Insulin-like Growth Factor I and Vascular Endothelial Growth Factor
advertisement

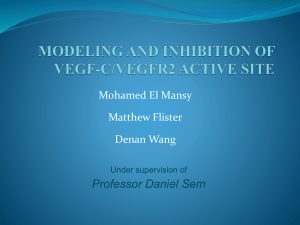
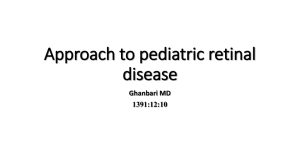
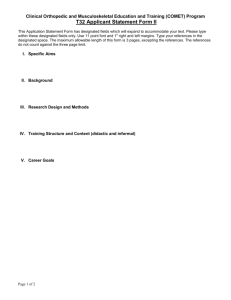
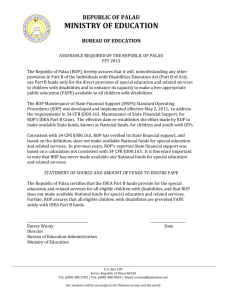
EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 Abdel Wahab et al INSULIN-LIKE GROWTH FACTOR I AND VASCULAR ENDOTHELIAL GROWTH FACTOR AS PREDICTIVE FACTORS IN RETINOPATHY OF PREMATURITY AND OTHER COMPLICATIONS OF PREMATURE BIRTH By Walid Abdel Wahab1,4, Walid Niazy Hassan2 , Ahmed Mahfuz3,4 Departments of Pediatrics1, Biochemistry2, and Community Medicine3, College of Medicine, King Khalid University, Abha, Saudi Arabia, and Aseer Regional Committee of Neonatal Care4 ABSTRACT: Background: Insulin-like growth factor I (IGF-I) and vascular endothelial growth factor (VEGF) are necessary for normal development of retinal blood vessels in mice and humans. We conducted a prospective study measuring serum levels of IGF-I and VEGF in preterm infants who developed complications of prematurity such as retinopathy of prematurity (ROP), bronchopulmonary dysplasia (BPD) and necrotizing enterocolitis (NEC). Also to evaluate their value in the prediction of those complications. Methods: A sample of 62 preterm infants who developed morbidity of prematurity such as ROP (n=31), BPD (n=18) and NEC (n=13) were included in the study. This group consist of 33 male and 29 female, their gestational age was less than 33 weeks (range: 25-32), and their mean birth weight was 961.7 g (range: 640-1200 g). Of the 31 infants with ROP, 19 had non-proliferative ROP and 12 had proliferative ROP. Twenty two preterm infants with no ROP, BPD or NEC of matched age and sex were enrolled in the study as a control group. Serum levels of IFG-I were measured by using radioimmunoassay while, serum VEGF levels were determined by enzyme linked immunosorbent assay (ELISA). Results: Serum levels of IGF-I were significantly lower (p < 0.001) in preterm infants with complications of premature birth than in the control group, however serum levels of VEGF were significantly higher (p < 0.001) in patients than in the controls. Among infants complicated with ROP, serum levels of IGF-I were significantly lower (p< 0.001) in patients with non-proliferative ROP than in those with proliferative ROP. We found that serum levels of VEGF were significantly higher (p< 0.001) in infants who had proliferative ROP than in those with non-proliferative disease. In BPD group, serum levels of IGF-I were significantly lower in patients than in the controls, while serum levels of VEGF were significantly higher in infants with BPD than in those without this morbidity. Serum levels of IGF-I were significantly lower (p< 0.001) in patients with NEC than in the control group. There was a significant positive correlation between IGF-I and VEGF (r= + 0.736; p<0.05). Conclusion: Low serum IGF-I levels predict an increased risk of ROP as well as other complications of premature birth such as BPD and NEC. Replacement of IGF-I to levels found in utero may prevent those complications. High serum VEGF levels predict retinal neovascularization or phase II ROP and carry poor prognosis. AntiVEGF therapy may be a promising strategy for treating retinal neovascular proliferation which can cause blindness. KEYWORDS: Preterm infants Vascular endothelial growth factor 27 Insulin-like growth factor I Retinopathy of prematurity. EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 Abdel Wahab et al Bronchopulmonary dysplasia (BPD) is a significant health problem in preterm infants. It is characterized by arrested alveolar development. Mechanism that regulate alveolar