HEP_23533_sm_suppmat
advertisement

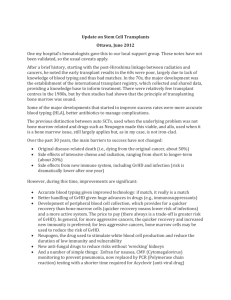
McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 1 Supporting Material HEPATOBILIARY COMPLICATIONS OF HEMATOPOIETIC CELL TRANSPLANT, 40 YEARS ON George B. McDonald, M.D. Gastroenterology/Hepatology Section, Fred Hutchinson Cancer Research Center and the Department of Medicine, University of Washington School of Medicine, Seattle, Washington, U.S.A. Contents: Three figures; four appendices. Correspondence to: George B. McDonald, M.D. Gastroenterology/Hepatology Section (D2 – 190) Fred Hutchinson Cancer Research Center 1100 Fairview Avenue North P.O. Box 19023 Seattle WA 98109 – 1024 Telephone 206 667 6932 Email gmcdonal@fhcrc.org McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 2 THREE SUPPORTING FIGURES TO ACCOMPANY THESE FIGURE LEGENDS SUPPORTING FIGURE 1. Histology of Sinusoidal Obstruction Syndrome (SOS) after myeloablative hematopoietic cell transplant. A. Zone 3 of the liver acinus in an early phase of SOS, with disruption of sinusoidal anatomy, red blood cells extending through the space of Disse, hepatocyte necrosis, and subendothelial edema in a patent central vein (CV) (H&E). B. Extensive hepatocyte necrosis and dropout, disruption of sinusoids, extravasation of red blood cells throughout zone 3, and subendothelial fibrosis (Masson trichrome). C. Alpha actin-positive stellate cells within zones 2 and 3 that contain areas of extensive hepatocyte necrosis; periportal hepatocytes are intact (PV, portal vein) (alpha-smooth muscle actin immunohistology). D. A later phase of SOS, showing extensive collagenization of sinusoids adjacent to two central veins, with hepatocyte dropout and extinction of hepatocyte cords in between the veins (Masson trichrome). E. Central vein and zone 3 hepatocytes later after transplant, illustrating eccentric phlebosclerosis and collagen deposition in sinusoids (Masson trichrome). F. Lower power view of confluent fibrosis in and around adjacent central veins, with central to central bridges forming a picture of “reverse” cirrhosis two months after transplant (Masson trichrome). (Photomicrographs by Howard M. Shulman, M.D.) McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 3 SUPPORTING FIGURE 2. Histology of graft-vs.-host disease (GVHD) involving the liver. A. Portal area showing small bile ducts (arrows) with a distorted appearance, lymphocyte infiltration, and epithelial drop-out (H&E). B. Small bile ducts, showing dysmorphic features, cytoplasmic eosinophilia, apoptosis (arrow), atypical nuclei, and lymphocytic infiltration (H&E). C. Liver lobules from a patient with severe multisystem acute GVHD, showing fibrotic portal spaces and periportal bile thrombi (arrows) (Masson trichrome). D. Immunohistochemical stain for cytokeratin 19 in a patient with longstanding liver GVHD, illustrating ductular reaction at the periphery of a portal but without an identifiable interlobular bile duct. E. A portal space showing absence of recognizable bile duct epithelium in a patient with longstanding refractory chronic GVHD (H&E). F. Diffuse lobular inflammation, from a patient with a hepatitic onset of GVHD following discontinuation of immunosuppressive drug therapy (H&E). (Photomicrographs by Howard M. Shulman, M.D.) McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 4 SUPPORTING FIGURE 3. Infections in the liver following hematopoietic cell transplant. A. Fungal liver abscesses demonstrating the variability of findings in different samples. On the left, a sterile healing abscess with a necrotic center devoid of fungal elements, surrounded by inflammatory cells and a pseudo-capsule (asterisk) (H&E). On the right, an acute abscess with a small focus of red-staining fungal elements (arrow) in a field of degenerative neutrophils, surrounded by a pseudo-capsule (PAS). B. Immunohistochemistry for hepatitis B core antigen, in a patient with fulminant hepatitis B after transplant, showing extensive periportal hepatocyte cytoplasmic and some nuclear staining. C. Focal microabscess (arrow) in the liver lobule caused by cytomegalovirus, in which lymphocytes and neutrophils are seen adjacent to enlarged, brick-red cells containing CMV (H&E) D. Confluent hepatocyte necrosis caused by Adenovirus infection; in the rim of hepatocytes surrounding the necrotic area are darker “smudged nuclei” typical of Adenovirus (H&E). E. Confluent hepatcyte necrosis (upper right) caused by Varicella Zoster Virus infection, with absence of PAS staining of necrotic cells. F. Diffuse infiltration by plasmacytoid cells and immunoblasts with displacement of portal structures, caused by Epstein-Barr Virus lymphoproliferative disease (H&E). (Photomicrographs by Howard M. Shulman, M.D.) McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 5 SUPPORTING APPENDIX 1. OVERVIEW OF HEMATOPOIETIC CELL TRANSPLANTATION. For in-depth reading on this subject, I recommend this textbook: Appelbaum FR, Forman SJ, Negrin RS, Blume KG. Thomas' Hematopoietic Cell Transplantation. 4th ed. Oxford, UK: Wiley-Blackwell Publishing, 2009. There are three sources of hematopoietic cells used in HCT: 1) A person’s own cells, harvested by either bone marrow aspiration or by apheresis of growth factor-mobilized peripheral blood (autologous transplant). There are only two indications for autologous transplant: malignant disorders requiring high-intensity chemotherapy (with or without radiation therapy) that would otherwise destroy marrow function, and some autoimmune diseases under experimental protocols (for Crohn’s disease, systemic sclerosis, and multiple sclerosis, for example). If a malignancy involves the marrow, an autologous transplant containing easily detected numbers of malignant cells is contraindicated. If a patient has an autoimmune disease, the hypothesis being tested is that high-dose, myeloablative chemotherapy followed by infusion of autologous hematopoietic cells will reset the “immunostat” and result in less inflammation. 2) Some one else’s cells, again harvested from either marrow or peripheral blood (allogeneic transplant or, if an identical twin is available, syngeneic transplant). The ideal allogeneic donor is an HLA-matched sibling, but patients without matched siblings can have transplants from family members who are not siblings or from unrelated donors who are HLA-matched with the patient. These unrelated donors are identified from McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 6 international registries of people who have volunteered to be HLA-typed and who are willing to have their hematopoietic cells harvested. There are many different indications for allogeneic or syngeneic transplant: malignant disorders such as leukemia, lymphoma, and myeloma; genetic disorders involving hematopoietic cells, immune cells, or cells derived from these lineages; and some acquired hematologic disorders such as aplastic anemia. Allogeneic cells can be infused after a myeloablative conditioning regimen, resulting in complete hematopoietic cell chimerism (see the glossary in Supporting Appendix 2), or after a reduced-intensity regimen, resulting in mixed host-donor hematopoietic cell chimerism. The original intent of allogeneic transplantation was to rescue patients whose marrow had been obliterated by high-dose anti-cancer therapy in the conditioning regimen, where the anti-cancer therapy was thought to be the primary modality that obliterated tumor cells. It is now apparent that allogeneic donor cells can have significant effects on tumor cells, resulting in graft-vs.