Review of Renal Anatomy and Histology with Introduction to Renal

Review of Renal Anatomy and Histology with Introduction to Renal Pathology (Robbins pp. 931-936)
Renal anatomy
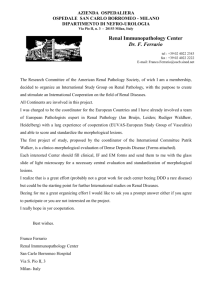
Renal Histology Distribution of glomerular damage
CL – capillary lumen
MES – mesangium
END – endothelium
EP – visceral epithelial cells w/ foot processes
Pattern of glomerular injury
Injury Presentation Description capillary wall alterations proteinuria
GBM alterations proliferation proteinuria (permeable to albumin) hematuria may be thickened due to immune complexes may be thickened due to accumulation of structural proteins
in cells either intrinsic (e.g., mesangial cells) or extrinsic (e.g., e.g., inflammatory), may have deposits necrotizing cellular crescents fibrocellular crescent fibrous crescent dysmorphic rbcs w/ rbc casts in urine, acute renal failure clinically “RPGN” necrosis usually w/ disruption of capillary wall & fibrinoid change defn – 2 cellular layers occupying min 1/3 of circumference
in cells in Bowman’s space (parietal epithelial cells & m
), often see fibrin, if >80% glomeruli w/ crescents
“crescentic GN” same as above but w/ fibrosis fibrous scar which may or may not have arisen from cellular/fibrocellular crescents hyalinosis sclerosis proteinuria acellular, structureless material located in capillary lumen consisting of glycoproteins & sometimes lipids
in mesangial matrix or fibrosis w/ glomerular collapse or occlusion
glomerular scar; possible final pathway
IF patterns
granular – due to discrete deposits of immune complexes, best seen on capillary loops
linear – smooth, global staining of GBM
mesangial – w/in mesangial matrix
EM patterns
epithelial cell injury – effacement of foot processes and microvillous transformation subepithelial deposits – btw epithelial cells and GBM
subendothelial deposits – btw endothelial cells and GBM
mesangial matrix deposits – in mesangium
Immune complex deposition
In situ deposition
antibodies to GBM deposit on GBM itself (linear IF pattern) (e.g., anti-GBM GN)
antibodies to intrinsic glomerular antigens (granular IF pattern) (e.g., Heymann’s nephritis, , membranous GN)
nonglomerular antigens bind to GBM, antibodies bind to planted antigen
Circulating immune complex deposition
complexes trapped in glomerular filter
incite inflammatory response
Progression of renal injury
end stage renal disease
compensatory hypertrophy,
glomerular pressure, systemic HTN
Clinical manifestations of renal disease
acute nephritic syndrome – hematuria, mild to moderate proteinuria, HTN nephrotic syndrome – heavy proteinuria (> 3.5 g/d), hypoalbuminemia, severe edema, hyperlipidemia, lipiduria
asymptomatic hematuria or proteinuria – subtle/mild glomerular abnormalities
acute renal failure – oliguria or anuria, recent onset of azotemia
chronic renal failure – prolonged symptoms and signs of uremia
renal tubular defects – polyuria, nocturia, electrolyte disorders
urinary tract infection – bacteriuria, pyuria
nephrolithiasis (renal stones) – renal colic, hematuria, recurrent stone formation
urinary tract obstruction and renal tumors – varied manifestations
Renal failure
diminished renal reserve – GFR 50% of normal, serum BUN and Cr values normal, pts asymptomatic
renal insufficiency – GFR 20% to 50% of normal, azotemia appears, anemia, HTN, polyuria, nocturia
renal failure – GFR less than 20% to 25% of normal, edema, metabolic acidosis, hypocalcemia, overt uremia
end-stage renal disease – GFR less than 5%, end stage of uremia
Medical Renal Disease (Robbins pp. 942-968)
Nephrotic Syndrome – proteinuria > 3.5 g/d, hypoalbumenia (< 3.5 g/dL), edema, hyperlipidemia/hypercholesterolemia, little or no hematuria
Disease
Minimal Change Dz
(Lipoid Nephrosis, Nil
Dz)
Focal & Segmental GN
(Focal Sclerosis, FSGS)
Membranous
Nephropathy
Diabetic Nephropathy
Amyloid
Epi
children
(most)
also adults
freq in adults
African
adults
leading
uncommon in children
Americans cause of nephrotic syndrome adults 10-20 yrs after onset of diabetes adults w/ multiple myeloma