development remains poorly understood. Even less is known about regulation of the growth and development of pulmonary vasculature7. BPD and necrotizing enterocolitis (NEC) are known serious complications of premature birth. IGFI is necessary for the development of nerve, muscle, bone, liver, lung, eye and other body tissues8. IGF-I enhances fetal growth and gastrointestinal development in sheep9. INTRODUCTION: Retinopathy of prematurity (ROP) is a blinding disease, initiated by lack of retinal vascular growth after preterm birth1. The greatest risk factors for development of ROP are low birth weight and low gestational age although the pathogenesis of ROP is multifactorial2. There are both oxygenregulated and non oxygen-regulated factors, which contribute to normal vascular development and retinal neovascularization. A critical non oxygen-regulated growth factor is insulin-like growth factor I (IGF-I) and one important oxygen- regulated factor is vascular endothelial growth factor (VEGF)3. The aim of the study was to mesure serum levels of IGF-I and VEGF in preterm infants who developed complications of prematurity such as ROP, BPD and NEC. Also to evaluate their value in the prediction of those complications. Pathologically, ROP consists of two phases, the first phase (nonproliferative), and the second phase (retinal neovascularization or proliferative) ROP3. SUBJECTS AND METHODS: This study was conducted at neonatal intensive care units of Abha General and Aseer Central Hospitals, Southwestern of Saudi Arabia between January, 2004 to June 2006. A sample of sixty two Preterm infants who developed morbidity of prematurity such as ROP, BPD and NEC were included in the study. This group consist of 33 male and 29 female, their gestational age was less than 33 weeks (range: 25-32), and their mean birth weight was 961.7 g (range: 640-1200 g). Twenty two preterm infants with no ROP, BPD or NEC of matched age and sex were enrolled in the study as a control group. The first phase of ROP in preterm infants consists of cessation of the normal retinal vascular growth which would occur in utero, as well as loss of some of the developed vessels. IGF-I is essential for normal retinal vascular development and lack of IGFI is associated with lack of vascular growth and subsequent initiation of ROP, so IFG-I has a critical role in the development of phase I of ROP. The second phase of ROP, retinal neovascularization, (proliferative ROP) is hypoxia induced and VEGF plays a role in the genesis of this phase3. Recent experimental studies suggest that growth factors such as VEGF and IGF-I can play an important role in the development of ROP, but clinical implications of these findings remain unclear4,5,6. INCLUSION CRITERIA OF THE PATINETS: (A) Patients with ROP: ROP was classified according to the International Classification of 28 EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 ROP (ICROP)10 and subdivided into stage 1 (demarcation line), stage 2 (ridge), stage 3 (ridge with extraretinal fibrovascular proliferations), stage 4 (subtotal retinal detachment), and stage 5 (total retinal detachment). Nonproliferative ROP was defined as stage 1 and 2, however, stage 3 and 4 are considered as proliferative ROP11. The preterm infants were evaluated according to the protocol of screening of ROP12. Initial examination was performed by 31 weeks postmenstrual or 4 weeks chronological age, which is later. Follow up fundus examinations once or twice a week until the eyes were fully vascularized or until the condition was stable. Diagnosis of ROP was done by consultant ophthalmologist by using indirect ophthalmoscopy. Abdel Wahab et al with corticosteroids had