post sedation instructions - EXTRANET
advertisement

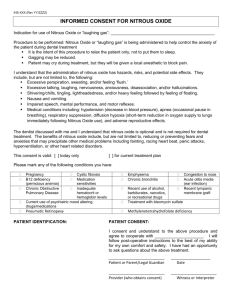
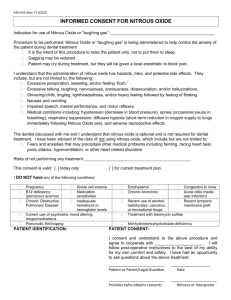
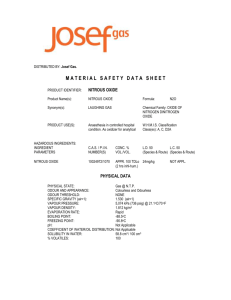
Emergency Department Use of NITROUS OXIDE ANALGESIA Background Nitrous oxide (N2O) is a sweet smelling inorganic gas that was first prepared by Priestly in 1772. Soon after Davy described the pleasurable effects of inhaling the gas and suggested its use during surgery, but it wasn’t until the late 1800s that its analgesic properties were exploited for use during dental procedures. Its popularity continues today with its use as an analgesic gas in ambulances, labour wards and dental offices, and in operating theatres as a supplement to general anaesthesia. The efficacy of nitrous oxide in providing analgesia and sedation for painful procedures in children has been well proven. The rapid onset of action and rapid return to normal state after discontinuation of nitrous oxide makes it a particularly useful agent for analgesia for short procedures in the emergency department. Analgesia equivalent to morphine follows the inspiration of 20% nitrous oxide. Some patients may lose consciousness when breathing as little as 30% nitrous oxide in oxygen, and most will become unconscious at 80%. As well as causing depression of the central nervous system, N2O also may have a depressant effect on the cardiac and/or respiratory systems1. The sedation caused by nitrous oxide may exacerbate existing airway obstruction. Although generally regarded as a benign agent nitrous oxide has significant side effects. Inappropriate usage has potential for fatality7. It is 40 times more soluble in blood than nitrogen, giving it the capacity to rapidly diffuse into closed gas spaces within the body, exerting pressure effects locally. This is especially important in the presence of a pneumothorax. With prolonged exposure nitrous oxide can cause megaloblastic anaemia and subacute combined degeneration of the spinal cord through its affects on vitamin B12 metabolism1,7. Twelve hours exposure to 50% nitrous oxide will cause mild megaloblastic bone marrow changes in healthy patients, but the required exposure time is reduced in seriously ill patients, and in those subjected to repeated exposure16. Prolonged staff exposure can in addition increase the risk of malignancy, and have reproductive implications if the waste gases are not adequately scavenged 7. Two recent large prospective studies examined adverse events related to the use of nitrous oxide for procedural sedation in children3,4. Of the 7679 children in the studies, 27 had major adverse events (a rate of 0.35%). Major adverse events included oxygen desaturation, airway obstruction, apnoea, bradycardia and oversedation (loss of verbal contact during the procedure or persistence of sedation for longer than 5 minutes after discontinuation of the anaesthetic). All events resolved within minutes after discontinuation of nitrous oxide inhalation and no serious complications ensued. A higher adverse event rate was reported in children younger than 1 year (2.3%), and in those who received additional psychotropic drugs. Minor adverse events such as euphoria, nausea, vomiting, dizziness and paraesthesia were reported more frequently and occurred in approximately 5% of cases. Despite these drawbacks, if used appropriately nitrous oxide has proven itself to be a very useful analgesic and sedative agent. Updated: Jan 2004 Nitrous Oxide Guidelines Page 1 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Nitrous Oxide Delivery Systems Nitrous Oxide may be delivered by two different methods in the RCH Department of Emergency Medicine: 1. Entonox - in a fixed concentration of 50% N2O / 50% O2 in a single cylinder. Entonox is administered via a demand valve system with a weighted mask. 2. The Matrix Quantiflex nitrous oxide delivery system – can deliver a variable concentration of N2O (0-70%) with oxygen administered via a constant gas flow system that does not require patient effort to trigger nitrous oxide delivery. In the two studies mentioned previously3,4 nitrous oxide was administered in a fixed concentration of 50% with oxygen via a demand valve system. The Matrix Quantiflex can administer up to 70% nitrous oxide, and theoretically could