familial in others
Path
cause: unknown
LM: nl glomeruli, lipids in tubular cells
IF: no staining
EM: diffuse effacement of epi foot processes, microvillous transformation of epi cell
protein & lipid in prox tubule
cause: 1 o (idiopathic)/2 o (HIV, morbid obesity,
renal mass)
LM: segmental sclerosis (
mesangial matrix), hyalinosis, atrophy of prox tubule
IF: passive trapping of IgM, C3
EM: diffuse effacement of epi foot processes, separation of epi cells from GBM (vacuolization), cell swelling, proliferation
mech includes circulating factor, hemodynamic injury, glom hypertrophy, hyperlipidemia, 1 o injury or dysfxn of glom cells
cause: 1 o (idiopathic)/2 o (HBV, SLE, gold therapy); immune-complex mediated
LM: uniform thickening of the GBM on H&E or PAS stains, silver stain will see spikes
IF: granular capillary-loop of IgG, C3
EM: subepi electron dense deposits (spikes = GBM rxn to deposits), effacement of epi foot processes, microvillous transformation
little glom cell prolif or inflam exudate
cause: poor metabolic control, hyperfiltration, genetic factors, HTN
LM: marked uniform thickening of GBM &
of mesangial matrix w/o
cells, periph spherical accumulations (Kimmelstiel-Wilson nodules), hyaline arteriosclerosis (aff and eff arterioles)
IF: linear Ig, albumin
EM: homogenous thickened GBM w/o deposits
cause: deposition of light chains, chronic infxns, chronic dialysis, familial
LM: amorphous pink material in all 4 compartments, stains positively w/ Congo red & shows circular dichroism under polarized light
IF: kappa or lambda chains
EM: microfibrils
manifestation of plasma cell dyscrasias
Clinical/Rx
nephrotic syndrome, but nl renal fx
diagnosis of exclusion
rx w/ steroids, sometimes spontaneous remission
nephrotic syndrome, renal insufficiency,
HTN, hematuria
can progress to renal failure
recurs in transplants at relatively high freq
rx w/ steroids somewhat helpful
chronic GN can occur
rx w/ steroids,
lower extremity edema, mild renal insufficiency sometimes spontaneous remission, sometimes nothing works microalbuminuria progressing to nephropathy (nephrotic syndrome & mild renal insufficiency)
rx w/ good metabolic &
HTN control (slow progression)
no rx
Nephritic Syndrome – inflamm damages glom capillaries
hematuria (rbc casts/smoky, brown urine), oliguria, azotemia, HTN, mild proteinuria, mild edema
Disease
IgA Nephropathy
(Berger’s Dz)
Post Infectious GN
(Post Strep GN)
Lupus Nephritis (LN)
Membranoproliferative
GN (MPGN)
Type I
Type II – Dense
Deposit Dz (DDD)
Epi
young adults
> in males
Asia, W.
Eur,
Mexico
women
renal dz
common in children young imp cause of morbidity, death in
SLE older children & young adults relatively rare
Path
cause: unknown;
synthesis of IgA by gut, errors of IgA processing by liver
LM: mild to moderate diffuse proliferation of mesangial cells & matrix, cellular crescents rare
IF: granular IgA deposits in mesangium
EM: mesangial electron dense deposits, focal or no foot process effacement
cause: serum sickness (Ag-Ab complexes
trapped in
glom
accumulate & stimulate C’
inflamm
LM:
in mesangial cells & varying numbers of inflamm cells (PMNs) w/ endo cell swelling, cellular crescents, inflamm & edema in interstitium
IF: diffuse granular IgG, C3 (IgA, IgM) around cap loops
EM: electron dense material
“humps” subepi
strep common; also staph, pneumo, others
cause: SLE (autoimmune immune complexes)
LM/EM:
normal glomeruli
mesangial proliferative (nl/
cells) – LM shows
matrix, EM shows mesangial deposits focal proliferative – segmental
cells < 50%, EM shows deposits in mesangium, subendo space
diffuse proliferative – same as above, but > 50%
membranous – spikes, subepi deposits, mesangial deposits
IF: full house mesangial or cap, IgG, IgA, IgM, C3, C1q
EM: tubuloreticular inclusions in endo cells
cause: complement, 2 o causes (Hep C)
LM: diffuse global thickening of capillary loops accompanied by
numbers of mesangial cells & accumulation of mesangial matrix, double contours on silver stain (GBM split)