been reported to alter serum IGF-I in neonates16. Venous blood samples (1 ml) were obtained from both patients and control groups. Sera were separated and stored at -800C until the assay. IGF-I assay Serum levels of IGF-I were measured by using radioimmunoassay [RIA] (Mediagnost GmbH, Tuingen, Germany). As the presence of IGF-Ibinding proteins in the serum interferes in the RIA procedure, these proteins were removed. Serum samples were extracted with formic acid and acetone as described previously 17. Because this extraction method does not eliminate all IGF-I-binding proteins present in the serum acid-acetone extracts were subjected to cryoprecipitation, a procedure described previously 17. The mean recoveries of iodinated IGF-I added to the serum were 90.5%. The Tris-neutralized serum extracts were diluted with RIA buffer containing 0.02% protamine sulfate and 0.05% Tween-20. Diluted seum extracts (1:50) were used in this RIA. The purified recombinant human IGF-I preparation purchased from Amgen, Inc. (Thousand Oaks, CA) was used as the reference preparation, and human IGF-I (A52–8MH-144; Eli Lilly & (B) Patients with BPD: Bronchopulmonary dysplasia and chronic lung disease (CLD) are still used in the literature interchangeably, however, CLD is considered as stage IV of BPD according to Northway stages of BPD13. Diagnosis of BPD was based on the typical appearance of BPD on serial chest radiographs13. Diagnosis of CLD was based on the need of preterm infants for oxygen supplementation at 36 weeks postconception14. Patients with BPD who enrolled in the study had stage II or III. Co., Indianapolis, IN) was iodinated and used as trace. Antiserum prepared against human IGF-I was used in this RIA. All serum extracts were included in the same assay to avoid interassay variability and IGF-I was measured in duplicate by a IGF radioimmunoassy of around 250-fold excess of IGF17. (C) Patients with NEC: Diagnosis of NEC was done according to modified Bell’s criteria and staging for NEC. It depends on clinical, radiological and laboratory findings15. Preterm infants with congenital anomalies or had been given corticosteroids for more than 14 days were excluded from the study. Treatment VEGF assay Serum VEGF levels were determined using a sensitive sandwich ELISA (R&D Systems, Minneapolis, 29 EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 MN, USA). A quantitative enzyme immunoassay was performed using micro-well plates pre-coated with monoclonal antibody. For each study participant, 100 µl of serum or standards were added to the wells and the unbound materials were washed off. An enzyme-linked polyclonal antibody that is specific for human VEGF was added, and unbound antibody was removed by washing the plate. Tetramethylbenzidine and hydrogen peroxide was added to the wells, developed, and read on a microplate spectrophotometer at 450-nm wavelength. All analyses were performed in duplicate. Concentrations were expressed in pg/ml. The detection limit of the VEGF assay was 9 pg/ml. Abdel Wahab et al III (n = 18) and the third group had necrotizing enterocolitis (n = 13). Of the 31 patients with ROP, 19 had nonproliferative (stage I & II) ROP and 12 had proliferative (stage III & IV) ROP. No infant developed ROP stage V. Characteristics of patients and controls are shown in table 1. Serum levels of IGF-I were significantly lower (p < 0.001) in preterm infants with complications of premature birth than in the control group, however serum levels of VEGF were significantly higher (p < 0.001) in patients than in the controls (figure 1). Among infants complicated with ROP, serum levels of IGF-I were significantly lower (p< 0.001) in patients