Urine testing guide for the educator

Developed as a teaching aid to accompany
Residents of Aged Care Homes &Urine Testing Protocol
Produced by the North East Valley Division of General Practice 2006 www.nevdgp.org.au
Residents of Aged Care Homes &Urine Testing Protocol
Guide for the Educator
Introduction
This Guide for the Educator has been developed to support the
Residents of Aged Care Homes & Urine Testing Protocol developed by the North East Valley Division of General Practice.
Both the protocol & the Guide are informed by current evidence & discussion with clinicians.
Why review an area of clinical management?
The common goal of GPs and Aged Care Home staff is to provide medical care to residents that will improve their quality of life.
We rely on evidence from good quality clinical studies to guide our practice (and new studies come out all the time).
These studies provide:
Evidence that the symptoms and signs we are using in our clinical assessments are reliable
Evidence that the treatment we provide does more good than harm.
A Clinical Dilemma
Accurate diagnosis of urinary tract infection in residents of aged care facilities is not straightforward.
It requires a clinical judgment to be made based on a combination of symptoms, signs & investigation.
The medical practitioner’s decision to treat may have to be made without absolute certainty or proof.
Why review urine testing in particular?
Studies show high rates of Dipstick urinalysis & MSU testing occurs in aged care homes leading to:
Over-diagnosis of UTIs
Unnecessary antibiotic use
Medication related side effects
Resistant organisms
Excessive cost – ACH & GP staff time, pathology services, medication
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 1 of 9
KEY MESSAGES
Residents in aged care homes have high rates of
ABNORMAL DIPSTICK AND MSU RESULTS without infection necessarily being present
15-30% men 25-50% women in aged care homes have abnormal urine test but no UTI
NB the rate of urine infections in the residential aged care population IS higher than in the community, but you cannot base the diagnosis of an infection on the result of a urine test alone.
Diagnosis of a UTI in an aged care home resident requires a combination of
RELIABLE CLINICAL SIGNS & SYMPTOMS
+
POSITIVE MSU
The interpretation of symptoms, signs and urine test results in the aged care population is DIFFERENT from that of the general community
There is NO role for Dipstick Urine test as a screening test
ie Do not do a Dipstick test if the resident is not unwell
Think carefully before doing a dipstick test for an unwell resident also – how will I interpret the result? Would an MSU be better? Does this resident need a general clinical assessment by the GP?
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 2 of 9
Notes
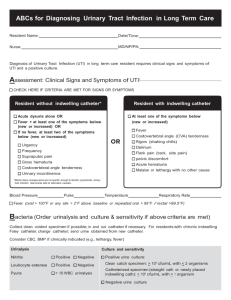
When would you test for a UTI?
Only test for a UTI when reliable symptoms & signs are present (these are symptoms & signs that have been shown in studies to be more likely to indicate a UTI)
What symptoms are most likely to suggest a UTI?
Dysuria
Frequent passing of urine or urge to pass urine
Bladder (low abdomen) or renal (loin) pain
New onset or worsening of incontinence
What symptoms MAY occur in the resident with a UTI but also occur as the result of other illness or infection?
general malaise
confusion
nausea &/or vomiting
haematuria
What signs are most likely to suggest a UTI?
None are reliably associated with UTI
In particular there is NO evidence to support cloudy urine or smelly urine as reliable signs of UTI
What signs MAY occur in the resident with a UTI but also occur as the result of other illness or infection?
Confusion (change in mental state)
Fever
Suprapubic tenderness
Loin tenderness
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 3 of 9
Notes
What test should I choose?
Is Dipstick urinalysis reliable? -NO
What does a Positive dipstick mean?
Positive for Leucocytes (pyuria, white cells)
can be produced by presence of bacteria, but may be contamination
is not always present when infection is present
poor correlation with UTI
Positive for Nitrites
Bacteria produce nitrites
Some bacteria do not produce nitrites
poor correlation with UTI
Bacteria may the cause of nitrites & leucocytes being present – but does this mean there is an infection??
What does a Negative dipstick mean?
A negative dipstick result strongly suggests there is NO UTI
HOWEVER even a negative dipstick result is not 100% reliable- so still suspect UTI if reliable symptoms present
Occasionally a GP may request a Dipstick test because a negative result MAY carry some weight, but in general AVOID DOING
DIPSTICK TESTING
IF A UTI IS SUSPECTED AN MSU SHOULD BE PERFORMED
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 4 of 9
How useful/reliable is an MSU?
Notes
How can you collect an MSU?
Is it possible in this population? rarely
Is a clean catch a suitable alternative? It may be all you can collect but is not as reliable as an MSU
How do you interpret the MSU Micro & Culture result?