have a higher risk of adverse events. There is a paucity of large studies in the literature looking at adverse events related to the use of this concentration administered outside the operating room environment. The Children’s Hospital Westmead in Sydney currently uses the Matrix Quantiflex device, and has an ongoing audit monitoring their adverse events. They currently do about 2000 nurse administrations a year using this device, and have had no mortality or major morbidity using their current guidelines#. They recently published a study5 looking at the safety of this device using 50 to 70% nitrous oxide concentrations administered by trained nursing staff for painful procedures in 90 children. They reported the adverse events of oxygen desaturation (SaO2 < 95%) 8.9%, vomiting 7.8%, excitement 4.4% and dysphoria 2%. The second important difference lies in the administration technique. Entonox delivered via a demand valve system relies on self-administration, making oversedation less likely but limiting its application in young children. The Matrix Quantiflex device is a constant gas flow system that does not require patient effort to trigger nitrous oxide delivery. This makes it inherently less safe than a demand valve system, requiring constant supervision by a dedicated Administrator monitoring the patients level of consciousness. It also means that oversedation and respiratory depression may occur, necessitating the availability of ventilation and resuscitation equipment. The Children’s Hospital Westmead uses a Bain rebreathing circuit to deliver the gas to the patient. This introduces the risk of rebreathing carbon dioxide with further sedation if inadequate gas flows are delivered. Current guidelines at the Children’s Hospital Westmead are that flows of 6L/min be maintained in those less than 20kg, and 8L/min in those greater than 20kg6. Because of the greater risk of excessive sedation with continuous flow devices, it is essential that the Administrator have as their sole responsibility, the care of the patient. Careful observation and maintenance of consciousness are paramount to the safety of the technique7. Updated: January 2004 Nitrous Oxide Guidelines Page 2 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Guidelines for use of Entonox in the Emergency Department General Parents should be given a Nitrous Oxide Parent Information sheet and given the opportunity to ask questions regarding the procedure. Informed consent for the procedure and for the sedation must be obtained. A written record (Sedation Record) detailing the duration and concentration of nitrous oxide administered, monitored patient variables, and any complications encountered should be completed with one copy filed in the patient chart and a second copy kept for audit purposes (Appendix 2). Staff Requirements At least two staff members (medical or nursing) must be in the procedure room at all times during the administration of N2O. The Administrator must either be a) a Registered Nurse with at least 12 months paediatric experience who has successfully completed the Entonox Administration Learning Package or b) a medical officer of Registrar level or above who is experienced in the use of Entonox in children Female Administrators should not administer nitrous oxide during the first trimester of pregnancy. Facilities Nitrous oxide should be administered in either the Minor Procedure Room or the Resuscitation Room. It is not to be given in the Plaster Room or at the patient bedside in other areas. The Administrator is responsible for ensuring that the resuscitation trolley (including appropriately sized self-inflating bag and mask) is present in the room prior to commencing the sedation Indications for use in DEM Nitrous oxide may be suitable for use when short acting analgesia/sedation is required for brief procedures: Injection of local anaesthetic for suture repair Foreign body removal from ear, soft tissues Abscess incision & drainage Wound care & dressing change Insertion of intravenous cannula in certain circumstances Simple moulding of Plaster of Paris cast to fracture Reduction of digit dislocation Use of Entonox should be restricted to children aged over 4 years of ASA physical class I or II (Appendix 1). It should not be used in