IF: granular C’ (C3) in mesangium, periph cap loops
EM: Type I – excess matrix containing deposits, mesangial cells extend to subendo space, subendo deposits, endo cells make GBM
double contours, foot process effacement,
Clinical/Rx
viral illness 1-2 d before
recurrent microscopic or gross hematuria & proteinuria
slowly prog HTN & renal insuff
20% lose renal fxn
no rx, but usually no sequelae
rx w/ steroids, other immunosuppressive type II worse prognosis
Anti-GBM Dz
(Goodpasture’s Dz)
GBM Dz:
Alport’s Hereditary
Nephritis (AHN)
GBM Dz:
Thin Basement
Membrane Disorder
2
> in young men, but at any age nd peak in elderly females mild
males CRF by 40 children & adults
familial microvillous transformation
EM: Type II – massive, very electron dense deposits in lamina densa of capillary GBM, GBM appears scalloped
cause: circulating IgG Ab
interacts w/ Goodpasture’s Ag
(subunits of NC1 domain of collagen IV), viral infxn, smoking, hydrocarbons
LM: crescentic GN
IF: linear IgG, C3 in GBM
EM: collapse of cap loops, frag of GBM, no GBM deposits
cause: lack Goodpasture’s Ag -
mech fragility & breakage of GBM
micro/macro hematuria; COL4A5 gene
LM: early nl, later focal sclerosis or proliferative GN, foam cells (glomeruli, interstitium)
IF: no staining
EM: (diagnosis) – segmental thickening & splitting of
GBM
layered, other segments show marked thinning
cause: unknown
LM/IF: unremarkable
EM: marked thinning of GBM
pulmonary hemorrhage followed by ARF rx w/ steroids, cytotoxic drugs, plasmaphoresis penetrance important deficits in hearing, mental retardation, platelet abnormalities
renal transplants for
AHN pts
anti-GBM nephritis
no rx
Nephrotic Syndromes
Minimal Change Disease FSGS
LM: looks normal
EM: foot effacement and microvillous transformation
LM: focal
Membranous Nephropathy
LM: segmental
LM: spikes on silver stain
LM: cellularity normal, thickened capillary loops
IF: granular, IgG, C3 EM: subepi deposits
Nephritic Syndromes
IgA nephropathy
LM: mesangial cellularity
Post Strep GN
LM: hypercellularity (epi, endo, mesan, PMNs), poorly defined capillary loops
IF: mesangial, IgA
No image available
EM: mesangial electron dense deposits, focal or no foot process effacement
IF: diffuse, granular, bumpy, IgG, C3, (IgA, IgM)
EM: subepithelial “humps”
A B
Goodpasture’s Disease
Membranoproliferative
GN (MPGN) on silver staining or
PAS staining, will see double contours of split
GBM
A = Type I subendo deposits in mesangium
B = Type II dense deposits in lamina densa, notice
“scalloped look”
Crescents
Crescentic GN caused by SLE (lupus nephritis)
IF: linear, IgG, C3
RPGN may idiopathic or caused by SLE, PSGN, vasculitis, Goodpasture’s
LM: crescent
LM: capillary wire loops seen in SLE
Male Reproductive System (Robbins pp. 1011-1034)
Prostate
Inflammations
acute bacterial prostatitis – minute, dissemin’ abscesses; large necrotic areas; or diffuse edema, congestion, suppuration
chronic prostatitis – aggregation of lymphocytes, plasma cells, macrophages, PMNs
Benign Prostatic Hypertrophy (Hyperplasia)
epidemiology
common in men over 50
w/ age (90% in 8 th decade)
pathology/pathogenesis
large hyperplastic nodules in central, periurethral region of prostate
composed of glandular & stromal proliferation
may be caused by testosterone (DHT) or advancing age
clinical
arise when nodules compress and narrow urethra
dysuria
usually no rx, but 5-10% need surgery if serious urinary tract obstruction
finasteride (anti-androgen) somewhat helpful
Carcinoma
epidemiology
3 rd leading CA death in men (11% of CA deaths)
w/ age (peak in 8 th decade)
Af-Am > Caucasians > Asians
occult CA common (9/10 remain undetected & clinically unimportant)
pathology/pathogenesis
most lesions adenocarcinoma (back-to-back acini w/ little stroma), in peripheral zone of gland
gritty and firm tissue, felt best by palpation
prostatic intraepithelial neoplasia (PIN) may be precursor to frank carcinoma (many of the same features)
Gleason grade
1 = well-differentiated (small to medium glands closely spaced)
3 = moderately differentiated (cribiform patterns)
