Resident Thyroid storm module: Created by Kathleen Colleran, MD
advertisement

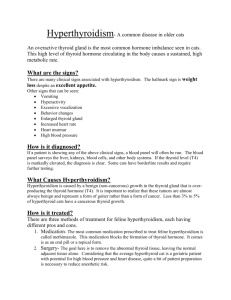
Attending Version Thyroid Storm Module: Created by Kathleen Colleran, MD Objectives: 1) you will recognize the signs and symptoms of thyroid storm and why they occur 2) you will be able to appropriately evaluate a patient with suspected thyroid storm 3) you will understand how to treat thyroid storm References: 1. McKeown, N, et al. Hyperthyroidism. Emergency Medicine Clinics of North America 23:669-85, 2005. 2. Migneco A, et al. Management of Thyrotoxic Crisis. Eur Rev Med Pharmacol Sci. 9:69-74, 2005. 3. Douglas S Ross, MD, Treatment of Thyroid storm @ 2006 UpToDate . Overview of Thyroid storm Thyroid storm is a medical emergency that includes hyperthyroidism, cardiovascular instability, thermogenic instability, and neurogenic instability. The diagnosis of thyroid storm is based signs and symptoms and is a clinical diagnosis. Being able to recognize the manifestations of thyroid storm thus is essential to expedite treatment and prevent morbidity and mortality. Even with appropriate treatment mortality rates for thyroid storm remain high at 25%. All forms of hyperthyroidism can culminate in thyroid storm. Table 1 list causes of hyperthyroidism. Grave’s disease accounts for most cases of thyroid storm because it is common and severe hyperthyroidism can occur. Thyroid storm typically occurs in a patient with underlying hyperthyroidism, either previously known or unknown, who develops a second illness or stressor. The second stressor results in an acute catecholamine surge. The catecholamine surge in the presence of hyperthyroidism leads to tachyarthymias, high output cardiac failure and cardiovascular instability. Elevated catecholamine in the setting of hyperthyroidism causes hyperthermia leading to thermodynamic instability. The combination also causes tremors, hyperreflexia, mania, concentration and memory disturbances and culminates in neuropsychiatric instability. Common precipitants of thyroid storm are listed in table 2. Thyroid storm can mimic several conditions including sepsis, pheochromocytoma, psychosis, adrenal insufficiency, intoxication, and autonomic insufficiency. Table 1. Causes of hyperthyroidism Graves’ Disease Toxic Multinodular Goiter Toxic Adenoma Thyroiditis Exogenous Thyroid Hormone Thyroiditis Jod Basedow TSH Secreting Pituitary Adenoma Molar Pregnancy Struma Ovarii Table 2. Precipitants of Thyroid Storm Pregnancy Trauma Infection Myocardial Infarction Surgery Intoxication ETOH Cocaine Amphetamines Iodine ( in MNG, Toxic adenoma) Radioactive Iodine IV Contrast Amiodarone Clinical Assessment The diagnosis of thyroid storm is made by clinical suspicion based on patient history, signs and symptoms and physical exam findings. Waiting for thyroid function tests to return leads to unnecessary treatment delays and can be catastrophic. Most patients will report a history of symptoms consistent with hyperthyroidism including unexplained weight loss, insomnia, heat intolerance, tremors, and palpitations. They will present with an acute worsening of those symptoms in addition to severe agitation. Significant physical exam findings include agitation and inability to sit still. Temperature is usually elevated, significant tachycardia is present and blood pressure is labile. Skin is moist and warm to touch. Eye examination may demonstrate stare, lid lag, or exopthalmos if Graves’ disease is present. Thyroid exam findings depend on the etiology of hyperthyroidism (table 3). Muscle weakness and hyperreflexia may be present. Additionally, patients perform poorly on the mini mental status exam. Standard laboratory analysis including a full metabolic profile and CBC is nonspecific. Table 3. Graves’ Disease Toxic Multinodular Goiter Toxic Adenoma Thyroiditis Exogenous thyroid intake TSH secreting pituitary tumor Molar pregnancy Strumii ovarie Diffusely enlarged gland bruit Nodular goiter Solitary nodule tenderness Nonpalpable gland Diffusely enlarged gland Diffusely enlarged gland Nonpalpable gland C. Treatment Treatment of thyroid storm is empiric based on clinical suspicion. Patients should be admitted to an intensive care unit. Treatment is multifactorial and includes supportive care and pharmacologic intervention. Pharmacologic treatment is aimed at blocking thyroid hormone synthesis, release, conversion to T3, and action on cells. Figure 1 demonstrates where pharmacologic therapies are acting. Fluid as patients are volume deplete Cooling blankets if hyperthermia is present Beta blockade to minimize catecholamine excess o Propranolol 20-40 mg q 6 hours to decrease heart rate to < 100 bpm o Esmolol if concern regarding cardiac output (fast acting/short t ½ life.) Thionamides: o Propothyouricil (PTU) 150 mg po q 6 hours if patient is able to take p.o. Or o Methimazole 10-20 mg pr q 6 