with non-proliferative ROP than in those with proliferative ROP. We found that serum levels of VEGF were significantly higher (p< 0.001) in infants who had proliferative ROP than in those with non-proliferative disease as shown in table 2. Statistical analysis: Values were expressed as mean + standard deviation (SD). The significance of comparison between mean values of two groups was evaluated by student t-test. However, the significance of comparison between more than one group was performed by ANOVA for parametric continuous variables. Simple Pearson correlation coefficient was calculated to quantify the correlation between serum levels IGF-I and VEGF in preterm infants with ROP. Significant differences were denoted by p < 0.05. Statistical analysis was performed by using the (SPSS) software. RESULTS: We studied 62 preterm infants with complications of premature birth in addition to 22 preterm neonates of matched gestational age and sex (without complications) as a control group. Preterm infants with complications of prematurity were divided into 3 groups; the first group developed retinopathy of prematurity (n = 31), the second group had bronchopulmonary dysplasia stage II & In BPD group, serum levels of IGF-I were significantly lower in patients than in the control group. Serum levels of VEGF were significantly higher in infants with BPD than in those without this morbidity (figure 2). Figure 3 shows the serum levels of IGF-I and VEGF in preterm infants who developed NEC. Serum levels of IGF-I were significantly lower (p< 0.001) in patients with NEC than in the control group. Regarding serum levels of VEGF, we found no significant difference between patients and controls. There was a significant positive correlation between IGF-I and VEGF (r= + 0.736; p<0.05) in preterm infants with ROP.. 30 EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 Abdel Wahab et al Table 1. Characteristics of patients and controls NonProliferative BPD proliferative ROP (Stage II &III) ROP (Stage I, II) (Stage III, IV) (n = 18) (n = 19) (n = 12) Gestational age, weeks Mean + SD Range Birth weight, gram (Mean + SD) Sex; Male, n (%) Female, n (%) 28.5 + 1.5 26-31 26.9 + 1.0 25-29 28.5 + 1.3 26-30 971.8 + 155.5 842.1 + 142.9 10 (53) 9 (47) 7 (58) 5 (42) NEC (n = 13) Controls (n = 22) 28.5 + 1.8 26-33 28.9 + 1.7 26-32 958.3 + 153.5 1006.5+ 176.6 9 (50) 9 (50) 994.3 + 203.7 7 (54) 6 (46) 70 * 60 Serum level 50 40 Control Patients 30 * 20 10 0 IGF-1 (mg/L) VEGF (Pg/ml) Figure 1. Serum levels of IGF-I and VEGF in preterm infants with complications (ROP, BPD, NEC) (n = 62) and controls (n = 22). * p < 0.001 Table 2: Serum levels of IGF-I and VEGF in preterm infants with ROP and controls IGF-I (ug / L) VEGF (Pg / ml) Non-proliferative ROP (Stage I, II) (n = 19) Proliferative ROP (Stage III, IV) (n = 12) Controls (n = 22) 11.2 + 3.8 49.2 + 4.1 20.8 + 2.5 77.9 + 7.2 40.8 + 3.5* 32.7 + 5.4* Values are mean + SD ; * p < 0.001 31 12 (55) 10 (45) EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 70 Abdel Wahab et al * 60 serum levels 50 40 30 Control BPD * 20 10 0 IGF-1 (mg/L) VEGF (Pg/ml) Figure 2. Serum levels of IGF-I and VEGF in preterm infants with BPD (Stage II &III) (n = 18) and controls (n = 22). * p < 0.001 50 ** 45 40 Serum level 35 30 25 Control * NEC 20 15 10 5 0 IGF-1 (mg/L) VEGF (Pg/ml) Figure 3. Serum levels of IGF-I and VEGF in preterm infants with NEC (n = 13) and controls (n = 22). * p < 0.001, **p = 0.04 significantly lower in patients with non-proliferative than in those with proliferative ROP. The critical role of IGF-I system in retinal vascular development had been confirmed in a clinical study done by Hellstrom and his colleagues