conjunction with other sedatives/analgesics without a Registrar or Consultant present. Patients should be kept nil by mouth leading up to the procedure and if possible should be fasted for at least 2 hours prior to the procedure. Updated: January 2004 Nitrous Oxide Guidelines Page 3 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Contraindications for use in DEM Nitrous oxide is not appropriate for use in the following circumstances: Suspicion of pneumothorax Intestinal ileus, abdominal distension or bowel obstruction Sinusitis Decompression sickness or air embolism Intrathoracic injury, dyspnoea or cyanosis Closed head injury or raised intracranial pressure Impaired conscious level prior to procedure Acute asthma or pneumonia Airway obstruction or history of difficult airway ASA physical class III to V (Appendix 1) Maximum continuous patient exposure to nitrous oxide should be no more than 2 hours once per week. Monitoring Pulse oximetry with an audible alarm and appropriate alarm limits must be used. The Administrator should maintain constant attention to the patient’s level of consciousness, breathing and airway patency. RR, PR, BP, O2 saturation and Sedation Score should be recorded on the Sedation Record every 15 minutes during the procedure. Technique A new disposable Mid O Gas circuit (Parker Healthcare part number MC/3200/F) and facemask or mouthpiece is to be used for each administration. This equipment is kept in the locked cupboard in the Minor Procedure Room. The Entonox device should be assembled and checked by the Administrator prior to each administration. The level of gas in the Entonox cylinder should be checked – if less than ¼ full (red zone) it should be replaced. Check the cylinder is firmly attached to the regulator pipe and that an appropriately sized mask has been chosen. The Entonox cylinder may then be turned on. The patient should then self-administer the gas via the facemask. A “hissing” sound on inspiration indicates correct use and adequate flow of gas. Administration should start at least 3 minutes prior to starting the planned procedure. A level of sedation approximating a Sedation Score of 2-3 is the objective (aim for analgesed but not asleep). Administration should be temporarily discontinued if the patient becomes excessively drowsy. At the end of the procedure (or if the facemask is removed for a period of >30 seconds) 100% oxygen should be delivered for 3 minutes. At the end of the procedure the Entonox cylinder should be turned off and the tubing and facemask should be removed for cleaning. The Administrator must ensure that the Sedation Record is complete and that the patient’s parent/s have been given the Post Sedation Guidelines sheet (Appendix 4) The patient may be discharged once they meet the following discharge criteria: Return to normal (presedation) level of consciousness Normal gait Normal speech Updated: January 2004 Nitrous Oxide Guidelines Page 4 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Guidelines for use of the Matrix Quantiflex device in the Emergency Department General Parents and, if appropriate, patients should be informed about the reasons for using N2O for the procedure Parents should be given a Nitrous Oxide Parent Information sheet and given the opportunity to ask questions regarding the procedure. Informed consent for the procedure and for the sedation must be obtained. A written record (Sedation Record) detailing the duration and concentration of nitrous oxide administered, monitored patient variables, and any complications encountered should be completed with one copy filed in the patient chart and a second copy kept for audit purposes (Appendix 2). Staff Requirements At least two staff members (medical or nursing) must be in the procedure room at all times during the administration of NO2. Administration of N2O via the Matrix Quantiflex system in the emergency department will be restricted to those who have the requisite skills in advanced paediatric airway management and who have satisfactorily completed a training program in the use of the device. Only the following staff are permitted to administer N2O via the Matrix Quantiflex system in the emergency department: c) DEM Consultant d) DEM Clinical Fellow e) Other Registrar or Consultant level