5 = poorly differentiated (cords, nests, solid sheets, individual cells w/ anaplastic features)
Gleason score
sum Gleason grades from 2 most prevalent types
score < 4 = well differentiated, rx is conservative
score > 5 = moderately to poorly differentiated, rx is aggressive
Staging – spread occurs by direct local invasion, lymphogenous spread, or hematogenous spread a occult or clinically unsuspected b palpable by rectal, but confined to prostate c local extension beyond prostate (seminal vesicles, bladder, lymph nodes) d metastases
clinical
PSA = 4-10 (stage a/b)
localized prostate CA; PSA > 10 (stage c/d)
invasive/metastatic prostate CA
virtually diagnostic if find osteoblastic metastases in bone
rx w/ orchiectomy, radiation, or estrogen therapy
Testes
Cryptorchidism
epidemiology – 0.3-0.8% of males, unilateral 75%, bilateral 25%
pathology – congenital anomaly characterized by incomplete descent of one or both testes into scrotal sac
clinical
sequelae – 1.) infertility (
in interstitial stroma, Leydig cell hyperplasia), 2.) 10x-40x
risk of testicular CA
rx w/ orchiopexy (surgical repositioning) at around 2 yrs of age
Torsion
twisting of spermatic cord resulting in altered blood supply
hemorrhage/infarction
requires emergency surgery
Atrophy
due to atherosclerosis, end stage inflamm orchitis, cryptorchidism, hypopituitarism, malnutrition/cachexia, obstruction to semen outflow, irradiation, estrogen rx to prostate CA, Klinefelter’s syndrome (XXY)
Inflammation
epididymitis > orchitis
in children, epididymitis associated w/ congenital genitourinary abnormalities
in sexually active men, epididymitis associated w/ Chlamydia trachomatis & Neisseria gonorrhoeae infxn
syphilis first affects the testis
mumps orchitis unilateral & self-heals
Tumors
Germ Cell Tumors (95% of testicular CA)
factors 1.) cryptorchidism, 2.) genetics, 3.) testicular dysgenesis
Seminoma (30% of germ cell tumors)
typical variant (85% of seminomas)
sheets of uniform cells w/ infiltration of septa by lymphocytes
large individual cells, well-defined membranes, clear cytoplasm, large nuclei, prominent nucleoli
anaplastic variant (5-10% of seminomas)
greater cellularity, nuclear irregularity
spermatocytic variant (4-6% of seminomas)
slow growing that affects men > 65, does not metastasize, excellent prognosis
not seen in children
chemo and radiotherapy works for pure seminomas
most AFP & HCG negative, but may see PLAP on tissue by immunoperoxidase staining
Embryonal carcinoma (3% of germ cell tumors in pure form, 45% of germ cell tumors in mixed form)
has glandular, alveolar, tubular, or sheet-like growth patterns
individual cells have indistinct borders, marked variation in cell and nuclear size and shape
see AFP on immunoperoxidase staining or in serum
Yolk sac tumor (infantile embryonal carcinoma, endodermal sinus tumor)
most common in infants and children
contain AFP
Choriocarcinoma
highly malignant arising from placenta, ovary, or totipotential cells in mediastinum or abdomen
contains 2 cell types
syncytiotrophoblast – large, multinucleate, contains HCG
cytotrophoblast – regular, polygonal cells w/ distinct cell borders
Teratoma
derivatives from more than one germ layer (ectoderm, mesoderm, endoderm)
ectodermal only (skin, hair, sebaceous glands) – cystic, filled w/ sebaceous material & hair (dermoid cysts)
benign (collection of mature tissue) usually occur in children
malignant (contain embryonic tissue) usually occur in adults – lack of malignant cytologic features
when contains areas of adenocarcinoma, squamous carcinoma, sarcoma
“teratoma w/ malignant transformation”
Mixed tumors
60% of testicular cancer is mixed
most common mixture (14%) is teratoma, embryonal carcinoma, yolk sac tumor, choriocarcinoma
if seminoma part of MCGT (mixed cell germ cell tumor), then prognosis better than NS-MGCT (nonseminomatous mixed cell germ cell tumor)
Staging
Stage I – tumor confined to the testis
Stage II – tumor confined to the retroperitoneal nodes below the diaphragm
