Viral Informationb doc
advertisement

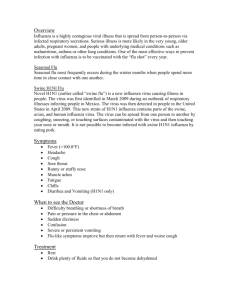
Influenza Virus from Fields Virology Miscellany Relevant for Modeling Influenza Infection from Fields Virology (Knipe and Howley 2001), a Great Book (Kevin Morgan, Nov5th_2004) I have bolded a few key issues to save you reading the whole thing (there is a lot more!). See Fields Virology for details of virus structure (left) and ‘life’-cycle (right). Sorry these are a bit fuzzy! Translational Control Mechanisms Two major translational controls operate in influenza A virus–infected cells: (a) suppression of the interferon (IFN)-induced block against all protein synthesis, thereby ensuring the efficient translation of virus-specific proteins in infected cells (141,163); and (b) shutoff of the translation of cellular mRNAs, resulting in the selective translation of viral mRNAs (163,176,188,316,317). Unless a virus-specific defense mechanism were established, overall translation in influenza virus–infected cells would be inhibited because of the production of virusspecific RNA molecules that contain double-stranded regions. The potential for the formation of such double-stranded RNA (dsRNA) molecules stems from the presence of both positive-sense and negative-sense RNAs that are synthesized in the nucleus during infection (163). These viral dsRNA molecules would activate the cellular kinase PKR (141). This dsRNA-activated kinase is expressed constitutively in eukaryotic cells at low levels, and its synthesis is substantially induced by IFN (141,210). Because virusspecific dsRNA also induces IFN (reviewed in 141), increased levels of PKR would be expected to be present in influenza virus–infected cells, and it has been shown that PKR is initially activated during infection (141). -1- Influenza Virus from Fields Virology ASIDE: with some difficulty (via the IPA tools, Gene Cards, and PubMed) I did manage to locate PKR in the control data set we are using for this work, see graph below which shows nice (though noisy) post-infection signal, plus inhibition by dex. Prkr Protein kinase interferon-inducible double stranded RNA dependent 140 Normalized Signal (stdevp) 120 100 80 60 40 20 Dex4_d3 Dex4_d1 Dex4_d-1 Dex2_d3 Dex2_d1 Dex2_d-1 VC_d3 VC_d1 VC_d-1 NC_d3 NC_d1 NC_d-1 0 Continued activation of PKR would lead to a global shutdown of protein synthesis because activated PKR phosphorylates the a-subunit of the initiation factor eIF-2 (141,210). This initiation factor forms the ternary complex (eIF-2) · g GTP · (mettRNAi) that binds to the initiating 40S ribosomal subunit before mRNA is bound (135). Phosphorylation of the a-subunit of eIF-2 prevents the recycling of eIF-2–g GDP to form the functional form of eIF-2, eIF-2-GTP (reviewed in 296). Recycling has been shown to be catalyzed by the factor eIF-2B, which is trapped in an inactive complex with eIF-2GDP when the a-subunit of eIF-2 is phosphorylated (reviewed in 296). Without this recycling of eIF-2 by eIF-2B, protein synthesis initiation is effectively blocked. Influenza virus mounts a two-pronged attack against the action of PKR. The virusspecific NS1 protein binds to, and hence sequesters, viral dsRNA molecules, thereby blocking the activation of PKR (102,202). In addition, a 58-kd cellular protein that inhibits PKR function is activated in influenza virus–infected cells (191,192). The experimental evidence indicates that this 58-kd cellular protein interacts directly with PKR, and that influenza virus activates the inhibitory activity of the 58-kd protein by dissociating it from its own natural inhibitor. In contrast, the mechanism by which viral mRNAs are selectively translated over cellular mRNAs in infected cells is poorly understood. One of the key elements in the shutoff of -2- Influenza Virus from Fields Virology host cell protein synthesis takes place in the nucleus of infected cells: newly synthesized cellular pre-mRNAs are degraded (143). This degradation is probably initiated by the cleavage of the 5´ ends of cellular pre-mRNAs transcripts by the viral cap-dependent endonuclease (163). The resulting decapped RNAs would be more susceptible to degradation by cellular nucleases, as it has been shown that the 5´ cap structure stabilizes RNAs against nucleolytic degradation both in vivo and in cell extracts (6). This degradation is probably significantly enhanced by the action of the viral NS1 protein, which blocks the nuclear export of cellular mRNAs (as discussed later). As a consequence, the mRNAs in the cytoplasm of influenza virus–infected cells are composed of cellular mRNAs synthesized before infection (“old cellular mRNAs”) and viral mRNAs synthesized after infection (“new viral mRNAs”). Nonetheless, high levels of these old cellular mRNAs are found in the cytoplasm of infected cells (143). These cellular mRNAs are stable and also functional, as assayed by their efficient translation in reticulocyte extracts in vitro (143). Consequently, the shutoff of host cell protein synthesis, which is complete by about 3 hours after infection in several cell lines, probably does not result from the degradation or modification of cytoplasmic old cellular mRNAs. Based on the polysome distribution of several representative cellular mRNAs in uninfected and infected cells, it has been concluded that both the initiation and the elongation step in the translation of old cellular mRNAs are blocked in infected cells (142). A molecular mechanism for a selective block against the elongation of cellular, but not viral, proteins has not been established. However, selectivity at initiation is probably due at least in part to the fact that influenza viral mRNAs are efficient initiators of translation (79,142,143). Other possible mechanisms for the selective translational initiation of viral over cellular mRNAs include the following: 1. The inhibition of the activation and activity of PKR may be partial, rather than complete (142,163). Under such conditions, the translation of viral mRNAs would be favored over the translation of cellular mRNAs because influenza viral mRNAs are better initiators of translation (142,143). 2. The NS1 protein may bind to the 5´-untranslated regions (5´-UTRs) of viral mRNAs, thereby causing, in a manner unknown, the selective translation of these mRNAs (61,74,251). However, no binding of the NS1 protein to the 5´-UTR in full-length viral mRNAs has been detected (278). Nonetheless, the NS1 protein may play a role in translation in infected cells because the NS1 protein appears to be associated with the polysomes of virus-infected cells (50,78,166). 3. Cellular proteins function in the selective translation of influenza virus mRNAs in infected cells. It has been reported that: (a) the cellular RNA-binding protein GRSF-1 specifically binds to the 5´-UTRs of viral mRNAs (252); and (b) the human homologue of the Stauffen protein, which binds to dsRNA, interacts with the NS1 protein that is associated with polysomes in infected cells (78). 4. One or more cellular protein initiation factors may be modified in influenza virus– infected cells (79), a strategy employed by some other viruses to ensure that their mRNAs are selectively translated (89). -3- Influenza Virus from Fields Virology The NS1A Protein Inhibits the Cellular Interferon Response The several hundred cellular proteins that are induced by IFN-a/b constitute one of the initial host defenses against virus infection (62,327). Reverse genetics experiments have established that the NS1A protein plays a crucial role in protecting influenza A virus against the cellular IFN response: influenza A viruses that lack the NS1A gene replicate only when the cellular IFN response is defective (84). One IFN-induced pathway involves PKR, and as discussed previously, the RNA-binding domain of the NS1A protein, by binding to dsRNA molecules, inhibits the activation of PKR in vitro (101,102,202). Evidence that the NS1A protein carries out this function in influenza virus–infected cells was obtained using mutant viruses that contain ts mutations in the NS1A protein coding sequence (102). IFN-induced pre-mRNAs are synthesized after infection and consequently should be subjected to the effector domain-mediated inhibition of nuclear export, followed by nuclear degradation (41,143,228,313). As a result, few or no IFN-induced mRNAs should survive, and few or no IFN-induced proteins should be synthesized in influenza A virus–infected cells. Consistent with such a role of the effector domain, laboratory-generated viruses that lack deletions of the effector domain fail to protect the virus against IFN (70). Only in Vero cells, which are defective in IFN production, do these mutant viruses grow as well as wild-type virus in tissue culture. The efficiency of replication of these mutant viruses in MDCK cells, which produce IFN, is inversely correlated with the length of the effector domain of the encoded NS1A protein, and these viruses are attenuated in wild-type mice that produce IFN. Fields Virology Section Two: Specific Virus Families Chapter 47: Orthomyxoviruses EVOLUTIONARY PATHWAYS OF INFLUENZA VIRUSES Studies on the ecology of influenza viruses have led to the hypothesis that all mammalian influenza viruses are derived from avian influenza reservoirs (520). Support for this theory comes from phylogenetic analyses of nucleic acid sequences of influenza A viruses from a variety of hosts, geographic regions, and virus subtypes. A surprising discovery from phylogenetic analyses of amino acid changes (Fig. 4) was that avian influenza viruses, unlike mammalian strains, show low evolutionary rates (166). In fact, influenza viruses in wild aquatic birds appear to be in evolutionary stasis, with no evidence of net evolution over the past 60 years. Nucleotide changes have continued to occur at a similar rate in avian and mammalian influenza viruses, but