where patients with defects in IGF-I or IGF-I receptor gene DISCUSSION: Our study showed that serum concentrations of IGF-I were significantly lower in preterm infants with ROP than in those without this complication. These data are in consistent with the results of studies done by Smith18 and Lofqvist19. We found that serum levels of IGF-I were 32 EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 were found to have a reduced number of retinal vascular branching points20. Abdel Wahab et al confirming the central role of VEGF in neovascular eye disease25-27. Our data showed that serum levels of VEGF were statistically higher in preterm infants with ROP than in those without the disease. Also we found higher serum concentrations of VEGF in infants with proliferative than those with non-prolifrative ROP and these findings are in accordance with the results of study that was conducted by Brady-MacCreery28. Our results support the role of VEGF in the genesis of ROP especially the proliferative phase of the disease. Smith reviewed the significant role of low serum IGF-I concentration in the genesis of ROP. Since the proliferative phase of ROP is induced by retinal hypoxia consequent to the retinal vascular growth arrest of the first phase in which low serum IGF-I concentration plays a pivotal role, Smith proposed that the second proliferative phase would not occur if the first phase was prevented3. Our results support that in preterm infants, early restoration of IGF-I to levels similar to those present in utero might prevent ROP by promoting normal vascular development. This perhaps could be accomplished by assuring sufficient nutrient intake. We found a significant positive correlation between serum levels of IGF-I and VEGF in preterm infants with ROP. Also we noticed that serum levels of IGF-I were significantly higher in patients with proliferative than in those with non-proliferative ROP. These findings indicate that IGFI is important and VEGF alone may not be sufficient for promoting vigorous retinal angiogenesis. IGF-I is a nutrient-dependent factor (e.g. diary products and germinated barley), insufficient intake of nutrients will result in a further decline of this peptide. Sufficient nutrient intake during pregnancy is important to reduce the risk of ROP21. Early breast feeding may be particularly beneficial at it has been shown that breast milk contains available amount of IGF-I22. Alexander in his study tried administration of insulin-like growth factor binding protein-3 (IGFBP-3) to preterm babies and found that it stabilized the existing vessels in the retina, also block the neovascularization. So administration of this protein to preterm infants might prevent ROP damage23. In murine mouse of retinopathy, it was shown that IGF-I enhances the production of VEGF by using IGF-I receptor antagonism which inhibited retinal neovascularization by decreasing the expression of both VEGF and VEGF receptors29. Also IGF-I regulates VEGF stimulation of Akt / PKB (protein-kinase B) phosphorylation, which is central in the signaling pathway of cell proliferation30. Chronic lung disease is considered as stage IV of BPD according to Northway stages of BPD13. Our study showed that serum concentrations of IGF-I were significantly lower in preterm babies who developed BPD (stage II or III) than in those without this complication. These results are in consistent with In the mouse, retinal hypoxia stimulates an increase in the expression of VEGF before the development of neovascularization4,24. Other investigators have also shown that VEGF is associated with ocular neovascularization in other animal models, 33 EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 