Determinants of survival on dialysis population of Libya
advertisement

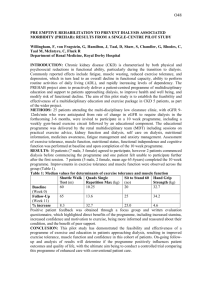
P104 DETERMINANTS OF SURVIVAL IN ADULT DIALYSIS PATIENTS IN LIBYA Alashek, W1, McIntyre, C1,2, Taal, M2 1 School of Graduate Entry Medicine, University of Nottingham, 2Department of Renal Medicine, Derby Hospitals NHS Foundation Trust INTRODUCTION: Maintenance dialysis sustains life for more than one million patients worldwide but is associated with substantially reduced survival when compared to the general population. Patient survival is an important outcome measure for dialysis because it is influenced by the quality of dialysis services. In Libya free access to dialysis has been provided for four decades but information about the outcomes of dialysis patients has not previously been published. A renal registry and national clinical practice guidelines for dialysis have not yet been established. This study therefore aimed to provide the first analysis of survival in Libyan dialysis patients. METHODS: This prospective multicentre, observational cohort included all patients in Libya who had been receiving dialysis for >90 days in June 2009. Socio-demographic and clinical data were collected upon enrolment using a structured data collection form. Survival status after 1 year was determined for all patients except those censored due to renal transplantation or lost to follow-up due to transfer to another dialysis unit. RESULTS: 2273 patients were enrolled for this study with a mean age of 48.7±15.5 years. Of these 67 received a kidney transplant, 46 were transferred to another dialysis unit where their status could not be confirmed and 1 recovered renal function. Thus 2159 patients were successfully followed up for 1 year. 458 deaths occurred, giving a crude annual mortality rate of 21.2%. 138 (30.1%) deaths were due to ischaemic heart disease, 73 (15.9%) due to cerebrovascular accidents and 74 (16.2%) due to infection. In 23% of cases, the cause of death was not determined. Annual mortality rate ranged from 0-70% in different dialysis centres. The best survival was in the age group 25-34 years. The mean age of those who survived was 9 years less than those who died. Those who survived had longer duration on dialysis, lower predialysis systolic blood pressure, more time on haemodialysis each week, higher haemoglobin and lower predialysis urea. A positive association was found between risk of death and diabetes, past history of cerebrovascular accidents, physical dependency and unplanned initiation of dialysis. Binary logistic regression analysis identified age at onset of dialysis, physical dependency, diabetes and predialysis urea as independent determinants of increased mortality (Table 1). Table 1: Independent risk factors for increased 1-year mortality in dialysis patients HR 95.0% CI P- value Age at onset (years) 1.037 1.027-1.047 <0.0001 Physically dependent 1.700 1.253-2.307 <0.0001 Diabetes 1.482 1.087-2.021 0.013 Predialysis urea 1.004 1.002-1.007 0.002 Hosmer and Lemeshow test of goodness of fit P- value =0.999; Nagelkerke R Squared=0.159 CONCLUSION: Patients receiving dialysis in Libya have a crude 1-year mortality rate similar to western countries but the mean age of the dialysis population is much lower than that in most western countries. As in most countries, cardiovascular disease was the most common cause of death, but infection was also an important cause. The large variation in mortality rates between different centres suggests that survival could be improved by transferring best practice from those centres with the best outcomes to those with poor survival. 1