Stage III – tumor outside the retroperitoneal nodes above the diaphragm
Sex Cord-Gonadal Stromal Tumors (4-6% of testicular CA)
Leydig cell tumors
epi – 2% of testicular CA
path – cell cytoplasm may contain lipid granules, vacuoles, lipochrome pigment & characteristic rodshaped crystalloids of Reinke, most benign
clinical – boys
precocious puberty; men
nothing or gynecomastia
Sertoli cell tumors (androblastoma) – most benign, freq in cryptorchid testes
Germ Cell Tumors
Seminoma showing poorly demarcated lobules and clear cells
Embryonal carcinoma showing sheets of undifferentiated cells and glandular elements
Choriocarcinoma w/ clear cytotrophoblastic cells w/ central nuclei and syncytiotrophoblastic cells w/ multiple dark nuclei
Neoplastic Disease of the Urinary Tract (Robbins pp. 991-994, 999, 1003-1008)
Neoplasms of the Urothelium normal histology – 5-7 layers thick (>7 abnl), lined by superficial “umbrella” cells (w/ asymmetric unit membrane)
Epithelial Tumors of the Bladder
classification – based on pattern of growth, cell type, cytologic abnormalities, papillary vs. non-papillary, carcinoma-in-situ
etiologic agents
cigarette smoking is the most important factor
industrial chemicals –
-naphthylamine & biphenyl compounds (both in dyes of textiles, paints, plastics, rubber, cable)
environmental exposure – artificial sweeteners, Schistosoma may cause squamous bladder tumors
genetic – chromosome 9 deletions (also 17 and 14)
grading – based on epithelium thickness, mitosis, polarity, presence of umbrella cells, nuclear chromatin abnormalities
Grade 0 –
Grade I – urothelial papilloma urothelial neoplasm, low malignant potential
100% 5-yr survival
>90% 5-yr survival
Grade II –
Grade III –
staging urothelial carcinoma, low grade urothelial carcinoma, high grade
>50% 5-yr survival
<10% 5-yr survival
Depth of Invasion Stage 5-yr survival
Noninvasive, papillary Ta 80%
Noninvasive, flat
Lamina propria
Superficial muscularis propria
TIS
T1
T2
40%
Deep muscularis propria
Perivesical fat
T3a
T3b 20%
Adjacent structures T4
Lymph node metastases (<2 cm) N1 6%
Lymph node metastases (2-5 cm) N2
Lymph node metastases (>5 cm) N3
Distant metastases M1
subclassification
papillary carcinoma (90% of all 1 o bladder tumors, will often recur in Grades I,II,III)
clinical – males:females (3:1), older pts (6 th -7 th decade), painless gross or microscopic hematuria, frequency, urgency, dysuria, pyelonephritis, hydronephrosis
gross – looks like red sea anemone, found in trigone & lateral walls, w/ narrow or broad stalk
microscopic – well differentiated have delicate fronds while poorly differentiated may have invasion
non-papillary (invasive, high grade)
clinical – past hx of papillary neoplasia
gross – flat, ulcerated, bulky lesions anywhere in bladder
microscopic – high grade, squamous or glandular
sessile carcinoma-in-situ (may give rise to non-papillary, may be near papillary CA, 4% of all bladder CA)
clinical – 60% progress to invasive
gross – red, velvety patch
microscopic – full thickness mucosal involvement by undifferentiated cells, no invasion
metastases – to regional lymph nodes then to liver and lungs
prognosis – 90% recurrence rate, see grading and staging section
treatment – local/radical surgery, local chemo/radiation
special studies/techniques
Ag – ABH, Lewis A & B on normal, but Lewis X & T on neoplastic
morphometry – quantify shape, abnormalities
DNA ploidy – diploid tumors better prognosis than aneuploid
chromosomal structure – none
genes/products – overexpression of ras family & mutations of p53 & Rb
cell kinetics – use Ab
Primary Neoplasms of the Kidney
Tumor
Epidemiology
Clinical
Gross features
Histopathology
Nephroblastoma
(Wilm’s Tumor)
peak during 2 yoa, 50% dx by 3 yoa, 75% dx by 5 yoa
no sex, geographical, or racial difference
tends to be familial (chromosome 11 abnormalities)
assc’ w/ sporadic aniridia, hemihypertrophy, Beckwith-
Wiedemann syndrome (macroglossia, omphalocele, gigantism, adrenal cytomegaly, visceromegaly)
abd mass (90%)
HTN, abd pain, anorexia, nausea, vomiting, fever, constipation, gross hematuria