those of studies done by Pierce31, Chetty32 and Capoluongo33. We found that serum levels of VEGF were significantly higher in patients with BPD (stage II or III) than in preterm infants without this morbidity. Lung blood vessels actively promote alveolar growth during development and contribute to the maintenance of alveolar structures throughout postnatal life. Disruption of angiogenesis impairs alveolarization and preservation of vascular growth and endothelial survival promotes growth and sustains the architecture of the distal airspace7. Abdel Wahab et al and gut of the preterm infants so could prevent BPD and NEC. High serum VEGF levels predict retinal neovascularization or phase II ROP and carry poor prognosis. AntiVEGF therapy may be a promising strategy for treating retinal neovascular proliferation which can cause blindness. REFERENCES: 1. Quiram Polly A, Antonio Jr.: Current understanding and management of retinopathy of prematurity. Contemporary Ophthalmology 2007; 6(22): 1-7 2. Simons BD, Flynn JT.: Retinopathy of prematurity and associated factors. Int Ophthalmol Clin 1999; 39:29-48 3. Smith LE.: Pathogenesis of retinopathy of prematurity. Acta Paediatr 2002; 437:26-28 4. Pierce EA, Avery RL, Foley ED, et al.,: Vascular endothelial growth factor / vascular permeability factor expression in a mouse model of retinal neovascularization. Proc. Natl. Acad. Sci. USA 1995; 92: 905-909 5. Stone J, et al.,: Roles of vascular endothelial growth factor and astrocyte degeneration in the genesis of retinopathy of prematurity. Invest. Ophthalmol. Vis. Sci. 1996; 37: 290299 6. Okamoto N, Tobe T, Hackett S, et al.,: Transgenic mice with increased expression of vascular endothelial growth factor in retina: a new model of intraretinal and subretinal neovascularization. Am J Pathol 1997; 151:281-291 7. Thebaud B, Steven H.: Bronchopulmonary dysplasia: where have all the vessels gene? Role of angiogenic growth factors in chronic lung disease. Am J Respiratory & Critical Care Medicine 2007; 175 (10): 978-85 Our data showed that serum levels of IGF-I were significantly lower in preterm infants who developed NEC than in those without this complication. Hypoxia-reoxygenation induces NEC by increasing the apoptosis of the intestinal mucosa in the young mice and human. IGF-I is a known anti-apoptotic factor. It protects the intestinal mucosa from apoptosis or intestinal injury34, 35. IGFI supplementation during pregnancy may be beneficial for the normal development of gastrointestinal tract 21. On other hand VEGF serum levels shown to be not significantly increased in the NEC patients implying that the role of neovascularisation is not involved in the development of NEC. CONCLUSION: Low serum IGF-I levels predict an increased risk of ROP as well as other morbidities of premature birth such as BPD and NEC. Replacement of IGF-I to levels found in utero may prevent ROP by promoting normal vascular development and if phase I of ROP is aborted, the destructive second phase of vasoproliferation will not occur. Also administration of IGF-I enhances other organ development such as lungs 34 EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 8. Alexander VL. Protein may prevent ROP damage. Review of Ophtalmology 2007; 7:6-8 9. Kimble RM, Breier BH, Gluckman PD, et al.,: Enteral IGF-I enhances fetal growth and gastrointestinal development in oesphageal ligated fetal sheep. J Endocrinol 1999; 162:227-235 10. Committee for the classifycation of retinopathy of prematurity.: An international classify-cation of retinopathy of prematurity. Arch Ophthalmol 1984; 106:471-479 11. International committee for the classification of the late