-tumor or graft-vs.-leukemia effects. All recipients of allogeneic hematopoietic cells must receive prophylactic immune suppressive drugs to prevent acute graft-vs.-host disease. 3) Hematopoietic cells from the umbilical cord of a newborn infant (cord blood transplant). Although hematopoietic cells obtained from cord blood are by definition allogeneic to any patient into whom they are infused (other than the same newborn, but later in life), these cells are immunologically immature, and are somewhat less prone to cause acute graft-vs.-host disease. Most cord blood cells are HLA-mismatched with the patient into whom they are infused. All recipients of allogeneic cord blood cells must receive prophylactic immune suppressive drugs to prevent acute graft-vs.-host disease. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 7 Two types of conditioning therapy are used to prepare patients for the infusion of hematopoietic cells. Without this conditioning therapy, a donor’s allogeneic cells would be rejected by the recipient’s immune cells. In patients with a malignant disorder, the conditioning regimen usually contains chemotherapy agents or radiation doses that have anti-tumor effects in addition to their immune suppressive effects. 1) Myeloablative conditioning therapy may consist of many different combinations and doses of chemotherapy drugs, with or without irradiation. Irradiation can be given as Total Body Irradiation (from 10 to 16 Gy) or as radiolabeled antibodies designed to target antigens on tumor cells. As noted in the body of this review, while all myeloablative regimens are effective in obliterating virtually all hematopoietic and immune cells, not all myeloablative conditioning regimens have equivalent organ toxicity, including liver toxicity. 2) Reduced-intensity conditioning therapy consists of lower doses of chemotherapy and immune-suppressive drugs, usually combined with lower dose Total Body Irradiation (for example, 2-4 Gy). The intent is to prevent rejection of donor allogeneic cells so that mixed chimerism can be established. In patients with malignant disorders, particularly leukemia and lymphoma, donor allogeneic cells can eliminate hematopoietic cells, immune cells and malignant cells of recipient origin, thus, achieving complete hematopoietic cell chimerism and clearing of malignant cells. While this is the desired effect of reduced-intensity allografting for malignant disorders, this result is not always achieved. Current research examines the biology of graft-vs.-tumor effects and methods to achieve more predictable anti-tumor effects after allogeneic transplant. In patients McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 8 with certain non-malignant hematologic disorders and in-born errors of metabolism, mixed hematopoietic chimerism is sufficient to correct phenotypic defects and “cure” the underlying disorders. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 9 SUPPORTING APPENDIX 2. GLOSSARY OF COMMONLY USED TERMS AND JARGON WORDS IN THE FIELD OF HEMATOPOIETIC CELL TRANSPLANTATION. TERM OR JARGON WORD MEANING REFERRING TO THE PREPARATION OF PATIENTS FOR TRANSPLANTATION Conditioning (as “conditioning Treatment with drugs and/or irradiation to achieve anti- therapy”, “the conditioning tumor and immune suppressive effects. Conditioning regimen”, “cytoreductive therapy”, regimens can be myeloablative (lethal doses that ablate or “the preparative regimen”) marrow cells) or of reduced-intensity (lower doses where the goal is immune suppression that avoids some of the toxicity of myeloablative regimens, allowing mixed hostdonor chimerism to be achieved after transplant). TBI, total body irradiation Irradiation usually given by linear accelerator, with total doses from 10 - 14 Gy (~1000 – 1400 rad) for myeloablative regimens, and from 2-4 Gy (200 – 400 rad) for reduced intensity regimens. The dose rate and the schedules of delivery (single dose, fractionated, hyperfractioned) vary widely around the world. TLI, total lymphoid irradiation Therapeutic irradiation selectively delivered to the spleen and anatomic sites that harbor lymph nodes, including the neck, mediastinum, supraclavicular regions and axillae (“mantle”), periaortic, iliac, and femoral (“inverted Y”) regions. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) TMI, total marrow irradiation page 10 Therapeutic irradiation selectively delivered to marrow sites, including the spine, pelvis, and proximal long bones, sometimes delivered as radioisotopes through the use of bone-seeking agents. Abbreviations for individual BU, busulfan; TBU, targeted busulfan; CY, cytoreductive drugs used in cyclophosphamide; FLU, fludarabine; MEL, melphalan; conditioning regimens TT, thioTEPA; VP-16, etoposide ATG, antithymocyte globulin, aka Potent anti-T cell antibody made by immunizing rabbits thymoglobulin or horses with human cells; can be used as an immunosuppressive agent in the conditioning regimen or for treatment of acute graft-vs.-host disease Peripheral blood stem cell Techniques for collecting hematopoietic cells from the mobilization and collection circulation following administration of granulocytecolony stimulating factor (with or without prior chemotherapy). Apheresis is used to collect blood leukocytes enriched for hematopoietic stem cells that normally reside in the marrow. Disease abbreviations AA, aplastic anemia; ALL, acute lymphocytic leukemia; AML, acute myeloid leukemia; BRCA, breast cancer; CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia (often subclassified as CP, chronic phase, or AP, accelerated phase, or BC, blast crisis); HD, Hodgkin’s disease; MDS, myelodysplastic syndrome; McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 11 MM, multiple myeloma; NHL, non-Hodgkin’s lymphoma; RA, refractory anemia; RAEB, refractory anemia with excess blasts; RCMD, refractory cytopenia with myelodysplasia REFERRING TO THE SOURCE OF CELLS FOR THE TRANSPLANT Hematopoietic cell transplantation A term that encompasses all souces of cells that restore (HCT, sometimes HSCT) hematological and immunological function. Some centers use the term “hematopoieic stem cell transplantation”. Bone marrow transplantation Transplantion that involves aspiration of bone marrow (BMT) cells, sieving to remove bony particles, then reinfusion into a recipient Peripheral blood stem cell (PBSC) Transplantation using a source of hematopoietic precursor transplantation cells derived from the peripheral circulation Cord blood transplantation Transplantation using a source of hematopoietic precursor cells derived from the umbilical vein of newborn infants; these infants may or may not be related to their intended recipient T cell depletion In allogeneic transplantation, a process whereby T lymphocyte subsets are removed from the infusate of donor hematopoietic cells; the intent is to decrease the likelihood of the recipient developing acute graft-vs.