STEMI_Launch_May 12 - Royal Columbian Hospital
advertisement

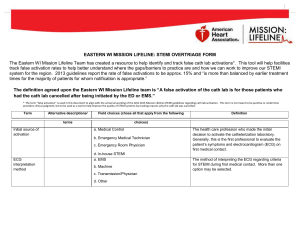
British Columbia Ambulance Service Prehospital STEMI Launch Protocol F.H.A. Lead – Helen Elliott B.C.A.S. Lead – Robert Wand Participants Prehospital - Primary Care Paramedic (PCP) - Advanced Care Paramedic (ACP) Critical Care Flight Paramedics (CCP) Station 280, YVR Vancouver Dispatch Operations Victoria Dispatch – Air Operations Helijet Airways Royal Columbian Hospital (RCH) - Cardiac Catheterization Laboratory (Cath lab) - Emergency Department - Security - Admitting PCP Assists with the ACP crew on scene, as per standard practice - Have no 12 lead Electrocardiogram (ECG) capabilities - Do not interpret 12 lead ECGs ACP Responsible for doing 12 lead ECG Will do 12 lead ECG a.s.a.p. Will go through inclusion/exclusion criteria If STEMI, initiate launch through B.C. Ambulance Vancouver Dispatch Center Send 12 lead to RCH (five alert clients) Will call RCH Emergency Room Physician and notify him/her of 12 lead and STEMI launch British Columbia Ambulance Service Professionalism - Accountability - Responsiveness - Teamwork - Wellness Emergency and Health Services Commission British Columbia Ambulance Service Continue treating patient Will organize transport to Landing Zone (Pt on a #9 stretcher with a mattress) Give brief report to CCP Flight Team Give copy of patient care report and 12 lead ECG to CCP Flight Team If an excluded STEMI or Air transport unavailable the ALS crew sends a copy of 12 lead to Chilliwack General Hospital Emergency Department Crew calls Chilliwack General Hospital Emergency Department and transports patient to Chilliwack General Hospital Emergency Department Will call RCH Emergency Room Physician and notify him/her of cancellation of STEMI launch due to no aircraft or CCP Flight Team Crew is responsible for patient and patient history Vancouver Dispatch Operations Takes request for STEMI launch from crew (usually crew or physician) Sends information to Victoria Dispatch – Air Operations, as per standard protocol Victoria Dispatch – Air Operations Dispatches call, same format as an Auto launch IF 80 Bravo is not available and 80 Alpha and/or 44Alpha are responding, Victoria Dispatch- Air Operations informs Vancouver Dispatch Operations who passes on this information to the crew Helijet Pilots receive call from Victoria Dispatch- Air Operations Accept the call If unable to make Chilliwack, advises Victoria Dispatch- Air Operations where they can go, i.e. Abbotsford Pilots start up machine and wait for CCP Flight Team to arrive. If 44 Alpha is responding, the pilots load the gear into machine and then start the machine(this is same protocol as the Auto Launch) Upon arrival at LZ, the pilot talks to CCP Flight Team regarding shutting down and/or hot loading British Columbia Ambulance Service Professionalism - Accountability - Responsiveness - Teamwork - Wellness British Columbia Ambulance Service Critical Care Flight Paramedics Receives STEMI Launch via pager Code 3 to Helicopter Phone Victoria Dispatch- Air Operations on way to machine for information Air to ground communication with ground ACP Give ETA and set up a landing zone Once landed - Get brief report from ground ACP - Gets all paperwork including a copy of 12 lead Load patient into machine Treat as appropriate Give Plavix (Clopidogrel) 600mg orally. If patient already on Plavix, give 300 mg. Phone RCH (Emergency Department) with ETA Phone Victoria Dispatch- Air Operations with ETA (Victoria Dispatch- Air Operations notifies Vancouver Dispatch Operations) Upon arrival at RCH - During Cath lab hours, 0800H – 1800H Mon – Fri, patient transported directly to Cath lab (patient care report given to cath lab staff) - After hours, patient transported directly to Emergency Department (patient care report given to admitting) RCH Cardiac Catheterization Lab Must have bed available upon arrival Receives patient directly during business hours Can have patient diverted directly to Cath lab after hours, (if patient not in Emergency Department). Must call security, and have security at RCH helipad divert CCP Flight Crew upon landing RCH Emergency Department Receives transmitted 12 lead ECG from ACP crew Receives notification of STEMI from ACP crew British Columbia Ambulance Service Professionalism - Accountability - Responsiveness - Teamwork - Wellness British Columbia Ambulance Service If Emergency Department Physician states it is not a STEMI he/she calls Vancouver Dispatch Operations directly and cancels the STEMI Launch Emergency Department Physician reviews 12 lead ECG and notifies on-call cardiac interventionalist. If on-call cardiac interventionalist states this patient is not a candidate for Cardiac catheterization then he/she notifies Emergency Department Physician and Emergency Department Physician cancels STEMI launch via regional dispatch If STEMI cancelled by