stages of retinopathy of prematurity. An international classification of retinopathy of prematurity: II. The classification of retinal detachment. Arch Ophthamol 1987; 105: 906-912 12. Reynolds JD, Dobson V, Quinn GE, et al.,: CRYO-ROP, LIGHT-ROP Cooperative Groups. Evidence-based screening criteria for retinopathy of prematurity: natural history data from the CRYO-ROP, LIGHT-ROP studies. Arch Ophthalmol 2002; 120: 14701476 13. Northway WH, Moss RB, Karlisle KB, et al.,: Late sequela of bronchopulmonary dysplasia. N Engl J Med 1990; 323: 1793-1799 14. Barrington KJ, Finner NN.: Traetment of bronchopulmonary dysplasia. Clin Perinatol 1998; 25: 177-202 15. Bell MJ, Ternberg JL, Feigin RD, et al.,: Neonatal necrotizing enterocolitis. Therapeutic decision based upon clinical staging. Ann Surg 1978; 187: 1-7 16. Skinner A, Battin M, Solimano A, et al.,: Growth and growth factors in premature infants recieving dexamethsone for bronchopulmonary dysplasia. Am J Perinatol 1997; 14: 539-46 17. Blum W, Breier B.: Radioimmunoassays for IGFs and IGFPBs. Growth Regul 1994; 4: 11-9 Abdel Wahab et al 18. Smith LE.: IGF-I and retinopathy of prematurity in the preterm infant. Biol Neonate 2005;/88:/237- 44 19. Lofqvist C, Andersson E, Sigurdsson J, et al.,: Longitudinal postnatal weight and insulin-like growth factor I measurements in the prediction of retinopathy of prematurity. Archives of Ophthalmology 2006; 124 (12):1711-1718 20. Hellstrom A, Carlsson B, Niklasson A, et al.,: IGF-I is critical for normal vascularization of the human retina. J Clin Endocrinol Metab 2002;/87:/3413-6 21. Smith WJ, Underwood LE, Keyes L, et al.,: Use of insulin-like growth factor I (IGF-I) and IGFbinding protein measurements to monitor feeding of premature infants. J Clin Endocrinol Metab 1997; 82: 3982-3988 22. Elmlinger MW, Grund R, Buck M, et al.,: limited proteolysis of IGF binding protein-2 (IGFBP-2) by a specific protease activity in early breast milk. Pediatr Res 1999;46:76-81 23. Alexander VL.: Protein may prevent ROP damage. Review of Ophthalmology 2007; 7: 6-8 24. Smith LE, Wesolowski E, McLellan A, et al.,: Oxygen-induced retinopathy in the mouse. Invest Ophthalmol Vis. Sci. 1994; 35:101-111 25. Donahue ML, Phelps DL, Watkins RH, et al.,: Retinal vascular endothelial growth factor (VEGF) m RNA expression is altered in relation to neovascularization in oxygen induced retinopathy. Curr Eye Res 1996; 15: 175-84 26. Adamis AP, Shima DT, Tolentio MJ et al.,: Inhibition of vascular endothelial growth factor prevents retinal ischemia-associated iris neovascularization in a non-human primate. Arch Ophthalmol 1996; 114: 66-71 27. Young TL, Anthony DC, Pierce E, et al.,: Histopathology and vascular 35 EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 endothelial growth factor in untreated and diode laser-treated retinopathy of prematurity. J Aapos 1997; 1: 105-10 28. Brady-MacCreery KM, McCreery CJ, Sriram V, et al.,: Serum vascular endothelial growth factor and threshold retinopathy of prematurity. Proc Annual Meeting American Academy of Ophthalmology; 2001: abstract 113.3 29. Roninson G.: Oligodeoxynucleotides inhibit retinal neovascularization in a murine model of proliferative retinopathy. Proc Natl Acad Sci USA 1996; 93: 4851-4856 30. Alon T, Hemo I, Itin A, et al.,: Vascular endothelial growth factor acts as a survival factor for newly formed retinal vessels and has implications for retinopathy of prematurity. Nat Med 1995;/1:/1024-8 31. Pierce WA, Lee Edward, Maynor A, et al.,: Relation between serum insulin-like growth factor I, insulin-like growth factor binding protein-2, insulin-like growth factor binding protein-3 and nutritional intake Abdel