mets in 25% of presentations
calcification rare
erythropoietin levels
related to congenital mesoblastic nephroma & solitary multilocular cysts of kidney
usually unilateral (5.8% bilateral)
large (mean 12 cm, 540 g)
on section, soft, gray-tan, bulging
National Wilms’ Study Group
Group I – limited to kidney
Group II – beyond kidney, but totally removed
Group III – beyond kidney & tumor remains
Group IV – hematogenous spread
may have epithelial, stromal, blastematous
tubular/glandular differentiation
better prognosis
Pathogenesis
persistent nodules of metanephric blastema (periphery of renal lobules & beneath capsule)
Renal Adenocarcinoma
(Hypernephroma, Grawitz Tumor)
6 mths to old age (peak in 6 th decade), adults
males:females (3:1)
pts w/ Von Hippel-Lindau dz (phakomatosis)
nonpapillary
chromosome 3 deletions/ translocations
papillary
show trisomies
painless, gross or microscopic hematuria
pain, renal mass, pyrexia, wt loss, fatigue, GI
& NM complaints
erythrocytosis (sometimes
erythropoietin)
anemia (normochromic, normocytic)
hypercalcemia (make parthormone)
amyloidosis (incidental)
dx w/ x-ray, radioisotopic scan, CT, US, FNA
both sides involved, bilateral 1-2%
<3 cm or >10 cm
protrudes from cortical surface as yellow to gray mass
bulging lobulated appearance
tumor gray-yellow w/ hemorrhage, necrosis
pseudocapsule many times
papillary, cystic, sarcomatoid, tubular
columnar/cuboidal in tubular/glandular pattern
pleomorphism modest
cytoplasm pale to eosinophilic
highly vascular, w/ glycogen, lipid
similar to prox convoluted tubules (both have tightly packed microvilli)
causes include hydrocarbons, aromatic amines
& amides, aliphatic compounds, aflatoxins, lead compounds, obesity, unopposed estrogen
strong association w/ tobacco use
at dx, 95% w/ mets
mets to lungs, lymph nodes, liver, bone, skin
Progression/Mets
local extension, but usually spread via vessels,
Treatment
Prognosis lymphatics
mets to lungs, liver, mediastinum (to bone rare)
mets w/in 2 yrs of dx
combined chemo, surgery, radiation
younger pts (<2 yrs) do best
current rx has led to
mortality in men
pts w/ large tumors (>550 g) do poorly
stage
mortality
surgery
poor, 18-27% 10-yr survival
staging
Stage I – confined to kidney
Stage II – invasion of perinephric fat
Stage III – regional nodes to vena cava
Stage IV – adjacent/distal organs
Causes of Hematuria
Hematologic
Coagulopathy
Hemoglobulinopathy
Renal
Glomerular vs. nonglomerular
Infection
Malformation
Ischemia
Trauma
Hypersensitivity
Post-Renal
Calculi
Mechanical
Inflammatory
Neoplasm
BPH
Exercise
False
Vaginal bleeding
Pigmenturia factitious
Epithelial Tumors of the Bladder
Normal bladder mucosa Grade I (low malignant potential)
Grade II (low grade)
Renal Adenocarcinoma (Renal Cell Carcinoma)
Grade III (high grade)
A: clear cell type sporadic/hereditary – translocations 3;6, 3;8, 3;11, deletions on chromosome 3, Loss of VHL, inactivated/mutated VHL, hypermethylation of VHL
B: papillary type sporadic – trisomy 7, 16, 17, loss of Y, mutated/activated MET, t(X;1)
PRCC oncogenes hereditary – trisomy 7, mutated/activated MET
C: chromophobe type excellent prognosis
Wilm’s Tumor
Gross: tan gray color, well-circumscribed margins
Microscopic: triphasic histology
stromal (less cellular on left)
epithelial (clear tubule in center)
blastemic (tightly packed blue cells on right)
Tubulointerstitial and Vascular Diseases of the Kidney (Robbins pp. 968-990)
Tubulointerstitial Diseases
Acute Tubular Necrosis (ATN)
Types
Ischemic ATN
etiology – shock, transfusion, hemorrhage, crush injuries, sepsis
hypoTN,
renal perfusion
tubular injury
path – dilatation of tubules, single cell necrosis w/ skip areas, casts (hyaline or pigmented), interstitial edema, regenerating epi cells (after 3-5 d), mononuclear cells in vasa recta
Nephrotoxic ATN
etiology
drugs – antibiotics (gentamicin), contrast media, antineoplastic (cisplatin)
chemicals – heavy metals (HgCl
2
, lead-see nuclear inclusions), organic solvents (CCl
4
, diethylene glycolsee oxalate deposition), poisons (herbicide)