ACP crew (no aircraft and/or CCP Flight Team) they will notify RCH Emergency Department Physician and RCH Emergency Department Physician will notify on-call cardiac interventionalist. After hours patient is brought to Emergency Department. The Patient is under the care of Emergency Department Physician Question and/or comments The ACP will run through the inclusion/exclusion criteria for P.C.I. If the patient meets the exclusion criteria then they will cancel the STEMI launch. If the patient is unstable the ACP crew at scene decides whether they should wait for the CCP team or transport directly to Chilliwack General Hospital. If ACP crew transports To CGH, the ACP crew will notify the CGH Emergency room Physician that the CCP team is enroute. Once transport has started to Royal Columbian Hospital in the Helicopter, there is no turning back and/or cancelling. We will continue transport and drop off at the Emergency Department. If the Emergency Room Physician and/or Cardiac Interventionalist want to cancel the STEMI Launch after reading the 12 lead ECG they must contact Vancouver Dispatch Operations. If they do not call that means it is still a go and the call continues. If patient is in cardiac arrest upon arrival at Royal Columbian Hospital during business hours the patient will be transported directly to the Emergency Department. FYI, the CCP Flight Team’s main goal is rapid turnaround time and rapid transport. The CCP Flight Team will get a brief history and any completed paperwork from the ground ACP. The ground ACP crew will be responsible for contacting the E.R. Physician and giving him/her a full report. The CCP Flight Team will report what transpired while the patient was in there care. (The CCP Flight Team will probably not have a full assessment, history and treatment report to give to the receiving staff). If the CCP Flight Team is enroute to a STEMI launch and an Auto launch comes in, the CCP Flight Team will be diverted to the Auto launch and a second team will be launched. (Good communication is the key). British Columbia Ambulance Service Professionalism - Accountability - Responsiveness - Teamwork - Wellness British Columbia Ambulance Service Inclusion/Exclusion criteria for STEMI Launch Inclusion: 1. 12 lead ECG must show ST elevation of 1 mm or greater in two anatomically contiguous leads and the patient must have symptoms of ischemia (chest pain, diaphoresis, shortness of breath, jaw/neck pain, dizziness, nausea). The 12 lead ECG must read *** Meets ST Elevation MI Criteria*** or ***Acute MI Suspected*** 2. STEMI in cardiogenic shock 3. Resuscitated post arrest who has a 12 Lead ECG showing STEMI Exclusion: 1. 12 lead ECG has less than 1 mm of ST elevation 2. Left Bundle Branch Blocks 3. Patient with permanent pacemaker in a paced rhythm 3. STEMI in an arrest 4. Patient has a “do not resuscitate” directive N.B. Ladies and Gentlemen. A few issues/questions to clear up. 1) How long of a delay should the ACP crew wait before deciding to transport to local hospital. The ACP crew will communicate with the CCP Flight Team and/or regional dispatch and the ACP team will decide to wait for CCP Flight Team or transport to Chilliwack Hospital. 2) Inclusion / Exclusion criteria has been formalized and signed off. Helen will develop plastic pocket cards with protocol and inclusion/exclusion criteria for station 206 ACPs. Fraser Health Authority staff: Dr. Anne Clarke, Medical Director Emergency Program Chris Windle, Director Emergency Program Dr. Gerry Simkus, Medical Program Director Cardiac Service Dr. Jan Kornder, Division Head General Cardiology Dr. Albert Chan, Regional Division Head Interventional Cardiology Jackie Murray, Manager Cardiac Catheter lab and 2 North, RCH Mehmud Karmali, Director Clinical Programs FHA Dr. Peter Macdonald, RCH ED Dr. Josh Greggain, FCH ED Corina Vogt, Team Leader FCH Dr. Paul Mallam, CGH ED (not actively engaged at this point) Helen Elliott, STEMI Project Manager of FH British Columbia Ambulance Service Professionalism - Accountability - Responsiveness - Teamwork - Wellness British Columbia Ambulance Service British Columbia Ambulance Service Staff: Robert Wand, Unit Chief / Critical Care Flight Paramedic, Station 280 Rob Sang, A.C.P. lead Chilliwack Tim Philley, Director Operations, Region 2 Michael Boyarski, Unit Chief, Chilliwack Wilf Meyer, District Superintendent, Chilliwack Dr. Steve Blythe, BCAS Co-Medical Director Lower Mainland Dr. Steve Wheeler, Medical Director, Air Programs and CCT Mike Essery, Director of Critical Care and Air Evacuation Bill Penhallurick, Superintendent of Critical Care Programs Tat Ridenour, Charge Dispatcher, Victoria Dispatch – Air Operations Mark King, Superintendent, Victoria Dispatch – Air Operations Gord Kirk, Superintendent, Vancouver Dispatch Operations British Columbia Ambulance Service Professionalism - Accountability - Responsiveness - Teamwork - Wellness