these changes no longer result in amino acid changes in the avian viruses, whereas all eight mammalian influenza gene segments continue to accumulate changes in amino acids. The high level of genetic conservation suggests that avian influenza viruses in their natural -4- Influenza Virus from Fields Virology reservoirs are approaching or have reached an adaptive optimum, wherein nucleotide changes provide no selective advantage. It also means that the source of genes for pandemic influenza viruses exists phenotypically unchanged in the aquatic bird reservoir. Figure 47-4 Phylogenetic trees for 41 influenza A virus NP genes rooted to influenza B virus NP (B/Lee/40). Left: Nucleotide tree. Horizontal distance is proportional to the minimal number of nucleotide differences to join nodes and NP sequences. Vertical lines, Spacing branches and labels. Animal symbols (black) denote the five host-specific lineages. Animal symbols (white) denote viruses in that lineage that have been transmitted to other hosts. Right: Amino acid tree. A table of abbreviations for virus isolates shown in these trees may be found in Gorman et al. (166). Phylogenetic analyses of the NP gene show that avian influenza viruses have evolved into five host-specific lineages (see Fig. 4): an ancient equine lineage, which has not been isolated in more than 20 years; a recent equine lineage; a lineage in gulls; one in swine; and one in humans. The human and classic swine viruses have a genetic sister-group relationship, which shows that they evolved from a common origin. It appears that the ancestor of the human and classic swine virus was an intact avian virus that, like the influenza virus currently circulating in pigs in Europe, derived all of its eight genes from avian sources (520). Studies of the NP and other genes in avian species reveal separate sublineages of influenza in Eurasia and the Americas. Studies on the 1918 influenza genome by Taubenberger's group (415) suggested that the precursor of the 1918 pandemic may have circulated in mammals before being transmitted to humans or alternatively may have been derived from a contemporary avian strain. Influenza A viruses in humans usually evolve along a single-branch lineage, leading to the hypothesis that these viruses evolve by clonal reconstitution after widespread extinction (52). However, detailed analysis shows that some human influenza sublineages can cocirculate for a limited period (86,93), which causes added difficulties in the selection of vaccine strains. In contrast, the B and C viruses exhibit multiple-lineage evolution, which indicates the presence of cocirculating strains within the human population (551). The pattern of epidemiology and evolution of the B and C viruses suggests that they are at or approaching an evolutionary equilibrium with their human -5- Influenza Virus from Fields Virology hosts, whereas the A viruses of humans are not and are prevented from it by perturbations arising from reassortment of human virus genomes with those from avian viruses. Overall, the most important implication of phylogenetic studies is that the ancestral viruses that caused Spanish influenza in 1918, as well as the viruses that provided gene segments for the Asian/1957 and Hong Kong/1968 pandemics, are still circulating in wild birds, with few or no mutational changes. Fields Virology Section Two: Specific Virus Families Chapter 47: Orthomyxoviruses PATHOGENESIS IN HUMANS Pattern of Virus Shedding Influenza virus replicates throughout the respiratory tract, with virus being recoverable from the upper and lower tracts of people naturally or experimentally infected with virus. ASIDE: We need to think carefully about the dosimetry when building our model. I recommend that you see Bahman’s particle deposition model sooner rather than later! The pattern of virus replication in six adult volunteers administered an influenza A/HK/68-like H3N2 virus, in relation to the onset of clinical symptoms, IFN response, and serum and nasal wash antibody responses, is presented in Fig. 10 (420). Virus replication peaks at about 48 hours after inoculation and declines somewhat slowly thereafter, with little shedding after days 6 to 8. Peak virus titers in symptomatic volunteers range from 103.0 to 107.0 TCID50/mL of nasopharyngeal wash (349), with a positive correlation between the amount of virus shedding and the severity of the clinical response. Individuals who shed less than 103.0 TCID50/mL are either asymptomatic or have only minor upper respiratory tract symptoms. Even after infectious virus can no longer be recovered, viral antigen can be detected for several days in cells and secretions of infected individuals (33,113,487). In children naturally infected with influenza viruses, virus is most frequently recovered 1 to 2 days after the onset of symptoms and can be found for up to 13 days thereafter (143). The peak titer is achieved on the