pigments – hemoglobin, myoglobin
path – similar to ischemic (dilated tubules, interstitial edema, regenerating epi cells), but also w/ extensive epi necrosis affecting greater portion of tubule
Mechanism ischemia or nephrotoxins tubular damage ( epithelial injury/necrosis ) vasoconstriction obstruction by casts tubular back leak pathogenesis:
tubule cell injury
disturbances in blood flow
intratubular pressure
( dilated tubules )
tubular flow interstitial edema
?direct glomerular effect
GFR oliguria
Clinical presentation
rapid onset of oliguria or anuria w/ proportionate rise in serum Cr and BUN
urinary sediment – granular, hyaline, pigmented casts
pts recover w/ proper support if etiology is found & corrected
Interstitial Nephritis (IN) must show interstitial inflammatory infiltrate & tubular epithelial injury
Acute Hypersensitivity IN – immune-mediated injury
etiology – drugs, esp synthetic penicillins (methicillin), diuretics (thiazides), NSAIDS (ibuprofen)
path – inflamm infiltrate in interstitium comprising mononuclear cells, eos, PMNs; interstitial edema, tubular injury
clinical – ARF w/ eos in urinary sediment, occurs w/in 2 wks of new drug, fever, eosinophilia, pyuria, skin rash
Pyelonephritis – infectious etiology
acute pyelonephritis
etiology – E. coli, Proteus, Klebsiella, Staph
pathogenesis – ascending infxn associated w/ urinary obstruction, vesicoureteric reflux, intrarenal reflux, catheterization, pregnancy, sexual activity, diabetes, neurologic deficits
pathology
gross – yellow streaks (pus) from pelvis to cortex
micro – shows inflamm infiltrate w/in tubular lumens & interstitium, interstitial edema, hematogenous infxn w/ small abscesses in cortex
chronic pyelonephritis & reflux nephropathy
etiology – chronic obstruction and/or reflux frequently associated w/ recurrent UTIs
pathology
gross – hydronephrosis, parenchymal atrophy, discrete cortical scar overlying damaged calyx most often at upper or lower pole
micro – tubular atrophy, thyroidization, chronic interstitial inflamm & fibrosis, periglomerular fibrosis
Chronic IN – tubular atrophy & loss accompanied by chronic interstitial inflamm & fibrosis
analgesic nephropathy
etiology – phenacetin, NSAIDs [inhibition of PG synthesis
vasconstriction & ischemia]
path – bland renal papillary necrosis w/ overlying cortical atrophy
metabolic disturbances
urate nephropathy (gout) & nephrocalcinosis
Hereditary Tubular Disease
adult – autosomal dominant polycystic kidney dz
infantile – autosomal recessive polycystic kidney dz
Vascular Disease
Hypertension
benign – intimal thickening in larger arteries, hyaline arteriosclerosis, glomeruli collapsed, tubules atrophied
malignant – fibrinoid necrosis in arterioles & onion skinning in medium sized arteries
Thrombotic Microangiopathy
etiology – endothelial injury
local intravascular coagulation
associated conditions – malignant HTN, hemolytic uremic syndrome, thrombotic thrombocytopenic purpura, scleroderma, pregnancy/delivery, drugs (cyclosporin, mitomycin C)
path – intimal thickening, edema w/ marked narrowing of lumen; fibrin thrombi; erythrocyte fragmentation; fibrinoid necrosis; associated glomerular changes
Vasculitis
hypersensitivity vasculitis, Wegener’s granulomatosis
Arterionephrosclerosis & Atheroembolic Renal Disease
etiology – consequences of atherosclerosis
path – result of chronic ischemia, glomerulosclerosis, tubular atrophy, interstitial fibrosis, intimal thickening, atheroemboli from aortic atherosclerotic plaques
Renal Transplantation
intimal vasculitis – w/ or w/o necrosis of vascular walls
intimal thickening w/ encroachment on lumen, ischemia of renal parenchyma, loss of renal fxn
tubulitis w/ interstitial inflammation
destruction of tubular epithelial cells results in destruction
Hyperacute Rejection
timing – minutes to days
etiology – preformed circulating Ab arising from previous blood transfusions
path – massive vascular thrombosis & renal infarction
Acute Rejection
timing – days to months or on abrupt cessation of immunosuppressive regimen