hours SSKI or Lugol's solution: administer 1-2 hours following thionamide administration. Steroids: Dexamethasone 1 mg q 6-8 hours Treat underlying precipitating stressor if present If no response consider emergent thyroidectomy or plasmaphoresis. Aviod aspirin; it increases free thyroid hormone levels by competing with binding sites on Thyroid binding globulin Figure 1. T-4 Synthesis Thionamides T3 activity T-4 release Iodine T-4 T3 PTU Propranolol Steroids β-blockers Steroids D. Pharmacology: PTU has a shorter t ½ and faster onset of action than methimazole. PTU preferentially blocks conversion of T4 to T3 (active hormone) PTU is preferred during pregnancy as methimazole may cause a XXXX Both agents can cause agranulocytosis and hepatitis (<0.1%). These adverse events are idiosyncratic can occur randomly; therefore monitoring WBC or LFTs are not useful. Patients should be educated to get a blood test done if they develop symptoms of neutropenia including: unexplained fever, sore throat, or mouth sores; or if they develop symptoms of hepatitis including: right upper quadrant pain, jaundice, or nausea or vomiting. E. Clinical Case D.Y is a 19 yr old male was involved in a low speed motor vehicle accident. At the scene, he complained of neck pain. A C-collar was placed and he was transferred by ambulance to the local Emergency room. On initial presentation he was warm to touch, anxious with a mild tremor, and tachycardic with a HR of 125. He was tender over the c-spine but demonstrated no focal neurological deficits. The remainder of his physical exam was nonspecific. An XRAY of the C-spine was ordered. Over the course of his ER stay he became progressively agitated, confused and combative. His HR increased to 160 and temperature rose to 40◦ C. He was visibly shaking and unable to sit still. He required sedation and restraints. He was incubated for airway protection and respiratory support and was transferred to a tertiary care center and admitted to an ICU bed. A full metabolic panel, CBC, blood and urine cultures, and a toxicology screen were ordered. EKG showed sinus tachycardia, CXR was negative, C-spine was difficult to interpret and a CT was ordered. What should be initial management step and what further tests should be ordered? He received IV fluids with no improvement in his heart rate. His labs were all WNL except for + cocaine and methamphetamines on the toxic screen. He remained tachycardic and febrile. Thyroid function tests were performed. His TSH was undetectable and his Free T4 was >6 mg/do. A diagnosis of thyroid storm was made. What would be reasonable treatment for his diagnosis, and what precipitated it? He was started on propranolol 60 mg iv q 6 hours, PTU 150 mg po q 6 hours, Dexamethasone 2 mg iv q 6 hours. 2 hours after the first does of PTU he received SSKI 6 drops po q 6 hours. Once his c-spine was cleared by CT scan, the c-collar was removed. A diffusely enlarge thyroid gland was visible on gross inspection. Three days after admission the patients heart rate was 92, Temp was 37.3, he was mentating normally, and was able to report a 20 pound weight loss over the preceding 3-months, insomnia and heat intolerance. A diagnosis of Graves’ disease was made and the patient was discharged on PTU, and propranolol. In summary, this patient had undiagnosed hyperthyroidism secondary to Graves’ disease. He then used methamphetamines and cocaine and was in a low speed motor vehicle accident. These two stressors pushed him into thyroid storm. Failure to do a full physical examination including removing the C-collar to assess his thyroid led to a significant delay in diagnosis and treatment which could have led to significant morbidity and mortality. Thyroid storm is diagnosed based on clinical suspicion and includes hyperthyroidism coupled with another physiologic stressor. E. Board Review Questions 1. A 64 yr. old male presents to the ED with angina and hyperthyroidism. He is scheduled to undergo cardiac catheterization. This procedure will result in a worsening of his hyperthyroidism if he has which of the following: a. Viral Thyroiditis b. Toxic Multinodular Goiter c. Graves’ Disease d. Hashimotos Thyroiditis e. Thyroid Hormone Resistance Answer is B. The iodine in the contrast dye used during cardiac catheterization can precipitate thyroid storm in Multinodular goiter and toxic adenoma. 2. A 40-yr-old female with Grave’s disease was recently started on methimazole. One month later she comes to the clinic for a routine follow-up. She reports low grade fevers, myalgias, arthralgias, and general malaise. The most important test to order now is which of the following? a. TSH b. ALT c. TSI d. WBC e. Radio iodine uptake Answer is D. Adverse effects of methimazole include bone marrow suppression resulting in agranulocytosis or aplastic anemia. If patient is neutropenic, she is at high risk for infection.