first day of illness and averages 104.0 TCID50/mL of nasal wash (188). -6- Influenza Virus from Fields Virology Figure 47-10 Six seronegative volunteers received 104.0 TCID50 of wild-type A/Bethesda/1015/68 virus intranasally on day 0. From ref. 149, with permission. Pathology Influenza A virus induces pathologic changes throughout the respiratory tract, but the most significant pathology is present in the lower respiratory tract (207–210,513). During bronchoscopy of persons with uncomplicated influenza infections, acute diffuse inflammation of the larynx, trachea, and bronchi were observed with mucosal inflammation and edema. Light-microscopic studies of infected cells revealed that the columnar ciliated cells become vacuolated, edematous, and lose cilia before being desquamated. Within 1 day after the onset of symptoms, desquamation of the ciliated and mucus-producing epithelial cells down to a one-cell-thick basal layer is observed; in other areas, the thickened and hyalinized basement membrane is exposed. Submucosal edema and hyperemia occur with an infiltration by neutrophils and mononuclear cells (310). Viral antigen is present predominantly in epithelial cells and mononuclear cells, but is infrequently found in the basal cell layer (344). In a more severe primary viral pneumonia, there is an interstitial pneumonitis with marked hyperemia and broadening of the alveolar walls, with a predominantly mononuclear leukocyte infiltration and capillary dilation and thrombosis. The alveolar walls become denuded of epithelium; intraalveolar edema and exudate are present; hyaline membranes cover alveolar walls; and intraalveolar hemorrhage occurs. Influenza virus–specific antigen is present in type 1 and 2 alveolar epithelial cells, as well as in intraalveolar macrophages (344). Necrotizing changes may occur with rupture of walls of alveoli and bronchioles. Influenza virus has been obtained from lungs at autopsy in titers of 102.0 to 105.7 50% egg infectious doses per gram of tissue (300). At a cellular level, influenza virus shuts off cell protein synthesis and induces apoptosis as an additional means of cell destruction (216). ASIDE: The latter sentence implies that the virus ‘intends’ to kill cells. Does this make sense in a predator-prey situation? From the third to fifth day after onset of illness, mitoses appear in the basal cell layer, and regeneration of the epithelium begins. During this time, reparative and destructive processes may be present simultaneously. Complete resolution of the epithelial necrosis -7- Influenza Virus from Fields Virology probably takes up to a month, because pulmonary-function abnormalities persist beyond the period of symptomatic recovery from the acute phase (190). Immune Response to Infection Innate Immune Response Human influenza viruses replicate exclusively in superficial cells of the respiratory tract. They are released from the apical surface of the cell, which may limit more systemic spread but facilitate accumulation of virus in the lumen of the respiratory tract for transmission to the next susceptible host (37). The apical release of virus raises not yet explored questions of how antigen recognition and modulation of infection by antibody may occur. The extremely short incubation period between infection and clinical illness implies that innate immunity or preformed cognate recognition components are important. The respiratory tract has a series of protective mechanisms against influenza infection, including the mucin layer, ciliary action, and protease inhibitors that may prevent effective cell entry and virus uncoating. Once the epithelial cell is infected, proinflammatory cytokines, notably interleukin-6 (IL-6) and IFNand released from these cells. These cytokines reach their peak by day 2 after experimental infection (199). These two cytokines correspond in their release with the highest clinical symptom score, mucus production, fever, and viral load. Other cytokines either appeared later [IL-8 and tumor necrosis factor-2, or TGFimportance of IFN in regulation of influenza replication is suggested by the observation that the NS-1 protein is an IFN antagonist. Deletion of NS-1 leads to increased induction of IFN and a virus that is highly attenuated, except in a mouse with an interruption in the IFNinduction pathway (151). It is generally believed that IFN contributes to recovery from infection, and the early cytokine pattern directs the immune response toward a Th1 pattern (150). A transient increase in natural killer cell activity occurs after influenza infection (121,292). Cognate Immune Response Humoral Immunity In 80% of naturally acquired human infections, a serum antibody response can be documented (136). After primary infection, HA-specific antibodies of IgG, IgA, and IgM isotypes are detected, whereas in the secondary response, IgG and IgA antibodies predominate (47,349). B cells producing influenza