etiology – predominantly cell-mediated immunity to foreign Ag
path – interstitial immunoblastic infiltrates w/ tubulitis (lymphocytes btw tubular epi cells w/in TBM), intimal vasculitis, interstitial edema
Chronic Transplant Nephropathy
timing – months to years
etiology
chronic rejection – end stage of acute rejection, characterized by effects of chronic ischemia
parenchyma loss & marked intimal thickening of large arteries
drug toxicity – cyclosporin causes vasoconstriction
chronic ischemic changes
hyperfiltration – reduction of renal mass
hypertrophy of remaining mass
recurrence – varying frequency
do novo dz
Developmental Pathology (Robbins pp. 459-471)
Concepts of Morphogenesis
Concept Definition Example
Malformation defect due to intrinsic process
Disruption defect due to extrinsic interference w/ originally nl process renal agenesis w/ no nephric development pulm stenosis following maternal rubella infxn
Deformation abnl form due to mechanical forces amputated digit following constriction by folds in amniotic membrane
Dysplasia
Sequence
Syndrome abnl organization of cells into tissue pattern of anomalies from single anomaly/mechanical factor pattern of related anomalies not known to be a sequence congenital adenomatoid malformation, cystic renal dysplasia oligohydramnios
renal agenesis
urethral atresia, bladder hypoplasia, clubbed foot, “Potter’s facies”, lung hypoplasia
Down syndrome
distinctive facies, congenital heart dz, musculoskeletal problems
Examples of Errors in Morphogenesis congenital adenomatoid malformation
distinctive mass in developing lung, represents dysplastic, hamartomatous, neoplastic growth in one lobe
detected on US as mass in lung, manifests as respiratory distress after birth
path – solid w/ few cysts to largely cystic
histo – multiple branched cuboidal or columnar epi-lined spaces resembling immature bronchioles
rx by surgery congenital diaphragmatic hernia
abd viscera enter thorax
mass effect crowds lungs
lung hypoplasia
small, immature lung & pulm HTN
rx by surgery cystic renal disorders
autosomal recessive polycystic kidney disease (infantile polycystic kidney disease)
presents during infancy as respiratory distress due to lung hypoplasia (rare in older pts, but may present then as renal failure, HTN)
dx by US – see very large reniform kidneys w/ tiny elongated cysts radiating outwards from renal pelvis
cysts may also be in liver, pancreas
autosomal dominant polycystic kidney disease (adult polycystic kidney disease)
presents in adults as renal failure, but now can be dx during development
path – kidneys enlarged by random cysts (grape-like clusters
bizarre kidney shapes)
histo – cysts lined by collecting duct-type epithelium w/ intervening parenchyma
liver cysts and/or berry aneurysms (Circle of Willis) present in 30% of cases
Intrauterine Infection of Fetus
pathogenesis of fetal infections
hematogenous spread (transplacental) – e.g., viruses, Listeria, T. palladium
from amniotic fluid following ascending cervical infxn – e.g., bacteria
through direct contact w/ vagina/cervix during delivery – e.g., HSV, HBV
barriers to intrauterine infections
maternal defenses – mucous membranes/secretions, placental villi, amniotic membranes/fluid
fetal defenses – skin, immune system (after 1 st trimester
Infection Syndromes of Fetuses and Neonates
transplacental route
disseminated infection w/ systemic consequences (e.g., syphillis)
growth retardation, disruption, fetal anemia w/ edema (fetal hydrops), precocious development of lymphoid system
in HIV, no neonatal syndrome (some membrane rupture, preemies), although some infants will develop AIDS
membranes – usually ruptured (usually due to infxn then leads to chorioamnionitis), are opaque, contain abundant PMNs
dx chorioamnionitis in mothers w/ fever and foul-smelling amniotic fluid
Acute Amniotic Infection Syndrome
chorioamnionitis (may lead to sepsis), funisitis (inflamed umbilical cord)
fetal lungs w/ exudate in airways (fetal pneumonia), fetal stomach containing exudate