Positive MSU and no symptoms = bacteriuria, not infection
(observe)
Positive MSU and symptoms = supports diagnosis of UTI (treat)
Note: there is debate about what constitutes a positive culture result in this population. Is it >10 8 or less? Does the presence of few versus lots of white cells influence interpretation?
Negative MSU - not a UTI
Sensitivities: useful to help choose correct antibiotic
Contaminated urine: bugs & skin cells present
How do you decide whether to treat for a UTI or not?
Notes
The diagnosis of UTI ultimately rests with clinical assessment. Clinical assessment means:
exclusion of other causes
collation of symptoms, signs & MSU result
Elderly patients with non-specific symptoms merit a full
clinical assessment (may include CXR, FBE etc)
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 5 of 9
When to treat a UTI?
Depends on the clinical condition- if the resident is mildly unwell then it may be appropriate to wait for the MSU result rather than initiate treatment while it is still unclear whether a UTI is present or not.
More on asymptomatic bacteriuria (MSU positive but no symptoms of UTI)
Is there any advantage to treating asymptomatic bacteriuria?
No evidence of prevention of future UTI no evidence of survival benefit no benefit in improving incontinence in resi care population
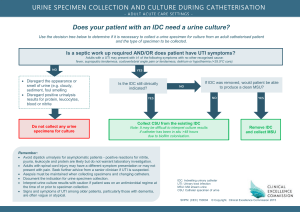
Patients with catheters
Bacteria will be present in the urine of ALL residents with a catheter
Cloudy urine is NOT indicative of UTI in someone with a catheter
To collect a meaningful urine specimen from the resident with an indwelling catheter (a CSU) it is necessary to change the catheter first
Treat with antibiotics only if clinical condition & CSU findings suggest UTI
In these patients loin pain & fever are significant indicators of a UTI
An example of the potential impact of implementing this
“protocol”
At one aged care home the records of 45 residents treated for
“UTIs” were analysed. These UTIs were diagnosed primarily with the use of dipstick testing. The analysis found that if the protocol (ie using MSU results & clinical assessment) had been applied only two residents would have been diagnosed as having a UTI.
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 6 of 9
Prevention
Why do the elderly get UTIs?
Notes
Many aged related changes contribute to the vulnerability of the elderly to UTIs
Post menopausal changes -quality of the tissues around the urethra poor
Poor bladder emptying (structural changes, functional changes)
General immune suppression (eg poor nutrition, presence of other illnesses, medications)
Reduced mobility, dementia
Notes
What can we do to prevent Urine infections?
Toileting
Hygiene
Hydration
Nutrition
Bowel
Other o Cranberry o Antibiotics, surgery, medication, oestrogen o Role of Ural etc
See next page for details
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 7 of 9
UTI Prevention – Details
Toileting
Regular visits to the toilet to minimise time spent in dirty or wet pad
Hygiene: bacteria usually enter via the urethra
Good management of incontinence of faeces
Prevention of maceration of skin from dampness
Continence Pads
Proper continence pads are made to draw urine away from the skin
Regular changing of pads important as
sitting in wet pad damages the skin & allows bacteria to enter
faecal soiling carries bacteria that may cause a urine infection
When dealing with faecal incontinence that has left only a small smear of faeces on the pad it may be appropriate to cover the area with a liner, but in general consider changing the pad.
Washing
If there is extensive faecal soiling, use toilet paper to clean the resident before washing. Use shower & soap (rather than sponging, as the water gets dirty)
Do NOT use talcum powder
As it makes the pad less absorptive and holds bacteria near the skin
Hydration – essential (minimum of 1000ml/day unless fluid restrictions in place)
Thirst drive is diminished in the elderly. Residents are often reliant on staff for prompts to drink.
Most people need about 1.5 L of fluid per day but more if the weather is hot, or if the resident has a fever
Less if fluid restriction order (eg residents with cardiac failure)
Nutrition – improves the body defences against all infections
Bowel – prevent & treat constipation
Other?
Cranberry juice/capsules? o Only proven to reduce rates of UTI in young women with recurrent E coli UTIs o Dose & frequency & form (juice or capsule) vary in all studies o Consider the calories & sugar load of juice
Daily antibiotics (if >3 Sx UTIs per year, but risk of resistance)
Fix bladder dysfunction (structural, functional)
Improve quality of tissues (oestrogen – some evidence helps stress incontinence, less evidence for UTI prevention)
urinary alkalinisers reduce symptoms (Ural, Atravescent, Citralite,
Citravescent, sodium bicarbonate, Uracol, Uricalm, Uricosal, Urocite-
K) .
They have no proven role in preventing UTIs & can interfere with antibiotic effectiveness
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 8 of 9
Illustration to explain Asymptomatic Bacteriuria
Male Urinary Tract
Female Urinary Tract
Guide for the Educator - Residents of Aged Care Homes &Urine Testing Protocol
Page 9 of 9