virus–specific IgG, IgA, and IgM antibodies are present in the peripheral blood of normal individuals and of individuals undergoing infection with an influenza A virus (59,552). Serum antibody plays a role in resistance to or recovery from influenza illness in humans. A protective effect of transplacentally acquired antibody has been inferred from the observation that a significant direct correlation exists between age at the time of symptomatic influenza A -8- Influenza Virus from Fields Virology virus infection in infants and level of maternally transmitted antibody measured in cord serum (408). During infection of humans with influenza A virus, antibodies to the HA, NA, NP, and M proteins are produced (88,403). Antibodies to the HA and NA glycoproteins are associated with resistance to infection and/or illness in humans and in laboratory animals, whereas antibodies to the internal M1 and NP proteins are not (12). Passively transferred monoclonal antibody to the M2 protein is protective in mice, and M2 antibodies develop in humans infected with influenza A viruses (36,499). A universal influenza A vaccine has been proposed based on the extracellular domain of the M2 protein (364). Studies of vaccinia recombinant viruses expressing each of 10 gene products of the influenza A virus clearly identified the HA and NA glycoproteins as primary protective antigens, and the primary mediators of the resistance to virus challenge induced by these glycoproteins were antibodies (123). Because of the importance of antibodies to the surface glycoproteins in resistance to infection, only the antibody response to these proteins is discussed further. The reader is referred to four reviews that have considered immunity to influenza virus infection in detail (12,85,349,403). The level of serum antibody to the HA and NA correlates with resistance to illness and with restriction of the influenza virus replication in the respiratory tract of humans (76,352). This has been shown after experimental infection with influenza virus (76) or after natural infection (85). HA antibodies can prevent infection by neutralizing the infectivity of the virus (509), whereas NA antibodies mediate their antiviral effect primarily after infection has been initiated by restricting spread of virus within the respiratory tract of the host (453). It was previously thought that CD8+ T cells were solely responsible for clearance of virus during primary infection or during reinfection. However, it has been demonstrated that passively transferred antibodies can clear an influenza A virus infection in the absence of B or T cells in the host (442). Although immunity mediated by infection can be long lived, reinfection with antigenetically closely related influenza A viruses occurs, indicating that immunity against this highly infectious virus induced by a single infection can be incomplete (141,142,467). Two mechanisms have been identified that can contribute to this incomplete immunity. First, there is a gradual diminution in the total amount of serum (IgG), local IgA antibodies, or antibody-secreting cells within the first year after the first infection (239,240,545). Second, after infection with a new influenza virus subtype, antibodies are generated that react with only a limited number of antigenic sites on the HA glycoprotein, whereas after several infections, antibodies are generated that have a broad range of specificities (516). Consistent with this is the greater degree of resistance to infection with antigenic drift strains in humans previously infected twice with prototype virus than in those with only one previous infection (97). Cellular Immunity The role of cellular immunity in clearance of influenza virus has been well defined in the murine model but less well in humans (251). There are two subsets of effector lymphocytes in humans. The first subset consists of cells that mediate cytoxicity that is restricted by class I histocompatibility antigens and has the CD8+ phenotype. These -9- Influenza Virus from Fields Virology cytotoxic lymphocytes (CTLs) appear in the blood of infected or vaccinated individuals on days 6 to 14 and disappear by day 21 (122). Most studies have examined memory CTLs, which are detected in vitro by stimulation of peripheral blood lymphocytes with antigen. These CTLs exhibit a cross-reactive pattern of virus specificity (i.e., they lyse target cells infected with influenza A viruses belonging to any subtype, but not target cells infected with influenza B virus) (553). However, a more specific subpopulation of CTLs lyses only cells infected with homologous virus. Human class I–restricted CTLs recognize either glycoprotein HA or nonglycoprotein antigens (M, NP, PB2), which can account for their subtype-specific and cross-reactive specificities, respectively (134,553). Depending on human leukocyte antigen (HLA) haplotype, individuals can differ considerably in the antigens