staff approved/certified by the ED Director to use the equipment Female Administrators should not administer nitrous oxide during the first trimester of pregnancy. Facilities Nitrous oxide should be administered in either the Minor Procedure Room or the Resuscitation Room. It is not to be given in the Plaster Room or at the patient bedside in other areas. The Administrator is responsible for ensuring that the resuscitation trolley (including appropriately sized self-inflating bag and mask) is present in the room prior to commencing the sedation Updated: January 2004 Nitrous Oxide Guidelines Page 5 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Indications for use in DEM The Matrix Quantiflex system allows administration of N2O to a younger group of children than those who are sufficiently cooperative and who have a sufficiently negative inspiratory pressure to trigger the Entonox demand valve system. Nitrous oxide may be suitable for use when short acting analgesia/sedation is required for brief procedures: Injection of local anaesthetic for suture repair Foreign body removal from ear, soft tissues Abscess incision & drainage Wound care & dressing change Insertion of intravenous cannula in certain circumstances Simple moulding of Plaster of Paris cast to fracture Reduction of digit dislocation Use of N2O via the Matrix Quantiflex system is restricted to children aged over 1 year of ASA physical class I or II (Appendix 1). It should be used with caution in children who have received other sedatives/analgesics. Patients should be kept nil by mouth leading up to the procedure and if possible should be fasted for at least 2 hours prior to the procedure. Contraindications for use in DEM Nitrous oxide is not appropriate for use in the following circumstances: Suspicion of pneumothorax Intestinal ileus, abdominal distension or bowel obstruction Sinusitis Decompression sickness or air embolism Intrathoracic injury, dyspnoea or cyanosis Closed head injury or raised intracranial pressure Impaired conscious level prior to procedure Acute asthma or pneumonia Airway obstruction or history of difficult airway ASA physical class III to V (Appendix 1) Maximum continuous patient exposure to nitrous oxide should be no more than 2 hours once per week. Monitoring Pulse oximetry with an audible alarm and appropriate alarm limits must be used. The Administrator should maintain constant attention to the patient’s level of consciousness, breathing and airway patency. RR, PR, BP, O2 saturation and Sedation Score should be recorded on the Sedation Record every 15 minutes during the procedure. Updated: January 2004 Nitrous Oxide Guidelines Page 6 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Technique A new disposable Mid O Gas circuit (Parker Healthcare part number MC/5000/F) and facemask is to be used for each administration. This equipment is kept in the locked cupboard in the Minor Procedure Room. The Matrix Quantiflex device should be assembled and checked by the Administrator prior to each administration according the Matrix Quantiflex N2O Machine Checklist (see Appendix 3). The suction connection to the scavenging system should be set on low flow. The Matrix Quantiflex device is not to be used without gas scavenging. The N2O supply may then be turned on and the flowmeters adjusted to provide 50% oxygen at a total flow of 8 L/min (ie. N2O @ 4 L/min + O2 @ 4 L/min). This starting point represents the minimum gas flow to be used for patients. The patient should then commence breathing the gas via the facemask. If possible, allow the patient to hold the mask. Administration should commence at least 3 minutes prior to starting the planned procedure. A level of sedation approximating a Sedation Score of 2-3 is the objective (aim for ‘analgesed’ but not asleep). Administration should be temporarily discontinued if the patient becomes excessively drowsy. Frequent communication with the patient allows rapid titration of the N2O percentage for effect. At the end of the procedure (or if the facemask is removed for a period of >30 seconds) 100% oxygen should be delivered for 3 minutes. At the end of the procedure the cylinders should be closed and the suction may be turned off. The facemask should be removed for cleaning and the circuit should