STATEWIDE INFECTION CONTROL PROGRAM
advertisement

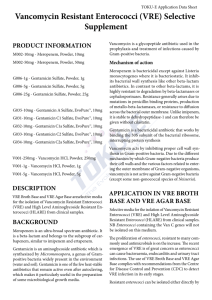
-----------------------------------------------------------------------------------------------------------------REPORT OF THE MONTH, Volume IV, Number 6 - November-December 2000 - - - - from the North Carolina Statewide Program for Infection Control and Epidemiology -----------------------------------------------------------------------------------------------------------------CONTENTS: NEWS FEATURES Patient Attire in Ambulatory Surgery Fabric-covered Furniture - a Reservoir for VRE REGULATORY/LEGISLATIVE Needlestick Safety Prevention Act QUESTION OF THE MONTH Banked Breast Milk Given to the Wrong Baby NEWS AND ANNOUNCEMENTS COURSES FOR THE INFECTION CONTROL PROFESSIONAL HOLIDAY FUN Grinchy Germs in Heelville -----------------------------------------------------------------------------------------------------------------NEWS FEATURES PATIENT ATTIRE IN AMBULATORY SURGERY In the 1990's a dramatic shift in patient-care practices occurred as greater than 65% of surgery cases were operated on in outpatient settings. In an effort to provide patients with cost-effective, convenient, efficient care in the ambulatory surgery setting, the issue of patient attire has become controversial. The expectation and goal of ambulatory surgery is to send the patients home the same day as the procedure, usually within hours of their arrival. Therefore, many patients request being able to keep their clothing on for their surgical procedures. Some healthcare experts are concerned about the contamination that may be brought in on patients' clothing or the clothing interfering with care should an emergency arise. No guidelines or studies have been published addressing the issue of appropriate patient attire in the ambulatory surgical setting. In August, 2000, the Statewide Program for Infection Control and Epidemiology (SPICE) sent a questionnaire by email to North Carolina (NC) infection control professionals (ICPs) at the 69 NC hospitals on its electronic mailing list. Infection control professionals at forty-four of the 69 hospitals (64 %) responded to the questionnaire that asked four questions about practices in their ambulatory surgery related to patients wearing their own clothing. These 69 hospitals represent approximately half of the North Carolina facilities that may do outpatient surgery. The results of the survey were as follows. In response to the question, "Is your facility allowing any procedures to be done with patients wearing their own clothing in the operation room (OR) suite?" slightly more than half, 24 of 44 (54%), of the facilities allowed patients to wear some or all of their own clothing in the OR suite for at least one type of procedure. Of those 24 responding affirmatively to that question, ten (42%) facilities allowed patients to wear their clothing for eye or cataract procedures only; six (25%) facilities for eye, ENT and plastics procedures; four (17%) facilities for all procedures; two (8%) facilities for pediatric cases only; and two (8%) facilities for surgery above the waist only. In response to the question "Is your facility allowing any procedures to be done with the patients wearing their own clothing under a cover gown supplied by the facility?" eight (33%) required no gown; 15 (63%) required a gown with no cuffs; and one (4%) facility required a gown with cuffs. As to what clothing facilities allowed patients to wear in the OR, eleven (46%) facilities allowed all clothing; two (8%) allowed all clothing but no shoes; six (25%) allowed underwear and socks only; three (13%) allowed socks only; and two (8%) allowed all clothing below the waist. All facilities replied that no problems had arisen because of patient clothing being worn in the OR, although one facility noted it was difficult to enforce the policy. These results suggest a change from the traditional practice of patients wearing only hospital provided gowns in the surgical suite and should be monitored for infection control issues. FABRIC-COVERED FURNITURE - A RESERVOIR FOR VRE Published studies have reported that vancomycin-resistant enterococci (VRE) can survive on nonporous surfaces for as long as seven days. Recently, researchers at Northwestern Hospital examined survivability and transmissibility of VRE on porous cloth-covered (woven, synthetic fiber) furniture (Am J Infect Control 2000;28:311-3). Cultures were taken from seat cushions in five randomly chosen rooms by specially-made Rodac impression plates. All rooms in this new hospital were private. Three of the five rooms were occupied by patients known to have rectal VRE colonization. The results of the 5 rooms investigated were that VRE was found on 3 of 10 seat cushions (30%) sampled. The investigators also performed simulated inoculation studies using vancomycin-resistant Enterococcus faecium onto the chair's seat cushion. Testing for recovery of VRE was accomplished by using a Rodac plate with a 5-second contact time. The surfaces inoculated included fabric chairs, vinyl chairs and linen (sheet and bath blanket). Of the 5 simulated samples inoculated onto the fabric and vinyl chair cushions, all were positive for growth after inoculations and at 72 hours and 7 days with no cleaning performed. Disinfection with a quaternary ammonium solution was not successful in removing VRE from any of the fabric chairs; however, this routine disinfection removed VRE from all vinyl surfaces. Cushions were positive for VRE after inoculating a sheet or bath blanket covering the seat cushion. However, folding the sheets in quarters or bath blanket in half prevented contamination of the chair surface. To simulate transmission from the seat