that their CTLs can recognize (321). The memory CTLs characterized after infection or vaccination of humans have the cross-reactive pattern of cytotoxicity (120,122). Passively transferred class I–restricted CTLs mediate recovery from influenza pneumonia in mice (553). The prechallenge level of memory CTLs did not correlate with susceptibility to infection or illness after experimental administration of wild-type virus, but it correlated with accelerated clearance of virus from the respiratory tract of humans (321). The other class of CTLs is restricted by histocompatibility class II antigens and has the CD4+ phenotype (248,472) and thus belong to the T-helper class of T cells. The CD4+ T cells have two functional properties. First, they are helper T cells, providing help both to B cells for antibody production and to class I–restricted CTLs for their proliferation (281,282,553). It is interesting to note that the helper T cells specific for M or NP antigen can provide help to B cells secreting HA antibody (282,283,441), and in this manner, can augment the antibody response to protective antigens. Second, the CD4+ T cells can have cytolytic activity, with a range of antigen specificities similar to those of class I–restricted CTLs (553). Little further is known of the role of these T cells in immunity in humans or of the kinetics of their responses after infection or vaccination. CD4+ and CD8+ T cells both can contribute to immunity to influenza A virus infection. The important role of CD4+ T cells in immunity to influenza virus infection has been defined from studies in CD8+ T cell–deficient animals, which can clear influenza A virus by a CD4+ T cell–dependent mechanism (28,116,295). Passively transferred influenza virus specific CD4+ T-cell clones are not able by themselves to clear an ongoing influenza virus infection, but require functional B cells to accomplish this clearance (442). Thus the primary antiviral activity of the CD4+ T cell is to provide help to B cells to produce antiviral antibodies. Because CD4+ T cells recognize many epitopes on influenza viral proteins, a large number of T cells are available to provide such help (66). CD8+ T cells also are able to mediate clearance of influenza A virus infection in CD4+ T cell–deficient animals (115,295). The CD8+ T cells not only clear infectious virus from experimentally infected animals, but also clear influenza virus RNA from lung tissue. Thus the immune system is functionally redundant in its ability to clear influenza A virus infections. Animals deficient in both CD4+ and CD8+ T cells succumb to infection, indicating that nonspecific mediators of immunity are not sufficient in the absence of T cells to restrict influenza A virus infection significantly (116,295). Although passively transferred CD8+ T cells that have been activated in vitro with influenza virus antigen can modify infection with influenza A virus, it remains problematic to induce protective - 10 - Influenza Virus from Fields Virology CD8+ T cells by immunization (287,475). The mechanisms by which influenza A virus CD8+ T-cell clones clear influenza A virus infections, be it by cytolysis or antiviral cytokine secretion, remains unknown. The number of CD8+ T-cell epitopes on viral proteins is much more restricted than the number of B-cell or CD4+ T-cell epitopes (30). Cytolysis of influenza virus–infected cells also can be mediated by antibody plus complement, and antibody-armed lymphocytes (195,409,434). Lymphproliferation is another measurement of a cellular response to influenza. Lymphocytes responsive to influenza antigens have been isolated from the blood and lower respiratory tract secretions of influenza virus–infected humans, but only the former have been studied extensively (244,553). Lymphocyte blastogenic responses to influenza antigens in humans increase after influenza A virus infection, beginning between the third and sixth day after infection (104), and return to baseline levels by day 28. Influenza antigen-specific cutaneous reactivity or in vitro blastogenesis in humans correlates weakly with susceptibility to infection with influenza A viruses (234). Influenza A virus infection can depress skin test reactivity to common antigens used to assess cutaneous delayed hypersensitivity (38,246,414). In addition, depression of the peripheral blood lymphocyte blastogenic responses to mitogenic and antigenic stimulation (104,246,292) is seen during the acute stage of infection and early convalescence. Despite this transient depression of delayed hypersensitivity and blastogenic responses to noninfluenzal antigens or mitogens, influenza virus–specific cellular responses develop (106,122). The mechanisms underlying the depression in the function of lymphocytes in influenza indicated earlier have not been defined, but influenza A virus can abortively infect human lymphocytes in vitro (48) and possibly in vivo (537). Mucosal