Wahab et al in premature infants with bronchopulmonary dysplasia. Journal of Pediatric Gastroenterology & Nutrition 2001; 32 (5): 542-549 32. Chetty A, Anderson S, Nielson HC.: Insulin-like growth factor (IGF-I) and IGF-I receptor (IGF-IR) expression in human lung in RDS and BPD. Pediatr Pulmonol 2004; 37: 12836 33. Capoluongo E, Ameglio F, Lulli P, et al.,: Epithelial lining fluid free IGF-I to PAPP ratio is associated with bronchopulmonary dysplasia in preterm infants. Am J Physiol Endocrinol Metab 2007; 292: 308-313 34. Baserga R, Hongo A, Rubin M, et al.,: The IGF-receptor in cell growth, transformation and apoptosis. Biochem Biophys Acta 1997; 1332: 105-126 35. Akisul M, Ozen S, Baka M, et al.,: Insulin like growth factor attenuates apoptosis and mucosal damage in hypoxia / reoxygenationinduced experimental necrotizing enterocolitis. Pediatr Res 2004; 56: 464-9 ومعامل نمو األوعية الدموية كعوامل تنبؤ فى1-”معامل النمو المماثل لألنسولين “األطفال الخدج المصابين باعتالل شبكية العين ومضاعفات الوالدة المبكرة 3 أحمد محفوظ.د. أ,2 وليد نيا زى. د.أ,1وليد عبد الوهاب عيد.د المملكة- أبها-جامعة الملك خالد- كلية الطب-3 الصحة العامة,2 الكيمياء الحيوية,1طب األطفال العربية السعودية :خلفية وهدف البحث يعتبر مرض اعتالل شبكية العين فى األطفال الخدج (غير مكتملي العمر الرحمي) من ومعامل نمو1- معامل النمو المماثل لألنسولين.األمراض الخطيرة التى قد تؤدى إلى العمى والهدف من وراء.األوعية الدموية ضروريين لنمو وتطور األوعية الدموية بشبكية العين البحث هو قياس مستوى هذان العامالن فى دم األطفال الخدج المصابين بمضاعفات الوالدة المبكرة ومنها اعتالل شبكية العين و اعتالل الرئة والقصيبات الهوائية وأيضا االلتهاب المعوي .المتحلل وكذلك التعرف على دورهم في التنبؤبتلك المضاعفات :طريقة البحث أسبوع وكانت32-25 تراوحت أعمارهم الحملية بين, طفال خديجا62 شملت الدراسة : قسم هؤالء األطفال إلى ثالث مجموعات. جرام1200-640 أوزانهم عند الوالدة بين 18 طفال مصابا باعتالل الشبكية و المجموعة الثانية وشملت31 المجموعة األولى وشملت طفال13 طفال مصابا باعتالل الرئة والقصيبات الهوائية والمجموعة الثالثة والتى احتوت على 36 Abdel Wahab et al EL-MINIA MED., BULL., VOL. 19, NO. 1, JAN., 2008 مصابا بااللتهاب المعوي المتحلل .كما اشتملت الدراسة على عدد 22طفال من األطفال الخدج الغير مصابين بمضاعفات الخداجة ولهم نفس الجنس والسن كمجموعة ضابطة .من بين األطفال المصابين باعتالل شبكية العين ,كان هناك عدد 19طفال مصابا بدرجة متوسطة من اعتالل الشبكية و 12طفال مصابا بدرجة شديدة من المرض. تم قياس مستوى معامل النمو المماثل لألنسولين 1-ومعامل نمو األوعية الدموية فى الدم لكال المجموعتين التجريبية والضابطة بواسطة اختبار اإلشعاع المناعي. نتائج البحث: أظهرت الدراسة انخفاض مستوى معامل النمو المماثل لألنسولين 1-فى دم األطفال المصابون بمضاعفات الخداجة عند مقارنتهم بالمجموعة الضابطة .وكان هذا االنخفاض أكبر فى األطفال المصابين بدرجة متوسطة من اعتالل الشبكية عن اآلخرين المصابين بالدرجة الشديدة من االعتالل .كما أظهرت النتائج ارتفاع مستوى معامل نمو األوعية الدموية فى دم األطفال المصابون بمضاعفات الخداجة عن أطفال المجموعة الضابطة ,وكانت نسبة االرتفاع أكبر فى األطفال المصابين بدرجة متقدمة من اعتالل الشبكية عن األطفال المصابين بدرجة متوسطة من هذا المرض.وكانت لكل تلك الفروق دالالت إحصائية واضحة .فى هذه الدراسة الحظنا وجود عالقة إيجابية ذات داللة إحصائية بين مستوى معاملي النمو فى مجموعة األطفال المصابين باعتالل شبكية العين. اإلستنتاجات: انخفاض مستوى معامل النمو المماثل لألنسولين 1-فى األطفال المصابين باعتالل الشبكية له أهمية فى توقع حدوث المرض لذا معالجة هذا اإلنخفاض قد يمنع حدوث االعتالل ومضاعفاته كما انه يساعد على منع مضاعفات الخداجة األخرى .ارتفاع مستوى معامل نمو األوعية الدموية فى األطفال المصابين بدرجة متقدمة من اعتالل شبكية العين يشير إلى دوره فى تحديد األطفال المعرضين لحدوث المضاعفات وإعطاء الدواء المضاد لعامل نمو األوعية الدموية فى تلك المرحلة من اعتالل الشبكية قد يكون له دور فى المستقبل فى منع حدوث العمى عند هؤالء األطفال. 37