-host disease Allogeneic transplantation From one person to another McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) HLA, human leukocyte antigen page 12 A set of highly polymorphic antigens encoded by genes in the major histocompatibility complex located on the short arm of chromosome 6 HLA-matched, or -mismatched In allogeneic transplantion, the designation of the relationship of the donor’s HLA type to that of the recipient. HLA-matched means that the donor and recipient have identical types for the antigens tested. HLA-mismatched means that the antigens of donor and recipient are discrepant. Unrelated donor A donor who is HLA-matched to the candidate for transplant, usually someone who has volunteered to be HLA typed as part of an international registry of potential donors. Autologous transplantation Reinfusion of one’s own hematopoietic cells (from peripheral blood or marrow) Syngeneic or isogeneic From one identical twin to another transplantation Day zero By convention, the day on which infusion of hematopoietic cells is completed; all subsequent events are numbered with reference to this day, as in “day 1”, meaning the first day after the infusion. OTHER TERMS AND ABBREVIATIONS COMMONLY USED IN THE PERI-TRANSPLANT PERIOD Hematopoietic growth factors G-CSF, granulocyte colony stimulating factor; GM-CSF, McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 13 granulocyte-macrophage colony stimulating factor; SCF, stem cell factor Antimicrobial drugs TMP-SMX, trimethoprim-sulfamethoxazole; AMB, amphotericin B; DHPG or GCV, ganciclovir; ACV, acyclovir; 3-TC, lamivudine Immunosuppressive drugs CSP or CSA, cyclosporine; FK506 or “tac”, tacrolimus; MTX, methotrexate; MMF, mycophenolate mofetil; ATG, antithymocyte globulin Viruses HSV, herpes simplex virus; CMV, cytomegalovirus; RSV, respiratory syncytial virus; HHV-6, human herpes virus 6; VZV, varicella zoster virus; EBV, Epstein-Barr virus Seropositive or CMV seropositive Presence of antibodies to CMV in blood samples from the patient before transplant, or from the donor, indicating prior CMV infection. The risk of CMV infection in the recipient after transplant is low when both patient and donor are seronegative. CMV can be activated from latency and can replicate when either the recipient or the donor has been previously infected. CMV antigen or DNA positive A blood test that detects either a CMV protein antigen or DNA in circulating leukocytes in the recipient, after transplant. A positive result indicates CMV infection, in contrast to CMV disease, where there is organ McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 14 dysfunction caused by CMV. REFERRING TO THE STATE OF HEMATOPOIETIC CELL ENGRAFTMENT POST TRANSPLANT Hematological acronyms ANC, absolute neutrophil count; PLTS, platelets; Hct, hematocrit Failure to engraft No signs of donor hematopoietic cells are seen in either peripheral blood or marrow post transplant Engraftment Appearance of donor hematopoietic cells in the peripheral blood or marrow post transplant, usually with concordant appearance of donor-derived leukocyte, red blood cell, and platelet lineages. By convention, engraftment is defined as ANC > 500/mm3, platelets > 20,000/mm3, or platelets >50,000/mm3. Graft rejection Disappearance of donor hematopoietic cells after signs of engraftment Mixed chimerism A result of allogeneic transplantation in which both donor and host hematopoietic cells co-exist in the recipient Complete chimerism A result of allogeneic transplantation in which all hematopoietic and lymphoid cells are of donor origin Platelet transfusion dependent A state where platelet transfusions are needed to maintain a patient’s platelet counts above an arbitrary level, usually 10,000/mm3 REFERRING TO GRAFT - VERSUS - HOST DISEASE GVHD An immunological process whereby donor-derived T McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 15 lymphocytes cause damage in recipient tissues; there are two forms of GVHD, acute and chronic Acute GVHD Immune-mediated damage to skin, gastrointestinal mucosa, and liver that occurs from the time of transplant to day 200. Occurs in 40 – 60% of allografts, in 10-15% of autograftsa, and rarely after syngeneic transplantb. Chronic GVHD A pleomorphic syndrome that affects the lacrimal glands, salivary glands, squamous mucosa (skin, mouth, esophagus, and vagina), lungs, muscle and tendons, and immune system. Often overlaps with protracted acute GVHD involving the gut and liver. Hyperacute GVHD Acute GVHD that occurs earlier than expected, usually before day 10, often with capillary leak syndrome and rapidly progressive skin rash, high-volume diarrhea, and jaundice. GVHD prophylaxis Immune suppressive drugs given during the peritransplant period and extended to day 70-80 to prevent or ameliorate the intensity of acute GVHD. Commonly used drugs include methotrexate, cyclosporine, tacrolimus, mycophenolate mofetil, high-dose cyclophosphamide, in different combinations. Stage and grade of GHVD Categoric variables for assessing the extent of damage to skin, gut, and liver (stage) and the overall severity of McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 16 acute GVHD (I-IV in the Americas, A-D in Europe). Not evidence-based but generally descriptive of severity. Acute GVHD Activity Index An evidence-based tool for predicting non-relapse mortality in patients with acute GVHD, based on four variables (total serum bilirubin, anorexia, need for immune suppression, and performance). Primary treatment of GVHD Immunosuppressive medication given to patients in whom a diagnosis of acute GVHD is first made; to be distinguished from prophylactic treatment and secondary treatment of GVHD; usually involves addition of prednisone at a dose of 1 - 2 mg/kg/day to the prophylaxis regimen Secondary treatment of GVHD Medication that is given to patients whose acute GVHD has not responded to primary treatment regimens; usually involves additional immunosuppressive drugs such as MMF, anti-T cell antibodies, anti-cytokine biological therapies, or prednisone pulses of >2 mg/kg/day, in various combinations. REFERRING TO THE OUTCOME OF HEMATOPIETIC CELL TRANSPLANTATION Relapse Reappearance of the malignancy for which the transplant was carried out. Cytogenetic relapse Abnormal cytogenetics or genetic test without detectable abnormal cell morphology McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) Donor lymphocyte infusion (DLI) page 17 Donor cells, given after relapse of malignancy in order to produce a graft-vs.-tumor effect Non-relapse mortality Death in a patient whose underlying malignancy had not relapsed. Second transplant Refers to a second conditioning regimen, followed by a second infusion of hematopoietic cells, usually for persistence or recurrence of malignancy. In allogeneic second transplants, a different donor is often chosen in an attempt to produce better graft-vs.