be placed in a non-contaminated waste bin. The Administrator must ensure that the Sedation Record is complete and that the patient’s parent/s have been given the Post Sedation Guidelines sheet (Appendix 4) The patient may be discharged once they meet the following discharge criteria: Return to normal (presedation) level of consciousness Normal gait Normal speech We gratefully acknowledge the assistance of Dr David Hill in the preparation of this document and the Departments of Emergency Medicine at Sydney Children’s Hospital, Children’s Hospital Westmead and Royal Children’s Hospital Melbourne for providing their Nitrous Oxide Administration guidelines. Updated: January 2004 Nitrous Oxide Guidelines Page 7 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) References 1. Marshall BE, Longnecker DE: General Anaesthetics. In: Gilman GA, Rall TW, Nies AS, Taylor P. (eds):1992 The pharmacologic basis of therapeutics (8th ed) McGraw-Hill, Singapore, ch 14 pp285-310. 2. Committee on Drugs, American Academy of Pediatrics. Guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures. Pediatrics 1992;89:1110-5. 3. Pena BM, Krauss B: Adverse events of procedural sedation and analgesia in a pediatric emergency department, Ann Emerg Med 1999;34:483-91. 4. Gall O, Annequin D, Benoit G, Van Glabeke E, Vrancea F, Murat I: Adverse events of premixed nitrous oxide and oxygen for procedural sedation in children, Lancet 2001;358:1-2 5. Kanagasundaram SA, Lane LJ, Cavalletto BP, Keneally JP, Cooper MG: Efficacy and safety of nitrous oxide in alleviating pain and anxiety during painful procedures, Arch Dis Child 2001;84:492-495. 6. Nitrous oxide guidelines, Department of Anaesthesia and Pain Management, The Royal Children’s Hospital, Westmead, Updated May 2000. 7. Keneally J: Nitrous Oxide Analgesia. In: McKenzie I, Gaukroger P, Ragg P, Brown T. (eds): 1997 Manual of Acute Pain Management in Children. Churchill Livingstone, New York, ch 4, pp. 17-24. 8. Australian and New Zealand College of Anaesthetists, Policy Document PS9. Guidelines on conscious sedation for diagnostic, interventional medical and surgical procedures, 2001. 9. Cote CJ: “Conscious sedation”:Time for this oxymoran to go away! Journal of Pediatrics 2001; 139:1-5. 10. Litman RS, Kottra JA, Verga KA, Berkowitz RJ, Ward DS: Chloral hydrate sedation: The additive sedative and respiratory depressant effects of nitrous oxide, Anesth Analg 1998;86:7248. 11. Cote CJ, Karl HW, Notterman DA, Weinberg JA, McCloskey C: Adverse sedation events in pediatrics: Analysis of medications used for sedation, Pediatrics 2000;106:633-645. 12. American Society of Anaesthesiologists. Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists. Anesthesiology 1996;84:459-71. 13. Donaldson D, Meechan JG. The hazards of chronic exposure to nitrous oxide. British Dental Journal 1995;178:95-100. 14. Shaw AD, Morgan M. Nitrous Oxide: time to stop laughing? Anaesthesia 1998;53:213215. 15. Girdler NM. The demise of nitrous oxide- fine for anaesthesia, but what about sedation? Anaesthesia 1998;53:711-723. 16. Baden JM, Rice SA. Metabolism and Toxicity. In Miller RD (editor): Anesthesia 4th ed, 1994. Churchil Livingstone, New York, ch8, p172. # Personal communication, Dr Michael Cooper, Deputy Head, Pain and Palliative Care Service, Children’s Hospital, Westmead, Sydney Updated: January 2004 Nitrous Oxide Guidelines Page 8 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Appendix 1 : ASA Physical Class The American Society of Anesthesiologists (ASA) has produced guidelines for assessing the physical status of patients pre-operatively. ASA Class 1 Normal healthy patient 2 Patient with mild systemic disease 3 Patient with a severe systemic disease that limits activity but is not incapacitating 4 Patient with an incapacitating systemic disease that is a constant threat to life 5 Moribund patient not expected to survive for 24 hours Updated: January 2004 Nitrous Oxide Guidelines Page 9 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Appendix 2 : Sedation Record (Please place patient label here) UR. No. _________________________________________ Surname:________________________________________ Given Names:_____________________________________ Royal Children’s Hospital and Health Service District