NEONATAL/PERINATAL MEDICINE 5841 S. MARYLAND AVENUE, MC 1051 CHICAGO, IL 60637 APPLICATION FOR NEONATAL/PERINATAL MEDICINE FELLOWSHIP For Training Period: July 1, 200__ to June 30, 200__ Indicate the Subspecialty Area for which you are applying: Specialty Training Choice (if applicable) Specialty Training Choice (if applicable) Specialty Training Choice (if applicable) APPLICANT INFORMATION Last Name Street Address City Home Phone Pager State First Name M.I. Country Zip Code Business Phone Email Address Date of Birth Social Security No. Cell Phone Place of Birth CITIZENSHIP Citizenship (please check one) U.S. Citizen Permanent Resident If not a citizen or permanent resident, please give visa status: EDUCATION Undergraduate Medical School Honors and Awards Degree Upon Completion Relative Class Rank Date of Graduation Date of Graduation Internship Inclusive Dates Residency Inclusive Dates USMLE Scores Part I ECFMG Certificate No. Part II (MM / YY) (MM / DD / YY) (MM / YY-MM / YY) (MM / YY-MM / YY) Part III ECFMG Issue Date: Please provide a hard copy of the USMLE Scores and your ECFMG Certificate. 1 THE UNIVERSITY OF CHICAGO DEPARTMENT OF PEDIATRICS NEONATAL/PERINATAL MEDICINE 5841 S. MARYLAND AVENUE, MC 1051 CHICAGO, IL 60637 Application - Page Two EXPERIENCE Hospital and Research Practical Experience (use additional sheet if necessary): NOTE: You may complete and submit your application electronically. However, before your application will be considered we must have the following: 1) Completed and signed hard copy of the application (please do not leave any items blank) 2) Curriculum Vitae 3) Personal Statement that delineates your career plans and gives us a brief biography 4) Hard copies of your USMLE Scores 5) A copy of your ECFMG certificate if you are a foreign medical graduate 6) Three letters of recommendation addressed to Lee Kwang-sun MD, Director, Neonatal/Perinatal Fellowship Program Please send completed application to: Signature of Applicant Maria Corpuz University of Chicago Department of Pediatrics 5841 S. Maryland Ave., MC 1051 Chicago, IL 60637-1470 Telephone: 773-702-3056 Fax: 773-702-0764 Email: mcorpuz@peds.bsd.uchicago.edu Date 2