-tumor effect. Tandem transplant A planned treatment, usually for myeloma, where an autologous transplant with myeloablative conditioning is followed by allogeneic transplant with reduced-intensity conditioning. a Holmberg L, Kikuchi K, Gooley T, Adams KM, Hockenbery DM, Flowers MED, Schoch HG, et al. Gastrointestinal graft-versus-host disease in recipients of autologous hematopoietic stem cells: Incidence, risk factors, and outcome. Biology of Blood and Marrow Transplantation 2006; 12: 226 – 234. b Adams KM, Holmberg LA, Leisenring W, Guthrie KA, Tylee TS, McDonald GB, Bensinger WI, et al. Risk factors for syngeneic graft-versus-host disease after adult hematopoietic stem cell transplantation. Blood 2004; 104: 1894 – 1897. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) SUPPORTING APPENDIX 3. ABBREVIATIONS COMMONLY USED HEMATOPOIETIC CELL TRANSPLANTATION. ABBREVIATION MEANING AA Aplastic Anemia aGVHD Acute Graft-vs.-host disease ALL Acute Lymphocytic Leukemia AML Acute Myelogenous Leukemia ANC Absolute Neutrophil Count ANL Acute Non-lymphocytic Leukemia ATG AntiThymocyte Globulin BMT Bone Marrow Transplant BU BUsulfan BU/CY or CY/BU BUsulfan and CYclophosphamide cGVHD chronic GVHD cGy centigray (0.01 Gy), or ~ 1 rad CLL Chronic Lymphocytic Leukemia CML Chronic Myeloid Leukemia CMV cytomegalovirus CSP or CSA cyclosporine CY CYclophosphamide CY/TBI or TBI/CY CYclophosphamide and Total Body Irradiation DLI Donor Lymphocyte Infusion IN THE page 18 FIELD OF McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 19 EBV Epstein-Barr Virus FLU Fludarabine G-CSF Granulocyte colony stimulating factor GM-CSF Granulocyte-macrophage colony stimulating factor GVHD Graft-Versus-Host Disease (see aGVHD and Cgvhd) GVHDAI Graft-Versus-Host Disease Activity Index GVL Graft Versus Leukemia Gy Grey, a radiation dose HCT Hematopoietic Cell Transplant HD Hodgkin’s Disease HHV-6 or -8 Human Herpes Virus-6 or -8 HLA Human Leukocyte-Associated (antigens) HLA-MM HLA-mismatched HSCT hematopoietic stem cell transplant HSV Herpes Simplex Virus MDS Myelodysplastic Syndrome MEL melphalan MM Multiple Myeloma MMF Mycophenolate Mofetil MTX Methotrexate MURD (HLA) Matched UnRelated Donor NHL Non-Hodgkin’s Lymphoma NRM Non-Relapse Mortality, death in the absence of a relapse of malignancy McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) PLTS Platelet count PBSCT Peripheral Blood Stem Cell Transplant RA Refractory Anemia RAEB Refractory Anemia with Excess Blasts RRT Regimen-Related Toxicity SCF Stem Cell Factor SOS Sinusoidal Obstruction Syndrome (aka VOD) TBI Total Body Irradiation TT ThioTEPA TLI Total Lymphoid Irradiation TMI Total Marrow Irradiation TMP-SMX Trimethoprim-sulfamethoxazole URD Unrelated donor of hematopoietic cells VOD Veno-Occlusive Disease, now known as Sinusoidal Obstruction Syndrome VP-16 Etoposide VZV Varicella Zoster Virus WHVPG Wedged Hepatic Venous Pressure Gradient page 20 McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 21 SUPPORTING APPENDIX 4. SUPPLEMENTARY TOPIC-ORIENTED READING LIST. EVALUATION OF LIVER PROBLEMS BEFORE TRANSPLANT FUNGAL LIVER INFECTIONS Anttila VJ, Lamminen AE, Bondestam S, Korhola O, Farkkila M, Sivonen A, Ruutu T, et al. Magnetic resonance imaging is superior to computed tomography and ultrasonography in imaging infectious liver foci in acute leukaemia. Eur J Haematol 1996;56:82-87. Ostrosky-Zeichner L, Alexander BD, Kett DH, Vazquez J, Pappas PG, Saeki F, Ketchum PA, et al. Multicenter clinical evaluation of the (1-->3) beta-D-glucan assay as an aid to diagnosis of fungal infections in humans. Clinical Infectious Diseases 2005;41:654-659. Mennink-Kersten MASH, Donnelly JP, Verweij PE. Detection of circulating galactomannan for the diagnosis and management of invasive aspergillosis. The Lancet Infectious Diseases 2004;4:349-357. Rossetti F, Brawner DL, Bowden RA, Meyer WG, Schoch HG, Fisher L, Myerson D, et al. Fungal liver infection in marrow transplant patients: prevalence at autopsy, predisposing factors, and clinical features. Clinical Infectious Diseases 1995;20:801-811. van Burik JH, Leisenring W, Myerson D, Hackman RC, Shulman HM, Sale GE, Bowden RA, et al. The effect of prophylactic fluconazole on the clinical spectrum of fungal diseases in bone McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 22 marrow transplant recipients with special attention to hepatic candidiasis: An autopsy study of 355 patients. Medicine (Baltimore) 1998;77:246-254. VIRAL HEPATITIS Hui C-k, Lie A, Au W-y, Ma S-y, Leung Y-H, Zhang H-y, Sun J, et al. Effectiveness of prophylactic anti-HBV therapy in allogeneic hematopoietic stem cell transplantation with HBsAg positive donors. American Journal of Transplantation 2005;5:1437-1445. Piekarska A, Zaucha JM, Hellman A, McDonald GB. Prevention of hepatitis B virus (HBV) transmission from an infected stem cell donor. Bone Marrow Transplantation 2007;40:399-400. Vance EA, Soiffer RJ, McDonald GB, Myerson D, Fingeroth J, Ritz J. Prevention of transmission of hepatitis C virus in bone marrow transplantation by treating the donor with alpha-interferon. Transplantation 1996;62:1358-1360. Ramos CA, Saliba RM, de Padua L, Khorshid O, Shpall EJ, Giralt S, Patah PA, et al. Impact of hepatitis C virus seropositivity on survival after allogeneic hematopoietic stem cell transplantation for hematologic malignancies. Haematologica 2009;94:249-257. LIVER DISEASES AT BASELINE Shulman HM, McDonald GB: Hepatic complications of hematopoietic cell transplantation. In: Gershwin ME, Vierling JM, Manns M, eds. Liver Immunology: Principles and Practice. Totowa, NJ: Humana Press, 2007; 409-421. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 23 Ohyashiki K, Kuriyama Y, Nakajima A, Tauchi T, Ito Y, Miyazawa H, Kimura Y, et al. Imatinib mesylate-induced hepato-toxicity in chronic myeloid leukemia demonstrated focal necrosis resembling acute viral hepatitis. Leukemia 2002;16:2160-2161. Ayoub WS, Geller SA, Tran T, Martin P, Vierling JM, Poordad FF. Imatinib (Gleevec)-induced hepatotoxicity. Journal of Clinical Gastroenterology 2005;39:75-77. Wadleigh M, Richardson PG, Zahrieh D, Lee SJ, Cutler C, Ho V, Alyea EP, et al. Prior gemtuzumab ozogamicin exposure significantly increases the risk of veno-occlusive disease in patients who undergo myeloablative allogeneic stem cell transplantation. Blood. 2003;102:15781582. GALLSTONES Safford SD, Safford KM, Martin P, Rice H, Kurtzberg J, Skinner MA. Management of cholelithiasis in pediatric patients who undergo bone marrow transplantation. Journal of Pediatric Surgery 2001;36:86-90. IRON OVERLOAD St Pierre TG, Clark PR, Chua-anusorn W, Fleming AJ, Jeffrey GP, Olynyk JK, Pootrakul P, et al. Noninvasive measurement and imaging of liver iron concentrations using proton magnetic resonance. Blood 2005;105:855-861. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 24 Kontoyiannis DP, Chamilos G, Lewis RE, Giralt S, Cortes J, Raad II, Manning JT, et al. Increased bone marrow iron stores is an independent risk factor for invasive aspergillosis in patients with high-risk hematologic malignancies and recipients of allogeneic hematopoietic stem cell transplantation. Cancer 2007;110:1303-1306. Lucarelli G, Galimberti M, Polchi P, Angelucci E, Baronciani D, Giardini C, Andreani M, et al. Marrow transplantation in patients with thalassemia responsive to iron chelation therapy. New England Journal of Medicine 1993;329:840-844. Foerder CA, Tobin AA, McDonald GB, Zager RA. Bleomycin-detectable iron in plasma of bone-marrow transplant patients: its correlation with liver injury. Transplantation 1992;54:11201123. Tomas JF, Pinilla I, Garcia-Buey ML, Garcia A, Gomez-Garcia de Soria V, R. M, FernandezRanada JM. Long-term liver dysfunction after allogeneic bone marrow transplantation: Clinical features and course in 61 patients. Bone Marrow Transplantation 2000;26:649-655. HEPATOBILIARY PROBLEMS FROM TRANSPLANT THROUGH DAY 200 SINUSOIDAL OBSTRUCTION SYNDROME McDonald GB, Hinds MS, Fisher LB, Schoch HG, Wolford JL, Banaji M, Hardin BJ, et al. Venocclusive disease of the liver and multiorgan failure after bone marrow transplantation: A cohort study of 355 patients. Annals of Internal Medicine 1993;118:255-267. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 25 DeLeve LD, Valla DC, Garcia-Tsao G, American Association for the Study Liver Disease. Vascular disorders of the liver. Hepatology 2009;49:1729-1764. McDonald GB, McCune JS, Batchelder A, Cole S, Phillips B, Ren AG, Vicini P, et al. Metabolism-based cyclophosphamide dosing for hematopoietic cell transplant. Clinical Pharmacology & Therapeutics 2005;78:298-308. Marr KA, Leisenring W, Crippa F, Slattery JT, Corey L, Boeckh M, McDonald GB. Cyclophosphamide metabolism is affected by azole antifungals. Blood 2004;103:1557-1559. Hagglund H, Remberger M, Klaesson S, Lonnqvist B, Ljungman P, Ringden O. Norethisterone treatment, a major risk-factor for veno-occlusive disease in the liver after allogeneic bone marrow transplantation. Blood 1998;92:4568-4572. Cutler C, Stevenson K, Haesook TK, Richardson PG, Vincent TH, Linden E, Revta C, et al. Sirolimus is associated with veno-occlusive disease of the liver after myeloblative allogeneic stem cell transplantation. Blood 2008;112:4425-4431. Corbacioglu S, Honig M, Lahr G, Stohr S, Berry G, Friedrich W, Schulz AS. Stem cell transplantation in children with infantile osteopetrosis is associated with a high incidence of VOD, which could be prevented with defibrotide. Bone Marrow Transplantation 2006;38:547553. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 26 Cheuk DK, Wang P, Lee TL, Chiang AK, Ha SY, Lau YL, Chan GC. Risk factors and mortality predictors of hepatic veno-occlusive disease after pediatric hematopoietic stem cell transplantation. Bone Marrow Transplantation 2007;40:935-944. Tay J, Tinmouth A, Fergusson D, Huebsch L, Allan DS. Systematic review of controlled clinical trials on the use of ursodeoxycholic acid for the prevention of hepatic veno-occlusive disease in hematopoietic stem cell transplantation. Biology of Blood & Marrow Transplantation 2007;13:206-217. Hasegawa S, Horibe K, Kawabe T, Kato K, Kojima S, Matsuyama T, Hirabayashi N. Venoocclusive disease of the liver after allogeneic bone marrow transplantation in children with hematologic malignancies: incidence, onset time and risk factors. Bone Marrow Transplantation 1998;22:1191-1197. Lee JL, Gooley T, Bensinger W, Schiffman K, McDonald GB. Venocclusive disease of the liver after busulfan, melphalan, and thioTEPA conditioning therapy: Incidence, risk factors, and outcome. Biology of Blood & Marrow Transplantation 1999;5:306-315. Toh HC, McAfee SL, Sackstein R, Cox BF, Colby C, Spitzer TR. Late onset veno-occlusive disease following high-dose chemotherapy and stem cell transplantation. Bone Marrow Transplantation 1999;24:891-895. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 27 Rajvanshi P, Shulman HM, Sievers EL, McDonald GB. Hepatic sinusoidal obstruction following Gemtuzumab ozogamicin (Mylotarg) therapy. Blood 2002;99:4245-4246. Pihusch M, Wegner H, Goehring P, Salat C, Pihusch V, Hiller E, Andreesen R, et al. Diagnosis of hepatic veno-occlusive disease by plasminogen activator inhibitor-1 plasma antigen levels: a prospective analysis in 350 allogeneic hematopoietic stem cell recipients. Transplantation 2005;80:1376-1382. Lassau N, Auperin A, Leclere J, Bennaceur A, Valteau-Couanet D, Hartmann O. Prognostic value of doppler-ultrasonography in hepatic veno-occlusive disease. Transplantation. 2002;74:60-66. Erturk SM, Mortele KJ, Binkert CA, Glickman JN, Oliva M-R, Ros PR, Silverman SG. CT features of hepatic venoocclusive disease and hepatic graft-versus-host disease in patients after hematopoietic stem cell transplantation. American Journal of Roentgenology 2006;186:14971501. Hashiguchi M, Okamura T, Yoshimoto K, Ono N, Imamura R, Yakushiji K, Ogata H, et al. Demonstration of reversed flow in segmental branches of the portal vein with hand-held color Doppler ultrasonography after hematopoietic stem cell transplantation. Bone Marrow Transplantation 2005;36:1071-1075. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 28 McCarville MB, Hoffer FA, Howard SC, Goloubeva O, Kauffman WM. Hepatic veno-occlusive disease in children undergoing bone-marrow transplantation: usefulness of sonographic findings. Pediatric Radiology 2001;31:102-105. Choi SW, Islam S, Greenson JK, Levine J, Hutchinson R, Yanik G, Teitelbaum DH, et al. The use of laparoscopic liver biopsies in pediatric patients with hepatic dysfunction following allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplantation 2005;36:891896. Groszmann RJ, Wongcharatrawee S. The hepatic venous pressure gradient: anything worth doing should be done right. Hepatology. 2004;39:280-282. Rubenfeld GD, Crawford SW. Withdrawing life support from mechanically ventilated recipients of bone marrow transplants: a case for evidence-based guidelines. Ann Intern Med 1996;125:625-633. Salinger DH, McCune JS, Ren AG, Shen DD, Slattery JT, Phillips B, McDonald GB, et al. Realtime dose adjustment of cyclophosphamide in a preparative regimen for hematopoietic cell transplant: a Bayesian pharmacokinetic approach. Clinical Cancer Research 2006;12:4888-4898. Slattery JT, Clift RA, Buckner CD, Radich J, Storer B, Bensinger WI, Soll E, et al. Marrow transplantation for chronic myeloid leukemia - the influence of plasma busulfan levels on the outcome of transplantation. Blood 1997;89:3055-3060. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 29 Shaw PJ, Scharping CE, Brian RJ, Earl JW. Busulfan pharmacokinetics using a single daily high-dose regimen in children with acute leukemia. Blood 1994;84:2357-2362. Ringden O, Ruutu T, Remberger M, Nikoskelainen J, Volin L, Vindelov L, Parkkali T, et al. A randomized trial comparing busulfan with total body irradiation as conditioning in allogeneic marrow transplant recipients with leukemia: a report from the Nordic Bone Marrow Transplantation Group. Blood 1994;83:2723-2730. Shulman HM, Gown AM, Nugent DJ. Hepatic veno-occlusive disease after bone marrow transplantation. Immunohistochemical identification of the material within occluded central venules. Am J Pathol 1987;127:549-558. Kikuchi K, Rudolph R, Murakami C, Kowdley KV, McDonald GB. Portal vein thrombosis after hematopoietic cell transplantation: frequency, treatment, and outcome. Bone Marrow Transplantation 2002;29:329-333. Pihusch M, Wegner H, Goehring P, Salat C, Pihusch V, Andreesen R, Kolb HJ, et al. Protein C and procollagen III peptide levels in patients with hepatic dysfunction after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplantation 2005;36:631-637. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 30 Kallianpur AR, Hall LD, Yadav M, Byrne DW, Speroff T, Dittus RS, Haines JL, et al. The hemochromatosis C282Y allele: a risk factor for hepatic veno-occlusive disease after hematopoietic stem cell transplantation. Bone Marrow Transplantation 2005;35:1155-1164. Kallianpur AR. Genomic screening and complications of hematopoietic stem cell transplantation: has the time come? Bone Marrow Transplantation 2005;35:1-16. Srivastava A, Poonkuzhali B, Shaji RV, George B, Mathews V, Chandy M, Krishnamoorthy R. Glutathione S-transferase M1 polymorphism: a risk factor for hepatic venoocclusive disease in bone marrow transplantation. Blood 2004;104:1574-1577. Bornhauser M, Storer B, Slattery J, Appelbaum F, Deeg H, Hansen J, Martin P, et al. Conditioning with fludarabine and targeted busulfan for transplantation of allogeneic hematopoietic stem cells. Blood 2003;102:820-826. Anderson JE, Appelbaum FR, Schoch G, Barnett T, Chauncey TR, Flowers ME, Storb R. Relapse after allogeneic bone marrow transplantation for refractory anemia is increased by shielding lungs and liver during total body irradiation. Biology of Blood & Marrow Transplantation 2001;7:163-170. Meresse V, Hartmann O, Vassal G, Benhamou E, Vatteau-Couenet D, Brugieres L, Lemerle J. Risk factors of hepatic venocclusive disease after high-dose busulfan-containing regimens McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 31 followed by autologous bone marrow transplantation: a study in 136 children. Bone Marrow Transplant 1992;10:135-141. Hassan M, Ljungman P, Ringden O, Hassan Z, Oberg G, Nilsson C, Bekassy A, et al. The effect of busulphan on the pharmacokinetics of cyclophosphamide and its 4-hydroxy metabolite: time interval influence on therapeutic efficacy and therapy-related toxicity. Bone Marrow Transplantation. 2000;25:915-924. Wang X, Kanel GC, DeLeve LD. Support of sinusoidal endothelial cell glutathione prevents hepatic veno-occlusive disease in the rat. Hepatology 2000;31:428-434. Geraci JP, Mariano MS, Jackson KL. Radiation hepatopathy of the rat: microvascular fibrosis and enhancement of liver dysfunction by diet and drugs. Radiat Res 1992;129:322-332. Lee J-H, Choi S-J, Lee J-H, Kim S-E, Park C-J, Chi H-S, Lee M-S, et al. Decreased incidence of hepatic veno-occlusive disease and fewer hemostatic derangements associated with intravenous busulfan vs oral busulfan in adults conditioned with busulfan + cyclophosphamide for allogeneic bone marrow transplantation. Annals of Hematology 2005;84:321-330. Radich JP, Gooley T, Bensinger W, Chauncey T, Clift R, Flowers M, Martin P, et al. HLAmatched related hematopoietic cell transplantation for chronic-phase CML using a targeted busulfan and cyclophosphamide preparative regimen. Blood 2003;102:31-35. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 32 Deeg HJ, Storer BE, Boeckh M, Martin PJ, McCune JS, Myerson D, Heimfeld S, et al. Reduced incidence of acute and chronic graft-versus-host disease with the addition of thymoglobulin to a targeted busulfan/cyclophosphamide regimen. Biology of Blood & Marrow Transplantation 2006;12:573-584. Kashyap A, Wingard J, Cagnoni P, Roy J, Tarantolo S, Hu W, Blume K, et al. Intravenous versus oral busulfan as part of a busulfan/cyclophosphamide preparative regimen for allogeneic hematopoietic stem cell transplantation: decreased incidence of hepatic venoocclusive disease (HVOD), HVOD-related mortality, and overall 100-day mortality. Biology of Blood & Marrow Transplantation 2002;8:493-500. Williams CB, Day SD, Reed MD, Copelan EA, Bechtel T, Leather HL, Wingard JR, et al. Dose modification protocol using intravenous busulfan (Busulfex) and cyclophosphamide followed by autologous or allogeneic peripheral blood stem cell transplantation in patients with hematologic malignancies. Biology of Blood & Marrow Transplantation 2004;10:614-623. Deleve LD, Wang X, Tsai J, Kanel G, Strasberg S, Tokes ZA. Sinusoidal obstruction syndrome (veno-occlusive disease) in the rat is prevented by matrix metalloproteinase inhibition. Gastroenterology. 2003;125:882-890. Chalandon Y, Roosnek E, Mermillod B, Newton A, Ozsahin H, Wacker P, Helg C, et al. Prevention of veno-occlusive disease with defibrotide after allogeneic stem cell transplantation. Biology of Blood & Marrow Transplantation 2004;10:347-354. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 33 Versluys B, Bhattacharaya R, Steward C, Cornish J, Oakhill A, Goulden N. Prophylaxis with defibrotide prevents veno-occlusive disease in stem cell transplantation after gemtuzumab ozogamicin exposure. Blood. 2004;103:1968. Imran H, Tleyjeh IM, Zirakzadeh A, Rodriguez V, Khan SP. Use of prophylactic anticoagulation and the risk of hepatic veno-occlusive disease in patients undergoing hematopoietic stem cell transplantation: a systematic review and meta-analysis. Bone Marrow Transplantation 2006;37:677-686. Bearman SI, Hinds MS, Wolford JL, Petersen FB, Nugent DL, Slichter SJ, Shulman HM, et al. A pilot study of continuous infusion heparin for the prevention of hepatic venocclusive disease after bone marrow transplantation. Bone Marrow Transplant 1990;5:407-411. Budinger MD, Bouvier M, Shah A, McDonald GB. Results of a phase I trial of antithrombin III as prophylaxis in bone marrow transplant patients at risk for venocclusive disease. Blood 1996;88:172a. Corbacioglu S, Greil J, Peters C, Wulffraat N, Laws HJ, Dilloo D, Straham B, et al. Defibrotide in the treatment of children with veno-occlusive disease (VOD): a retrospective multicentre study demonstrates therapeutic efficacy upon early intervention. Bone Marrow Transplantation 2004;33:189-195. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 34 Kornblum N, Ayyanar K, Benimetskaya L, Richardson P, Iacobelli M, Stein CA. Defibrotide, a polydisperse mixture of single-stranded phosphodiester oligonucleotides with lifesaving activity in severe hepatic veno-occlusive disease: clinical outcomes and potential mechanisms of action. Oligonucleotides 2006;16:105-114. Benimetskaya L, Wu S, Voskresenskiy AM, Echart C, Zhou JF, Shin J, Iacobelli M, et al. Angiogenesis alteration by defibrotide: implications for its mechanism of action in severe hepatic veno-occlusive disease. Blood 2008;112:4343-4352. Lazarus HM, McCrae KR. SOS! Defibrotide to the rescue. Blood 2008;112:3924-3925. Azoulay D, Castaing D, Lemoine A, Hargreaves GM, Bismuth H. Transjugular intrahepatic portosystemic shunts (TIPS) for severe veno-occlusive disease of the liver following bone marrow transplantation. Bone Marrow Transplantation 2000;25:987-992. Meacher R, Venkatesh B, Lipman J. Acute respiratory distress syndrome precipitated by transjugular intrahepatic porto-systemic shunting for severe hepatic veno-occlusive disease. Is it due to pulmonary leucostasis? Intensive Care Medicine 1999;25:1332-1333. Koenecke C, Kleine M, Schrem H, Krug U, Nashan B, Neipp M, Ganser A, et al. Sinusoidal obstruction syndrome of the liver after hematopoietic stem cell transplantation: decision making for orthotopic liver transplantation. International Journal of Hematology 2006;83:271-274. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 35 Mellgren K, Fasth A, Saalman R, Olausson M, Abrahamsson J. Liver transplantation after stem cell transplantation with the same living donor in a monozygotic twin with acute myeloid leukemia. Annals of Hematology 2005;84:755-757. Kim ID, Egawa H, Marui Y, Kaihara S, Haga H, Lin YW, Kudoh K, et al. A successful liver transplantation for refractory hepatic veno-occlusive disease originating from cord blood transplantation. American Journal of Transplantation 2002;2:796-800. CHOLESTATIC LIVER DISORDERS Malone FR, Leisenring W, Schoch G, Stern J, Aker S, Lawler R, McDonald GB. Prolonged anorexia and elevated plasma cytokine levels following myeloablative allogeneic hematopoietic cell transplant. Bone Marrow Transplant 2007;40:765-772. Green RM, Beier D, Gollan JL. Regulation of hepatocyte bile salt transporters by endotoxin and inflammatory cytokines in rodents. Gastroenterology 1996;111:193-198. Chand N, Sanyal AJ. Sepsis-induced cholestasis. Hepatology 2007;45:230-241. Bernuau D, Feldmann G, Degott C, Gisselbrecht C. Ultrastructural lesions of bile ducts in primary biliary cirrhosis. A comparison with the lesions observed in graft versus host disease. Human Pathology 1981;12:782-793. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 36 Quaranta S, Shulman HM, Paganin S, Schoenfeld Y, Peter J, Ahmed A, Leung PA, et al. Autoantibodies in human chronic graft-versus-host disease after hematopoietic cell transplantation. Clinical Immunology 1999;91:106-116. Saunders MD, Shulman HM, Murakami CS, Chauncey TR, Bensinger WI, McDonald GB. Bile duct apoptosis and cholestasis resembling acute graft-versus-host disease after autologous hematopoietic cell transplantation. American Journal of Surgical Pathology 2000;24:1004-1008. Akpek G, Boitnott JK, Lee LA, Hallick JP, Torbenson M, Jacobsohn DA, Arai S, et al. Hepatitic variant of graft-versus-host disease after donor lymphocyte infusion. Blood 2002;100:39033907. Ma SY, Au WY, Ng IOL, Lie AKW, Leung AYH, Liang R, Lau GKK, et al. Hepatitic graftversus-host disease after hematopoietic stem cell transplantation: clinicopathologic features and prognostic implication. Transplantation 2004;77:1252-1259. Melin-Aldana H, Thormann K, Duerst R, Kletzel M, Jacobsohn DA. Hepatitic pattern of graft versus host disease in children. Pediatric Blood & Cancer 2007;49:727-730. Stockschlaeder M, Storb R, Pepe M, Longton G, McDonald GB, Anasetti C, Appelbaum FR, et al. A pilot study of low dose cyclosporin for graft-versus-host prophylaxis in marrow transplantation. Br J Haematol 1992;80:49-54. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 37 List AF, Spier C, Greer J, Wolff S, Hutter J, Dorr R, Salmon S, et al. Phase I/II trial of cyclosporine as a chemotherapy-resistance modifier in acute leukemia J Clin Oncol 1993;11:1652-1660. ACUTE HEPATOCELLULAR INJURY Kim B, Chung K, Sun H, Suh J, Min W, Kang C, Sim S, et al. Liver disease during the first posttransplant year in bone marrow transplantation recipients: retrospective study. Bone Marrow Transplantation 2000;26:193-197. Ho G-T, Parker A, MacKenzie JF, Morris AJ, Stanley AJ. Abnormal liver function tests following bone marrow transplantation: aetiology and role of liver biopsy. European Journal of Gastroenterology & Hepatology 2004;16:157-162. Poon A, Ly L. Common potential drug interactions following hematopoietic cell transplantation. In: Appelbaum FR, Forman SJ, Negrin RS, Blume KG. Thomas' Hematopoietic Cell Transplantation. 4th ed. Oxford, UK: Wiley-Blackwell Publishing, 2009; 1523-1538. Koc Y, Miller KB, Schenkein DP, Griffith J, Akhtar M, DesJardin J, Snydman DR. Varicella zoster virus infections following allogeneic bone marrow transplantation: frequency, risk factors, and clinical outcome. Biology of Blood & Marrow Transplantation 2000;6:44-49. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 38 Bordigoni P, Carret AS, Venard V, Witz F, Le Faou A. Treatment of adenovirus infections in patients undergoing allogeneic hematopoietic stem cell transplantation. Clinical Infectious Diseases 2001;32:1290-1297. Baldwin A, Kingman H, Darville M, Foot AB, Grier D, Cornish JM, Goulden N, et al. Outcome and clinical course of 100 patients with adenovirus infection following bone marrow transplantation. Bone Marrow Transplantation 2000;26:1333-1338. Bruno B, Gooley T, Hackman RC, Davis C, Corey L, Boeckh M. Adenovirus infection in hematopoietic stem cell transplantation: effect of ganciclovir and impact on survival. Biology of Blood & Marrow Transplantation 2003;9:341-352. Walls T, Shankar AG, Shingadia D. Adenovirus: an increasingly important pathogen in paediatric bone marrow transplant patients. The Lancet Infectious Diseases 2003;3:79-86. Kuribayashi K, Matsunaga T, Iyama S, Takada K, Sato T, Murase K, Fujimi A, et al. Human herpesvirus-6 hepatitis associated with cyclosporine-A encephalitis after bone marrow transplantation for chronic myeloid leukemia. Internal Medicine 2006;45:475-478. Muller WJ, Levin MJ, Shin YK, Robinson C, Quinones R, Malcolm J, Hild E, et al. Clinical and in vitro evaluation of cidofovir for treatment of adenovirus infection in pediatric hematopoietic stem cell transplant recipients. Clinical Infectious Diseases 2005;41:1812-1816. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 39 Lau GK, He M-L, Fong DYT, Bartholomeusz A, Au W, Lie AKW, Locarnini S, et al. Preemptive use of lamivudine reduces hepatitis B exacerbation after allogeneic hematopoietic cell transplantation. Hepatology 2002;36:702-709. Hui CK, Cheung WWW, Au WY, Lie AKW, Zhang HY, Yueng YH, Wong BCY, et al. Hepatitis B reactivation after withdrawal of pre-emptive lamivudine in patients with haematological malignancy on completion of cytotoxic chemotherapy. Gut 2005;54:1597-1603. Lin P-C, Poh S-B, Lee M-Y, Hsiao L-T, Chen P-M, Chiou T-J. Fatal fulminant hepatitis B after withdrawal of prophylactic lamivudine in hematopoietic stem cell transplantation patients. International Journal of Hematology 2005;81:349-351. de Latour RP, Asselah T, Levy V, Scieux C, Devergie A, Ribaud P, Esperou H, et al. Treatment of chronic hepatitis C virus in allogeneic bone marrow transplant recipients. Bone Marrow Transplantation 2005;36:709-713. Honjo I, Suou T, Hirayama C. Hepatotoxicity of cyclophosphamide in man: Pharmacokinetic analysis. Res Commun Chem Pathol Pharmacol 1988;61:149-165. Fischer MA, Winkelmayer WC, Rubin RH, Avorn J. The hepatotoxicity of antifungal medications in bone marrow transplant recipients. Clinical Infectious Diseases 2005;41:301-307. FUNGAL INFECTIONS McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 40 Ullmann AJ, Lipton JH, Vesole DH, Chandrasekar P, Langston A, Tarantolo SR, Greinix H, et al. Posaconazole or fluconazole for prophylaxis in severe graft-versus-host disease. New England Journal of Medicine 2007;356:335-347. van Burik J-AH. Role of new antifungal agents in prophylaxis of mycoses in high risk patients. Current Opinion in Infectious Diseases 2005;18:479-483. GALLBLADDER AND BILIARY DISEASE Ko CW, Murakami C, Sekijima JH, Kim MH, McDonald GB, Lee SP. Chemical composition of gallbladder sludge in patients after marrow transplantation. Am J Gastroenterol 1996;91:12071210. Ko CW, Gooley T, Schoch HG, Myerson D, Hackman RC, Shulman HM, Sale GE, et al. Acute pancreatitis in marrow transplant patients: prevalence at autopsy and risk factor analysis. Bone Marrow Transplant 1997;20:1081-1086. Murakami CS, Louie W, Chan GS, O'Donnell M, David D, Forman SJ, McDonald GB. Biliary obstruction in hematopoietic cell transplant recipients: an uncommon diagnosis with specific causes. Bone Marrow Transplantation 1999;23:921-927. MALIGNANT DISORDERS Zutter MM, Martin PJ, Sale GE, Shulman HM, Fisher L, Thomas ED, Durnam DM. Epstein-barr virus lymphoproliferation after bone marrow transplantation. Blood 1988;72:520-529. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 41 HEPATOBILIARY PROBLEMS IN LONG-TERM TRANSPLANT SURVIVORS CHRONIC GVHD Sakai M, McDonald GB: Gastrointestinal and hepatic manifestations of chronic GVHD. In: Vogelsang GB, Pavletic SZ, eds. Chronic graft-versus-host disease: Interdisciplinary management. First ed. New York, New York: Cambridge University Press, 2009; 216-226. Jagasia M, Shulman HM, Filipovich AH, Pavletic S: Diagnosis and Staging. In: Vogelsang GB, Pavletic SZ, eds. Chronic graft-versus-host disease: Interdisciplinary management. First ed. New York, New York: Cambridge University Press, 2009; 87-100. Malik AH, Collins JRH, Saboorian MH, Lee WM. Chronic graft versus host disease (GVHD) following hematopoietic cell transplantation (HCT) presenting as an acute hepatitis. American Journal of Gastroenterology 2001;96:588-590. Mullighan CG, Bogdanos DP, Vergani D, Bardy PG. Cytochrome P450 1A2 is a target antigen in hepatitic graft-versus-host disease. Bone Marrow Transplantation 2006;38:703-705. Martin PJ, Gilman AL: Front Line Treatment of Chronic Graft Versus Host Disease. In: Vogelsang GB, Pavletic SZ, eds. Chronic graft-versus-host disease: Interdisciplinary management. First ed. New York, New York: Cambridge University Press, 2009; 124-133. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 42 Arat M, Idilman R, Soydan EA, Soykan I, Erden E, Karayalcin S, Akan H. Ursodeoxycholic acid treatment in isolated chronic graft-vs.-host disease of the liver. Clinical Transplantation 2005;19:798-803. Orlando G, Ferrant A, Schots R, Goffette P, Mathijs J, Lemaire J, Danse E, et al. Liver transplantation for chronic graft-versus-host disease: case report with 10-year follow-up. Transplant International 2005;18:125-129. HEPATITIS VIRUSES Nieters A, Kallinowski B, Brennan P, Ott M, Maynadie M, Benavente Y, Foretova L, et al. Hepatitis C and risk of lymphoma: results of the European multicenter case-control study EPILYMPH. Gastroenterology 2006;131:1879-1886. Gisbert JP, Garcia-Buey L, Pajares JM, Moreno-Otero R. Systematic review: regression of lymphoproliferative disorders after treatment for hepatitis C infection. Alimentary Pharmacology & Therapeutics 2005;21:653-662. Lok ASF, McMahon BJ. Chronic hepatitis B: Update 2009. Hepatology 2009;50:661-662. Lalazar G, Rund D, Shouval D. Screening, prevention and treatment of viral hepatitis B reactivation in patients with haematological malignancies. British Journal of Haematology 2007;136:699-712. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 43 Hui C-K, Cheung WWW, Zhang H-Y, Au W-Y, Yueng Y-H, Leung AYH, Leung N, et al. Kinetics and risk of de novo hepatitis B infection in HBsAg-negative patients undergoing cytotoxic chemotherapy. Gastroenterology 2006;131:59-68. Thursky KA, Worth LJ, Seymour JF, Miles Prince H, Slavin MA. Spectrum of infection, risk and recommendations for prophylaxis and screening among patients with lymphoproliferative disorders treated with alemtuzumab. British Journal of Haematology 2006;132:3-12. Angelucci E, Muretto P, Nicolucci A, Baronciani D, Erer B, Gaziev J, Ripalti M, et al. Effects of iron overload and hepatitis C virus positivity in determining progression of liver fibrosis in thalassemia following bone marrow transplantation. Blood 2002;100:17-21. Shuhart MC, Myerson D, Childs B, Fingeroth JD, Perry JJ, Snyder DS, Spurgeon CL, et al. Marrow transplantation from hepatitis C virus seropositive donors: transmission rate and clinical course. Blood 1994;84:3229-3235. Andreoni KA, Lin JI, Groben PA. Liver transplantation 27 years after bone marrow transplantation from the same living donor. New England Journal of Medicine 2004;350:26242625. Rizzo JD, Wingard JR, Tichelli A, Lee SJ, Van Lint MT, Burns LJ, Davies SM, et al. Recommended screening and preventive practices for long-term survivors after hematopoietic cell transplantation: joint recommendations of the European Group for Blood and Marrow McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 44 Transplantation, Center for International Blood and Marrow Transplant Research, and the American Society for Blood and Marrow Transplantation. Bone Marrow Transplantation 2006;37:249-261. IRON OVERLOAD Kamble R, Mims M. Iron-overload in long-term survivors of hematopoietic transplantation. Bone Marrow Transplantation 2006;37:805-806. Angelucci E, Brittenham GM, McLaren CE, Ripalti M, Baronciani D, Giardini C, Galimberti M, et al. Hepatic iron concentration and total body iron stores in thalassemia major. New England Journal of Medicine 2000 343:327-331. Strasser SI, Kowdley KV, Sale GE, McDonald GB. Iron overload in bone marrow transplant recipients. Bone Marrow Transplant 1998;22:167-173. Bair S, Spaulding E, Parkkinen J, Shulman HM, Lesnikov V, Beauchamp M, Canonne-Hergaux F, et al. Transplantation of allogeneic T cells alters iron homeostasis in NOD/SCID mice. Blood 2009;113:1841-1844. Lucarelli G, Angelucci E, Giardini C, Baronciani D, Galimberti M, Polchi P, Bartolucci M, et al. Fate of iron stores in thalassaemia after bone-marrow transplantation. Lancet 1993;342:13881391. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) page 45 Muretto P, Angelucci E, Lucarelli G. Reversibility of cirrhosis in patients cured of thalassemia by bone marrow transplantation. Annals of Internal Medicine 2002;136:667-672. CANCER IN THE LIVER Socie G, Deeg HJ: Secondary Malignancies and Other Late Effects. In: Vogelsang GB, Pavletic SZ, eds. Chronic graft-versus-host disease: Interdisciplinary management. First ed. New York, New York: Cambridge University Press, 2009; 326-334. Bhatia S, Louie AD, Bhatia R, O'Donnell MR, Fung H, Kashyap A, Krishnan A, et al. Solid cancers after bone marrow transplantation. Journal of Clinical Oncology 2001;19:464-471. FUNGAL ABSCESS Thaler M, Pastakia B, Shawker TH, O'Leary T, Pizzo PA. Hepatic candidiasis in cancer patients: the evolving picture of the syndrome. Annals of Internal Medicine 1988;108:88-100. Oliver MR, Van Voorhis WC, Boeckh M, Mattson D, Bowden RA. Hepatic mucormycosis in a bone marrow transplant recipient who ingested naturopathic medicine. Clinical Infectious Diseases 1996;22:521-524. NODULAR REGENERATIVE HYPERPLASIS Snover DC, Weisdorf S, Bloomer J, McGlave P, Weisdorf D. Nodular regenerative hyperplasia of the liver following bone marrow transplantation. Hepatology 1989;9:443-448. McDonald GB: Complications of hematopoietic cell transplant (ON-LINE VERSION) (Revised 2/13/16) GALLBLADDER, page 46 BILIARY DISEASE, AND PANCREATITIS Teefey SA, Hollister MS, Lee SP, Jacobson AF, Higano CS, Bianco JA, Colacurcio CJ. Gallbladder sludge formation after bone marrow transplant: sonographic observations. Abdom Imaging 1994;19:57-60. Sastry J, Young S, Shaw PJ. Acute pancreatitis due to tacrolimus in a case of allogeneic bone marrow transplantation. Bone Marrow Transplantation 2004;33:867-868.