Magnesium Sulfate Orders for Tocolytic Therapy
advertisement

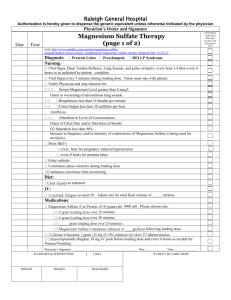
PLACE LABEL HERE MAGNESIUM SULFATE ORDERS FOR TOCOLYTIC THERAPY The following orders will be implemented. Orders with a “” are choices and are NOT ordered unless checked. Initial all hadwritten order modifications and the bottom of each page when indicated. Allergies: ________________________________________________________________________________ Diabetic: Yes No 1. Diagnosis & Status: Admit as Inpatient to L&D ___________________________________(reason for admission) 2. In addition to these orders, follow: Generic Antepartum Orders (form # 15603) Other: ________________________________________________ ASSESSMENTS: 3. Obtain baseline maternal/fetal assessments prior to initiation of therapy. This includes maternal vital signs, breath sounds, deep tendon reflexes (DTRs), oxygen saturation, level of consciousness, fetal heart rate (FHR), and uterine activity. 4. Maternal/fetal assessments per routine, or more often if clinical condition warrants: Antepartum Blood pressure & heart Every 5 minutes during loading dose, rate then every 15 minutes for the first hour, then every 30 minutes for the second hour, then hourly. Respiratory rate Every 15 minutes for the first hour, then every 30 minutes for the second hour, then hourly. FHR & uterine activity Continuously Document with each set of maternal vital signs. DTRs Every hour Intake & output Every hour Level of consciousness Every hour Breath sounds Every 2 hours SaO2 (pulse oximetry) Every hour IV site assessment Every 2 hours Fundus/lochia N/A 5. Transfer to High Risk Pregnancy Unit when the following criteria have been met for 6-12 hrs: Maintenance dose has not been increased Uterine activity has been below threshold with no cervical change Maternal vital signs and FHR are stable with maternal respiratory rate at or above 16 Urine output is above 30 ml/hr or 120 ml/4 hrs DTRs are at least 1+ Serum magnesium level is below 8 mg/dl (if ordered) Order writer’s initials _________ *3-18086* FORM 3-18086 REV. 07/2012 WHITE: Medical Record CANARY: Pharmacy Page 1 of 2 PLACE LABEL HERE MAGNESIUM SULFATE ORDERS FOR TOCOLYTIC THERAPY The following orders will be implemented. Orders with a “” are choices and are NOT ordered unless checked. Initial all hadwritten order modifications and the bottom of each page when indicated. 6. Notify physician immediately if patient has: Uterine contractions: _______ or more per hr Significant changes in BP from baseline values Double (or blurring) of vision Tachycardia or bradycardia Respiratory rate below 14 or above 24 Oxygen saturation below 95% Adventitious lung sounds Changes in level of consciousness or neurological status Absence of DTRs Urine output less than 30 ml/hr for 2 consecutive hrs (or less than 120 ml in fours if no Foley) Category III FHR patterns (anticipate minimal variability and loss of accelerations) Vaginal bleeding 7. If respirations < 12, discontinue magnesium sulfate, notify Physician, and give supplemental O2 to keep O2 sat > 95%. 8. Foley catheter to bedside bag OR do not insert Foley; may use bedpan 9. Activity: Strict bedrest OR Bedside commode (for BM) with assistance Bedrest with bathroom privileges with assistance 10. Hygiene: Bed bath OR Shower with assistance IVF/SCHEDULED MEDICATIONS: 11. LR as primary fluids. Maintain total IV intake at 125 ml/hr, or ______________________________ 12. Loading dose: Magnesium Sulfate 4 gram IV loading dose over 20 min x 1 dose Magnesium Sulfate 6 gram IV loading dose over 20 min x 1 dose 13. Maintenance: at completion of magnesium sulfate loading dose, run maintenance infusion at ________ gms/hr IV PRN MEDICATIONS: 14. Respiratory Arrest: Calcium gluconate 10%, 1 gm (10 ml) IV push over 3-5 minutes prn and assess VS q 5 min until respiratory rate is ≥ 12, SaO2 is >95%; then every 15 min x one hr, then resume per above ADDITIONAL ORDERS: ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________ Date ___________________ Time FORM 3-18086 REV. 07/2012 _________________________________ Physician Signature WHITE: Medical Record CANARY: Pharmacy ___________ PID Number Page 2 of 2