Neuroscience 5b – Nociception
advertisement

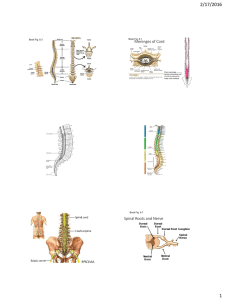
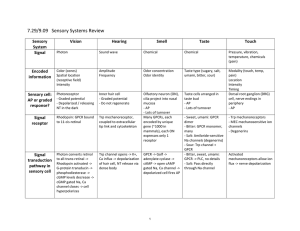
Neuroscience 5b – Nociception Anil Chopra Nociception is the ability to detect overt or impending tissue damage. It is different from pain in that pain is an experience that may arise from nociception or in the absence of nociception. It is sensed by nociceptors. A nociceptive stimulus can be measured. Conduction Speed: as a general rule, larger axon diameters and myelination of axons results in an increase in conduction velocity. The nociceptors are all slow adapting nerve endings that are sensitive to mechanical deformation, excessive heat and various chemicals that are released by damaged cells such as transmitters, bradykinin, histamine, cytokines e.t.c. These all cause depolarisation at nerve terminals on skin, muscles and visceral organs and result in the sensation of pain. This generally has a high threshold. Sensory Neurons Cell bodies are in the PNS (Doral root ganglion or trigeminal ganglia) 2 axon types:- 1) Aδ mechano or thermoreceptor, faster, produces sharp pain, leads to avoidance. 2) C fibres, chemoreceptor, e.g. Bradykinin or histamine, produces a dull aching pain, leads to guarding to allow recovery Receptive fields are normally large Intensity is coded by the frequency of firing Receptors feed into the spinothalamic system Pathway Perception of pain and temperature also consists of 3 neurones: (1) From the limb/organ/dermatome it has its cell body in the dorsal root ganglion. From the dorsal root ganglion, it passes into the spinal cord via the dorsal horn and synapses again in the grey matter of the spinal cord. At the pons, the spinothalamic tract becomes the spinal leminiscus and attaches itself to the medial leminiscus. (2) From here it passes through the spinal cord anterolaterally (opposite side) and travels up to the thalamus along the Spinothalamic tract up to synapse in the thalamus. Input from the face also from trigeminal nerve (V) and trigeminal nerve ganglion. (3) From the thalamus it then terminates in the appropriate section of the primary somatosensory cortex. NB: Organised somatotopically Parts of the Brain which Process Nociceptive Information The spinothalamic tract carries information to several destinations in the brain: o To the VPL and VPM nuclei of the thalamus and then onto SI and SII in the cortex, for analysis of localisation and intensity of the stimulus o To the reticular formation of the brainstem and the intralaminar nuclei of the thalamus to signal the unpleasantness of the stimulus and give the emotional component of pain – the affective pathway o To the periaqueductal grey of the midbrain – the central inhibition pathway o Both of these connections from the cortex are via collateral synapses The sensation of pain is emotionally neutral until it does down one of the collateral branches, it is then perceived emotionally as pain The affective or secondary pain pathway is shown on the right The dotted line arrow shows it going on to SI and the thalamus, the collateral branch to the cingulated cortex is part of the limbic system – giving emotion and fitting in with the function of the limbic system As can be seen the collateral branches come of the spinothalamic tract before the signal reaches the thalamus or cortex Reticular Formation If all the tracts and nuclei of the brainstem are identified, anything left is known as the reticular formation. Central Inhibition This is a process by which the feeling of pain can be suppressed. Electrical stimulation from the periaqueductal grey matter travel down via the nuclei of the reticular formation to the dorsal horn of the spinal cord and cause inhibition of action potential firing at nociceptors. The pathway uses endogenous opioids and strong inputs from hypothalamus and cerebral cortex. Peripheral Inhibition Peripheral inhibition is the sensation of analgesia when pain is rubbed. Because mechanoreceptors have a low-threshold and pain receptors have a high threshold, when the mechanoreceptors fire action potential, they inhibit the pain receptors around them by lateral inhibition. This has an analgesic effect. It takes place at the superficial levels of the dorsal horn (substantis gelatinosa) and is also known as the gate theory. Secondary Pain Pathway: • STT projects to cerebral cortex via reticular formation and intralaminar nuclei • Triggers arousal • Signals unpleasantness of the stimulus • Registers awareness of pain at thalamic level Nociceptive Dysfunction • Disruption of pathway – loss of pain E.g. syringomyelia, Charcot joints • Exacerbation of pain – hyperalgesia E.g. thalamic syndrome, windup in dorsal horn




![Major Change to a Course or Pathway [DOCX 31.06KB]](http://s3.studylib.net/store/data/006879957_1-7d46b1f6b93d0bf5c854352080131369-300x300.png)