DOB:_____________________________ Sex: F M PROCEDURAL SEDATION FORM PROCEDURE DATE: / / PROCEDURE:____________________________________________________ Pre-Sedation Checklist Discussed with patient/guardian Information Sheet for specific agent (if available) given to patient/guardian - Reasons for sedation No contraindications to use of sedative agent (see guidelines) - Expected effects of agent/s Consent Obtained - Potential adverse events Pre-Procedure Details Patient’s Weight: Patient last ate: Sedative/analgesic agent administered in last 4 hours: Patient last Drank: Agent:: __________________ Dose: ______ Time: _______ Procedure Details Procedure Performed By:______________________________ Sedation administered by:_______________________ DRUGS USED: (Write order on Medication Sheet) Date & Time Given Drug Name Route Dose Duration OBSERVATIONS: Time N2O% O2 (L/min) O2Sat EtCO2 RR HR BP SS Assessment of Procedural Sedation: Excellent Adequate Poor Adverse Events: Vomiting Apnoea (>10 secs) Bradycardia Desaturation (<95%) Over Sedation Excessive Salivation Emergence agitation Other (Please State) ________________________ Management of Adverse Event: Laryngospasm _____________________________________________________________________________________ __________________________________________________________________________________________________________________ Post-Procedure Orders Home (once normal gait, normal speech, normal conscious level, no nystagmus) Oximetry for 1 hour post procedure RR,PR,BP,SS q15min for 1 hour Remain NBM Post-Procedure advice sheet given Other: _______________________________________________________ Name:________________________ O2 via facemask of O2 Sat <95% & notify MO Signature:______________________________ Date: Designation:________________________________________ Updated: January 2004 Nitrous Oxide Guidelines Page 10 of 12 / / Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Appendix 3 : Matrix Quantiflex N2O Machine Checklist To be performed by Administrator before Machine use Prepare & check Machine: Pipelines for O2 (white) and N2O (blue) correctly attached at cylinder and machine ends Turn on cylinders and check contents of O2 cylinder (black & white) and N2O cylinder (blue) adequate (not in red portion of dial). Set Mixture Dial to 30% O2 and turn up Flow Control Valve. Ensure that when N2O flowmeter shows 7L/min, O2 flowmeter shows at least 3L/min. Turn off O2 cylinder (black & white) – both O2 and N2O flowmeter readings should drop to zero. Turn O2 cylinder back on. Port below gas outlet is sealed by plug & black bag. Check seal by occluding gas outlet and ensuring no leak present. Check that O2 flush button is operational. Attach and check Circuit & Scavenging: Attach white arm of Mid O Gas circuit to gas outlet and attach blue arm of Mid O Gas circuit to suction trap at rear of machine. Attach suction piping from suction trap to wall suction unit. Check that components correctly fitted. Check that suction is set on low flow rate. Updated: January 2004 Nitrous Oxide Guidelines Page 11 of 12 Department of Emergency Medicine, Royal Children's Hospital (Brisbane) Appendix 4 : Post Sedation Guidelines PARENT INFORMATION SHEET POST SEDATION INSTRUCTIONS Your child has been given a sedative drug during their visit to the Emergency Department today. The name of this drug is ………………………….. Medicines of this type may cause your child to: be sleepy or less aware not think clearly be more likely to lose their balance or fall Because of this, he or she should be watched closely for the next 8 hours. Also, please observe the following: Your child should not take part in activities that require normal childhood coordination such as bicycle-riding, skating, roller-blading, playing on swings or monkeybars for the next 24 hours For the next 8 hours, your child should not play outside unless supervised by a responsible adult Your child should not have a bath/shower, cook, or use any possibly dangerous electrical devices without a responsible adult to watch them in the next 8 hours If you notice anything unusual about you child or have any questions, please phone the RCH Emergency Department on (07) 3636 8085 and ask to speak to the Emergency Registrar. Updated: January 2004 Nitrous Oxide Guidelines Page 12 of 12