Antibody Response Francis (140) was the first to detect neutralizing activity to influenza virus in nasal secretions, and subsequently, resistance to experimental influenza A virus infection in the mouse was found to be mediated primarily by antibody present in bronchial secretions (128). The neutralizing antibody in nasal secretions of humans is primarily of the immunoglobulin A (IgA) isotype (11) and is locally produced (431). Antibody to both the HA and NA can be detected in local secretions, but the former is easier to detect and thus has been studied more frequently (85). Furthermore, IgA antibodies, which are the primary mediators of resistance to influenza A virus infection in the upper respiratory tract, can act intracellularly to inhibit replication of virus and likely actively participate in clearance of infectious virus from the epithelial cells of the respiratory tract (314,315,416,417). During primary viral infection, IgA, IgG, and IgM hemagglutinin-specific enzymelinked immunosorbent assay (ELISA) antibodies appear in nasal washes, with IgA and IgM antibodies detected more frequently than IgG antibody (349,353). Most of the HA-specific IgA and IgM antibodies are actively secreted locally, whereas local secretion could be demonstrated only infrequently for IgG antibody. Individuals with a local IgA response also had a serum IgA response. Local IgA antibody stimulated by natural infection is detectable for 3 to 5 months after infection, and there is local IgA memory for influenza antigen (349,545). After secondary infection, local antibody is also - 11 - Influenza Virus from Fields Virology primarily of the IgA isotype. Again, those individuals with a local IgA response also have a serum IgA response, and the magnitude of the serum IgA HA antibody response correlates with that of the local response. Nasal wash IgG appears to be predominantly a transudate from serum, with a serum-to-nasal wash concentration gradient of 350:1 (353). The presence of local IgA antibody induced by infection with an attenuated virus correlated with resistance of volunteers to infection and illness after challenge with a virulent wild-type virus (239). Challenge of children with an attenuated live vaccine showed similar findings (40). Resistance to experimental wild-type infection also correlated with the level of local HA antibody present at the time of virus administration, with IgG and IgA each contributing to resistance (76). Effect of Infection on Bacterial Flora and Phagocytic Cell Function Influenza A virus infection does not generally significantly alter the normal bacterial flora (39,102); however, several exceptions have been noted. In patients with chronic bronchitis, influenza A virus infection was followed by an increased incidence of colonization with Streptococcus pneumoniae (463). During an outbreak of meningococcal and influenza A virus infections, influenza virus infection was found to be significantly associated with infection or carriage of Neisseria meningitidis (554). Furthermore, pharyngeal cells from experimentally infected volunteers demonstrated an increased adherence for pathogenic bacteria during acute disease (124). Infection of human polymorphonuclear (PMN) and mononuclear (MN) leukocytes with influenza A virus in vitro depresses the ability of these cells to respond to a chemotactic stimulus (1,63). During influenza A virus infection in humans, PMN and MN leukocytes obtained from peripheral blood also exhibit depressed chemotaxis in vitro (1). Phagocytosis has generally not been affected by infection of PMN or MN leukocytes in vitro, but infection does decrease bactericidal capacity of the phagocytic cells (1). Similar findings have been reported in experimental animals, although not by all investigators (377,438). Influenza A virus infection of macrophages in vitro can inhibit their ability to help or augment the proliferative response of lymphocytes to mitogens (422). Perhaps these virus-related alterations in phagocytic cell function act in concert with the destruction of the ciliated epithelium to set the stage for the secondary bacterial infections that can occur during influenza virus infections of humans. Other Antivirals Against Influenza Interferon and IFN inducers induce resistance to influenza infection in mice (60,157,484). In humans the administration of exogenous IFN or an IFN inducer before experimental or natural challenge with a virulent influenza virus fails to reduce the level of illness or the quantity of virus shed (212,327). Studies with recombinant IFNindicate slight protection against illness and virus shedding (496). Copyright © 2001 by Lippincott Williams & Wilkins - 12 - Influenza Virus from Fields Virology Source of information: Please do not distribute as this is copyrighted material. Tx! Kevin Knipe, D., and Howley, P., eds. (2001). Fields Virology. Lippincott Williams & Williams, Philadelphia, PA. - 13 -