cushion to a patient or healthcare worker, one area on both the fabric and vinyl chairs was inoculated with VRE, then touched 5 minutes later with the palmar surface of the hand, then to a Rodac plate. Hands of healthcare workers cultured after contact with contaminated cushions (fabric or vinyl) were positive for VRE. These results demonstrate that porous surfaces cannot be disinfected for VRE and may serve as a reservoir where VRE could transfer to hands. The authors recommended the selection of non-porous fabrics that are easily cleaned in health care institutions. QUESTION OF THE MONTH Q: What should be done if banked breast milk is given to the wrong baby in the nursery? Is this an exposure? A: No guidelines exist specifically for the post-exposure management of infants accidentally exposed by ingestion of breast milk. However, situations in which human milk is collected from unrelated donors for infant feeding has prompted the development of guidelines for appropriate selection and screening of donors as well as practices for careful collection, processing, and storage of the breast milk. Currently, U.S. donor milk banks that belong to the Human Milk Banking Association of North America voluntarily follow guidelines drafted in consultation with the U.S. Food and Drug Administration and the Centers for Disease Control and Prevention. These guidelines summarized in the Pediatric Red Book include screening donors for antibodies to HIV-1, HIV-2, HTLV-I, HTLV-II, HBsAg, hepatitis C, and syphilis. The Statewide Program for Infection Control and Epidemiology (SPICE) recommends that it would be prudent to follow these guidelines for the postexposure testing of the source of the human milk, with the exception of syphilis, as long as these results were already available from the prenatal screening. Also, SPICE suggests that the source should be tested for HSV if lesions are present on the donor breast. Of course, a policy that is enforced to rectify the situation from occurring again is paramount. UNC Healthcare has a protocol that allows only the nurse assigned to the baby to prepare (i.e., thaw) and deliver the milk to the baby after carefully cross-checking the infant identification bracelet number to the milk identification number. NEWS AND ANNOUNCEMENTS Dr. Julie Gerberding, Director of the Hospital Infections Program (HIP), CDC, announced that HIP has changed its name to the Division of Healthcare Quality Promotion and Infection Prevention (DHQPIP). The North Carolina Tuberculosis Policy Manual, 8th Edition, 1999, was modified 11/01/00 to reflect new CDC recommendations and is available on the internet at http://tbnc.mc.duke.edu/manual.htm These revisions incorporate updated information since the 1995 publication. A new Chapter V-A. HIV/AIDS has been added to emphasize the unique considerations necessary for the management of HIV-positive individuals with tuberculosis infection and/or disease. For additional information about changes, see Report of the Month, Volume IV, Number 4, July-August 2000. http://www.unc.edu/depts/spice/rep-iv-4.html The Occupational Safety and Health Administration (OSHA) "Ergonomics Program; Final Rule" was published in the Federal Register on November 14, 2000. It is available online at http://www.osha-slc.gov/ergonomics-standard/index.html COURSES FOR THE INFECTION CONTROL PROFESSIONAL "Infection Control Part I: Clinical Surveillance of Nosocomial Infections will be held in Chapel Hill in the spring of 2001. "Infection Control in Long-Term Care" will be held in Chapel Hill in the spring of 2001. HOLIDAY FUN GRINCHY GERMS IN HEELVILLE All the Heels down in Heelville loved Christmas for a reason And it wasn‘t just because it was basketball season. They loved the trimmings, the trappings, and friends so dear But little did they think of the many grinches near! These grinches are tiny, not big, not tall and They even don ‘t live near Mt. Crumpet at all. They come in small sizes, in groups and in pairs And they live in Heel homes and even Heel hair! They can hide in their food and their Christmas tree Oh these little devils are so hard to see! These germs need no season or even a reason To make a Heel cough or start a Heel sneezin'. Their gifts are so grinchy especially the flu Making every Tarheel in Heelville cry “Boo Hoo"! What can we do, what can we say So these germs won ‘t steal our Heel Christmas Day?! Why, wash your hands and get some sleep And in a cold refrigerator your feast will keep. A flu shot will do and lots of fresh air And pass out those hankies, a few germs they can snare. Then greet your friends and sing by the tree And when you toast just remember your Vitamin C!!! Written by Vickie Brown, an ICP in Chapel Hill (home of the University of North Carolina Tar Heel teams), North Carolina (the Tar Heel state). -----------------------------------------------------------------------------------------------------------------Contributors to Report of the Month: Karen K. Hoffmann, RN, MS, CIC; William A. Rutala, PhD, MPH; David J. Weber, MD, MPH; Eva P. Clontz, MEd. -----------------------------------------------------------------------------------------------------------------To subscribe to the Report of the Month, send email to spice@unc.edu Report of the Month is also available on the home page of the Statewide Program for Infection Control and Epidemiology at http://www.unc.edu/depts/spice/ The Statewide Program for Infection Control and Epidemiology (SPICE) is funded by the General Assembly of North Carolina to serve the State. SPICE is not a regulatory agency but provides education and consultation to North Carolina healthcare facilities. Copyright 2000 Statewide Program for Infection Control and Epidemiology